Abstract
Background/Purpose
Different researchers have studied pulpal calcifications and their connection with cardiovascular and systematic diseases. The study aims to test the prevalence of pulp stones in dental patients and determine the link between pulp stones and systemic diseases.
Materials and methods
One thousand and thirty patients from the Riyadh Elm University clinic participated in the experiment to test the correlation between pulp stones and cardiovascular diseases. The examination was conducted using digital radiographs. To determine the prevalence of pulp tones and their connection with cardiovascular diseases, pulp chamber images, and the canal were gathered using a digital radiograph instrument.
Results
The sample participants were categorized into two groups of medically fit and compromised patients. The results showed that pulp stones were significant for patients with cardiovascular diseases and diabetic Mellitus. The age variable significantly influenced pulp stones’ development. By implication, 81% of participants between 46 and 60 years were prone to have pulp stones. There was a significant difference in pulp stones development between male and female patients.
Conclusion
The outcome showed a significant relationship between cardiovascular diseases and pulp stones. Pulp stones prevalence is significantly higher among patients with systemic diseases, especially hypertension and diabetes mellitus.
Introduction
Pulp stones development is still a puzzle in medicine. The neurotic impact of aggravation by the microorganisms of dental caries causes decay, which deposits calcium salts within the tissues. Some predisposing factors include orthodontic tooth development, idiopathic and hereditary.
Table1: Summaries of previous works of literature.
Cardiovascular illnesses (CVDs) are diseases of the heart and veins. CVDs could be heart illnesses, heart attack, stroke, heart failure, arrhythmia, heart valve issues, coronary illness, cerebrovascular sickness, fringe blood vessel malady, rheumatic coronary illness, congenital diseases, or deep vein thrombosis and pulmonary embolism.5 The essential behavioral variables of coronary disease and stroke are undesirable eating regimens, physical idleness, tobacco use, and alcohol addiction. The impacts of these behavioral variables may appear in people as high circulatory strain, high blood glucose, high blood lipids, and overweight and obesity. Sound, emerging, and developed teeth can have pulp stones.6
A large portion of the teeth of teenagers and adults above fifty years old has pulp stones, which are presumably microscopic. Pulp stones formation might be related to long-standing aggravations, for example, caries, profound fillings, and interminable irritation. A few researchers recommend that pulp stones are a component of an aggravated pulp, trying to repair its tissues. Pulpal discomfort is one of the continuous side effects related to pulp stones.7,8,9 The pain may shift from soft to severe. They can cause an obstacle to the root trenches, which prompts endodontic failure. Calcification of dental pulp and calcific plaques may have similar pathogenesis, so the normal dental radiographs might be valuable to recognize proof of potential cardiovascular infections.10 Thus, oral and facial radiographs might be useful in screening cardiovascular infections.11
There have been works on pulp development and a systematic disease, however, these studies do not address the pathological connection with CVDs. The innovation of this study is to evaluate pulp stones and the symptoms of CVDs using digital radiographs. The analysis would be used to assess the connection between pulp stones and systemic disorders. This examination is additionally aimed at determining the pervasiveness of pulp stones with independent variables such as age, sexual orientation, and CVDs.
Materials and Methods
One thousand and thirty patients from Riyadh Elm University took part in the study to test the correlation between pulp stones and cardiovascular diseases. The inclusion criteria were patients with CVDs, diabetes mellitus, and age. The participants’ patients were subjected to panoramic, RVG radiography, and CBCT evaluation. The sample patients were divided into three groups, which include 15-30 years, 31-45 years, and 46–60 years. Patients were informed regarding the study and informed written consent was obtained. The research analyzed patients’ data such as age, sexual orientation, and CVDs.
The ethics committee approval was obtained for this study. The sample populations were divided into two major groups of medically fit and compromised patients. The study groups include Group I patients with cardiovascular diseases (including myocardial infarction, angina pectoris, heart disease, hypertension, and patients who had undergone heart surgery). Group II patients had diabetes mellitus. Group III patients had both cardiovascular diseases and diabetes mellitus. Group IV patients were used as the control group. Data obtained were tabulated and analyzed with the SPSS tool. Descriptive statistics were performed along with the Chi-square test with the value of significance kept under 0.05.
The test-retest technique measures external uniformity or agreement of an examination. The method describes the degree to which examiners provide coherent or uniform values of the same analysis or test. However, the intraobserver test assesses the level of uniformity among repeated observations or evaluations conducted by one researcher. The average pairwise percent agreement showed the coders had a 94.4% agreement. The examination had a Fleiss Kappa value of 0.88, which is excellent. The observed agreement was 0.94 while the expected agreement was 0.53. The Krippendorff’s Alpha for the analysis was 0.883, which is above Krippendorff’s benchmark of 0.800. The inter-observable test provided assurance and confidence in the study results.
Results
The results revealed that 48% of study participants from age group 15-30 years had pulp stones, whereas 73% and 81% of study participants had pulp stones belonging to age groups 31-45 years and 46-60 years respectively (Table 2). Table 2 shows the observed results on the distribution of pulp stones. The results revealed the highest and lowest values for pulp development across the age groups. Participants between 46 and 60 years developed pulp stones.
Consequently, patients between 15 and 30 years had the lowest pulp development. The likelihood of pulp development was higher in adults and lower in teenagers. Table 3 shows the prevalence of pulp stones based on tooth number and age. The probability of having pulp stones decreased with age across the sampled population. Table 4 showed the incidence of pulp stones based on sexual orientation. The analysis showed that male patients had a higher likelihood of pulp development. As a result, 69% of the male population had pulp development, while 62% of the female population had pulp stones. The results also showed the probability of not having a pulp stone.
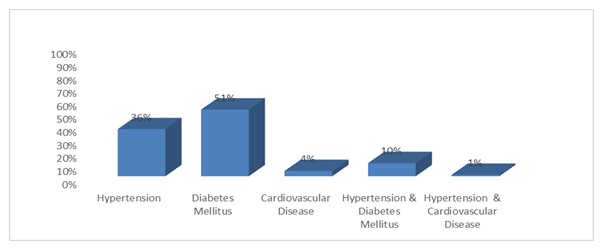
The likelihood of not having pulp development was higher in females and lower in male patients. Table 5 showed a comparison data of pulp stones based on individual teeth and sexual orientation. The research compared the p-value of male and female patients using their tooth numbers. Table 6 shows pulp stones development based on the patient’s health status. The result showed that 86% of medically compromised patients had pulp development, while 47% of sound patients developed pulp stones. Table 7 shows the distribution of pulp stones prevalence among individual teeth by a medical condition. There was a statistical significance between all the teeth except tooth numbers 27, 37, and 48 (p>0.05). Figure 1 shows the distribution of pulp stones among medically compromised patients. Over one-third, (36%) of patients with hypertension had pulp stones. The study revealed that 51% of patients with diabetes mellitus had pulp stones, and only 4% of patients with CVDs had pulp stones (figure 2). One-tenth (10%) of patients with hypertension and diabetes mellitus had pulp stones, and only 1% of study participants with hypertension and CVDs had pulp stones.
Table 2: Prevalence of pulp stones in different age subgroups.
Table 3: Prevalence of pulp stones in the individual tooth among the sample based on age group.
Table 4: Prevalence of pulp stones among males and females.
Table 5: Comparison of pulp stones prevalence among individual teeth based on gender.
Table 6: Prevalence of pulp stones based on medical condition.
Table 7: Comparison of pulp stones prevalence among individual teeth based on a medical condition.

Discussion
Most authors used different techniques in their examinations.13,14,15,16 One examination had demonstrated that there is no critical contrast with the system to distinguish the pulp stones. In this investigation, the digital radiograph was considered the best option. Edds et al.17 found a unique connection between pulp stones also, the nearness of arteriosclerosis and other cardiovascular diseases. The study recorded the occurrence of calcification in the pulp of atherosclerosis patients. The survey discovered calcification development in the extirpated dental pulp vessels in CVD patients. Nayak et al.12 in their investigation on the Indian populace discovered the pervasiveness of pulp stones in hypertensive patients was 15.85% higher than the value of medically sound patients. The present examination likewise demonstrated a higher prevalence of pulp stones in CVDs and diabetic patients when contrasted with the general development of pulp stones.
In this study, the outcome revealed that diabetic patients were distinguished with severe pulp stone development.18,19,20,21 The researchers inferred that calcification in angioplasties, thickened cellar layer were noted in both expansive and little veins, and vascular changes are articulated in the focal zone of the pulp.22,23,24,25 The study concluded that pulp calcifications in diabetic patients were frequent and sickle-molded.
In another study on dental pulps of diabetic patients, no vascular changes were found in the tissue.22 Indistinct calcified bodies in the pulp of diabetic patients were reported in the survey. The dental pulp of patients with diabetes mellitus ages rapidly because of endarteritis and poor blood circulation in the matured teeth. Dental radiographs require insignificant radiation, particularly advanced imaging innovation. The sensitivity of imaging instruments reduces radiation exposure from 10 to 40%. Digital radiographs were chosen to decide both coronal and radicular pulp stones. During this investigation, the size of pulp stones varied from little particles of calcified bodies to large masses that impede the pulp chamber.
This study suggests that patients with pulp stones have high susceptibility to develop diabetes mellitus and hypertension. Therefore, it is recommended that such patients should be screened to assess such complications at early stages. Further research is recommended to determine the causes of pulp stones formation. The findings of this research revealed the prevalence of pulp stones in aged patients. The outcome showed a significant relationship between pulp stones development and CVDs. Pulp stones prevalence is significantly higher among patients with systemic diseases, especially hypertension and diabetes mellitus. Consequently, pulp stones are prevalent among patients with CVDs and diabetes mellitus. The utilization of pulp stones in this part of the prescription may be upgraded if longitudinal examinations could affirm a connection between heart diseases and pulp stones development.
References
Swathy S, Gheena S, Sri VL. Prevalence of pulp stones in patients with history of cardiac diseases. Research J Pharm and Tech 2015;8:1625-628.
Bains K, Bhatia A, Singh P, Biswal S, Kanth S, Nalla S. Prevalence of coronal pulp stones and its relation with systemic disorders in Northern Indian Central Punjabi population. ISRN Dent 2014;617590.
Ezoddini-Ardakani F, Namayandeh SM, Sadrbafghi SM, et al. Diagnostic value of dental pulp stones in the early diagnosis of ischemic heart diseases. Health 2015;7:336-45.
Talla HV, Kommineni NK, Yalamancheli S, Avula JS, Chillakuru D. A study on pulp stones in a group of the population in Andhra Pradesh, India: an institutional study. J Conse Dent 2014;17:111-13.
Khojastepour L, Bronoosh P, Khosropanah S. Rahimi E. Can dental pulp calcification predict the risk of ischemic cardiovascular disease? J Dent 2013;10:456-60.
Feng X, Luo X, Li R, Dong W, Qi M. Multiple pulp stones: report of a case and literature review. Shanghai Journal of Stomatology 2015;24:511-2.
Gutmann J, Rigsby S, Endo C, Abe D. Meeting age old challenges in root canal procedures with contemporary technological assessments. ENDO (Lond Engl) 2015;9:107-10.
Turkal M, Tan E, Uzgur R, Hamidi M, Colak H, Uzgur Z. Incidence and distribution of pulp stones found in radiographic dental examination of adult Turkish dental patients. Ann Med Health Sci Res 2013;3:572-6.
Moudi E, Kazemi A, Madani Z, Haghanifar S, Moudi E. A radiographic correlation between the presence of pulp stones and kidney stones. Caspian Journal of Applied Sciences Research 2015;4:620-5.
Ertas T, Veli I, Akin M, Ertas H, Atici Y. Dental pulp stone formation during orthodontic treatment: a retrospective clinical follow-up study. Niger J Clin Pract 2017;20:37-42.
Neville B, Damm D, Allen C, Bouquot J, Neville B. Hematologic disorders. J Oral Maxillofac Pathol 2009;2:526-7.
Nayak M, Kumar J, Prasad K. A radiographic correlation between systemic disorders and pulp stones. Indian J Dent Res 2010;21:369-73.
Ranjitkar S, Taylor, J, Townsend G. A radiographic assessment of the prevalence of pulp stones in Australians. Aust Dent J 2002;47:36-40.
Goga R, Chandler N, Oginni A. Pulp stones: a review. Int Endontic J 2008;41:457-68.
Sisman Y, Aktan AM, Tarim-Ertas E, Ciftçi ME, Sekerci AE. The prevalence of pulp stones in a Turkish population: a radiographic survey. Med Oral Patol Oral Cir Bucal 2012;17:212-7.
Horsley SH, Beckstrom B, Clark SJ, Scheetz JP, Khan Z, Farman AG. Prevalence of carotid and pulp calcifications: A correlation using digital panoramic radiographs. Int J Comput Assist Radiol Surg 2009;4:169-73.
Edds AC, Walden JE, Scheetz JP, Goldsmith LJ, Drisko CL, Eleazer PD. Pilot study of correlation of pulp stones with cardiovascular disease. J Endod 2005;31:504-6.
Bender IB, Bender AB. Diabetes mellitus and the dental pulp. J Endod 2003;29:383-9.
Edds A, Walden J, Scheetz J, Goldsmith L, Drisko C, Eleazer P. Pilot study of correlation of pulp stones with cardiovascular disease. J Endod 2005;31:504-6.
Ezoddini-Ardakani F, Namayandeh SM, SadrBafghi SM, et al. Association of pulp stones with coronary artery stenosis. Community Dental Health 2011;XX:3.
Yeluri G, Kumar CA, Raghav N. Correlation of dental pulp stones, carotid artery and renal calcifications using digital panoramic radiography and ultrasonography. Contemp Clin Dent 2015;6:S147-51.
Nagaraj ST, Sinha P, Goswami RD, Veerabasaviah BT. A radiographic assessment of the prevalence of idiopathic pulp calcifications in permanent teeth: A retrospective radiographic study. J of Indian Of Oral Med & Radio 2014;26:248-52.
Ertas ET, Inci M, Ertas H, Yengil E, Sisman Y, Gokce C. A Radiographic correlation between renal and pulp stones. West Indian Med J 2015;63:620-25.
Vibhute NA, Vibhute AH, Daule RT, Bansal PP, Mahalle A. Hard facts about stones, pulpal calcifications: a review. J Pat Care 2016;2:105.
Hsieh C, Wu Y, Su C, et al. The prevalence and distribution of radiopaque, calcified pulp stones: a cone-beam computed tomography study in a Northern Taiwanese population. J Dent Sci 2018;13:138-44.