Abstract
This dissertation is about organisational development and the processes and methods in instituting it. Organisations regard change as new and disturbing. However, change is inevitable in almost all aspects of human life and even in other organisms. Change is significant in this time of intense globalisation and dominance of technology in almost all organisational functions.
The literature provided concepts and studies on organisational development. One significant fact is change is now “a regular feature for organisations” (Drummond-Hay & Bamford, 2009, p. 324). We looked into a specific case study to examine why change is necessary and conducted primary and secondary researches. The problem stemmed from one of the hospital’s departments, and that is the scheduling of outpatients in the radiology department.
Patients’ waiting time is one of the seemingly unresolved problems among healthcare providers these days. Government hospitals have faced this problem without instituting the necessary solution. This affects healthcare service, reduces patients’ satisfaction and exacerbates pain and suffering.
Organisational development (OD) was introduced in the hospital by installing a computer software for online booking system in the hospital’s ultrasound department. The change process used the Health Service Executive (HSE) model of change and the different stages involved. HSE was further analysed to find if there was a fit between the model’s requirements and the healthcare provider.
Outpatients agreed to participate in the study and were asked to fill in questionnaires. The study found that the number of outpatients who preferred online booking system was significant as this reduced patients’ wait time and increased their level of satisfaction.
Introduction
Introduction
It is a fact and a need for organisations to change in order to survive in this harsh time of intense competition and globalisation. Change is synonymous with development, and it should be a part of organisational strategy: every organism that has survived in the evolution changes like a thorny plant that evolves into a full-blown flower. We are not talking about evolution that takes place in an immeasurable time, since organisational change has to occur every minute, every second, in order to survive in this period of intense competition among organisations. We are talking of evolution, which is sudden and quick, an evolution that comes from within. Internal change is a factor of organisational development, which should be continuous and effective. An organisation that does not adopt to change will not survive in the competition, and will later fade without notice (McAuliffe, & Vaerenbergh, 2006).
Knowledge is significant in the context and study of organisations. We usually understand this as theoretical knowledge, but there are types of knowledge we call practical or that derived from experience, and skills knowledge. Knowledge is important in the globalising environment. Organisations conduct knowledge sharing as part of enhancing organisational knowledge, and because organisations need to grow through change. Just like human beings, they grow and change every now and then, and they have to accept this change as part of their existence. Knowledge management is a part of culture, and knowledge sharing should be a part and concept of delivering healthcare. Organisations need virtual teamwork to stay in the competition. This eliminates the vertical type of management and should become a regular process of management (Allee, 1997).
The literature tells us that existing knowledge combines with new knowledge through daily interactions of doctors, staff, and patients. This should also lead to formation of virtual teams, the process of which provides a gradual and effective program in which efficient and transformational leaders lead. They may be managers, physicians, staff, or ordinary employees of the hospital.
Robbins (2001) describes this present time as the “age of discontinuity” (p. 541), where the years past are not anymore extension of today and the future. Since the oil crisis in the 1970s, when oil prices continued to rise astronomically, and the beginning of the economic shocks, organisations have to continuously apply changes in their functions, strategies, and activities (Robbins, 2001).
Change is disturbing, and that is the reason why many people resist change. Managers and employees tend not to accept change because this will alter their normal course of activities. However, most change activities lead to organisational success (Kotter & Schlesinger, 2008). Many of those who resist are uninformed and lack the necessary skill. If they lack skill, then short-term training is an easy and quick solution. For example, the radiology staff, especially doctors in the hospital under study, did not have knowledge of online booking or scheduling of patients and they thought it would complicate their activities. A simple orientation seminar could have enlightened them. Online booking is a quick solution to a simple problem of patients’ waiting time. It involves a software wherein the physician would just input the names of the patient and the system provides the scheduling.
The situation in the hospital needed a little amount of effort from top management by purchasing the software. IT people would install the software and conduct the necessary tests, and doctors and outpatients should have information and knowledge about its use before it would become operational. The hospital in our case study is a government hospital in one of the bustling districts of the United Arab Emirates. Therefore, funding is no problem, along with the necessary skilled IT people. The radiology department did not have a systematic method of attending to its patients, who had to wait for long hours or days. Radiologists used the traditional manual booking and examination took time. There was prolonged treatment period, which delayed or hampered the curative stage of any illness.
Providing healthcare is not only a noble human endeavour but also one of the most important services health providers can deliver to individuals. Delivering healthcare involves improving the quality of life of people, requires the expertise of dedicated professionals and institutions, and needs planning and use of important resources and tools that include technology and computer software.
Inadequate healthcare delivery means lack of any one of those sources, which delays treatment and worsens suffering. A hospital is not only a healthcare provider but also a business organisation with the responsibility of providing customer satisfaction. Patient satisfaction should be a major goal and mission of healthcare providers.
Patients are like “customers” who deserve high-quality service or product. Dissatisfaction can result into customers looking for other providers. Customer satisfaction, which is meeting the needs and wants of customers, is essential in this age of stiff competition among business organisations.
A significant undertaking in providing effective healthcare is reducing patients’ waiting time. Examples of patients’ wait time include wait time before a doctor can provide check up, wait time before undergoing ultrasound or x-ray, and other similar situations. A waiting patient experiences more pain and suffering. If healthcare service is inadequate, patients feel neglect from their government, if the hospital is a government facility. Government doctors, administrators, and private practitioners also feel they are inefficient, when in truth they are victims of an ineffective old system, or maybe lack of effective management system.
This research paper is about organisational development. Any change applied to an organisation involves significant OD. In particular, this is about modifying a system in a hospital so that attending physicians, nurses, and radiologists, can effectively deliver healthcare to a great number of outpatients, without having them wait for long time before they receive healthcare. Patients’ waiting time is one of the growing problems of hospitals, particularly government hospitals. Patients have to wait for the long line before the doctor examines them. A simple problem of ultrasound scheduling allows patients to wait before they receive treatment or given prescription by a government physician. This has become a pain-in-the-neck of hospital administrators, who serve large populations.
Change and innovation in the hospital is significant and necessary. Top management and its staff and all the other stakeholders should accept it like a gift, and deliver the intended change like a gift and a responsibility, because it would improve the quality of life of many patients who need the radiology facility anytime. Change will enhance organisational performance and improve healthcare service. In particular, change needs the application of computer software to address the problem of ultrasound scheduling.
The recommended change was for the doctor to schedule the patients’ ultrasound appointment through the system so that the patients would not anymore go to the radiology department for scheduling. This would reduce the waiting time, crowdedness in the radiology department, and workload of radiology staff, and increase patient satisfaction.
Evaluation and discussion at the near-end of this dissertation will explain the reasons why this is so, by means of a thorough discussion of the literature and from the results of the primary research, which provided the respondents’ answers to the questionnaire.
Organisational context
Organisational development was applied to a hospital in Bur Dubai, which is under the jurisdiction of the Ministry of Health in Dubai of the United Arab Emirates. The hospital has several specialised clinics and departments, all focused for healthcare and control and prevention of diseases in the Bur Dubai district, which has a multi-ethnic and multi-cultural population.
The hospital addresses the health problems of the population, and for all age groups. It caters to in-patients and outpatients, whatever sicknesses they have, and since this is a government hospital, the costs of hospitalisation are minimal while some are being addressed to by the government agency concerned.
The hospital has a staff of 150 Doctors, 6 Radiologists and 15 radiographers in addition to a number of administrative employees and nurses. It receives patients with or without appointments, which causes disruption to the regular flow of services and annoyance to doctors, nurses, and staff. The maximum number of patients treated every month is 1,888, and the radiology department is one of the busiest departments in the hospital. This means that there has to be a systematic type of scheduling of services for patients.
While this research stressed on organisational development, this will also expound on the role of organisations in delivering high-quality healthcare and in meeting the needs and wants of patients, who must receive service like customers waiting for high-quality product or service.
This research used an organisational change model to introduce an effective organisational development, the Health Service Executive (HSE) model, which aims to provide high-quality health service for all people, including the most vulnerable members of society.
Rationale
Technology dominates human activities. There is no human and organisational activity, which do not take advantage of the use of technology, in particular, information technology (IT) and the Internet. These are used to provide communication and rapid operations and processing of tasks and functions among organisations, whether for business or for non-profit, and even individual tasks. Organisations utilise computer software that speeds up various departmental functions. In the hospital under study, some functions were still not computerised, or the staff did not use a software, particularly in booking patients who needed ultrasound. This was an opportune time for the staff to use IT since the hospital already had the IT infrastructure to give way for the installation of the online booking software.
Moreover, hospital staff to include physicians and nurses should know how to work on the software that will allow computerised scheduling. This process is a change from the hospital’s ordinary course of activities. Doctors and staff must not resist this change because change is a part of organisational development that benefits the patients, the hospital management and staff, and those working to improve the quality of life of the patients. They are not working for or serving an organisation, but they are serving the patients. They exist not for themselves but for people in the community.
Aim and objectives
Aim
The aim is to study and apply an online booking system for ultrasound appointment for outpatients of the hospital. This will further provide an analysis of the situations before and after the application of the online booking system.
Objectives
- To reduce waiting time for outpatients of the radiology department of the aforementioned hospital
-
- To determine the effectiveness of online booking system in the radiology department of the hospital
- To enhance customer satisfaction of patients
Hypothesis
Software application of an online booking system will reduce patients’ wait time, improve the service of the ultrasound/radiology department, enhance high-quality healthcare, and improve quality of life of the people.
Role of the student in the organisation and project
This is a part of the responsibilities of students, to research from the literature the theories and applications of organisational development. Additionally, we have the responsibility as citizens and as human beings who should look after our fellow human beings, improve quality of life, and make the world a wonderful place to live in. Part of this advocacy is to help in the delivery of healthcare for patients and those in need of help. We should also advocate the Health Service Executive (HSE) principles and its approach to organisational development, which is the delivery of high-quality healthcare.
The organisation that we introduced change is a hospital in the Dubai. They have an IT infrastructure and they only needed a computer software that would introduce a system of online booking for outpatients of the radiology department. My role here was to help motivate the staff in the change process, facilitate the online booking system and orient the participants on the advantages of the system. During the administration of the questionnaire, this Researcher sent emails to the prospective participants. The radiologists were interviewed regarding their feedback of the change process and their opinion of the applied change. All these were recorded and became part of this dissertation.
Quality healthcare must be available for all, in particular the ordinary folks of the country, the disadvantaged and the most vulnerable sector of society. We use the HSE model in pursuing organisational development because the approach and the principles, as explained in the Methodology chapter, focus on every member of society, in particular the less fortunate and the most vulnerable. Our background and vision as individuals are for the promotion of health of ordinary people, people in the countryside who do not have access to healthcare, and people like our folks who have given us life and the philosophy that has built us up as rational human beings.
Summary and Conclusion
This section provides background for the research, which emphasised organisational development of a hospital that focuses on delivering high quality healthcare to its thousands of patients. Delivering quality healthcare is a primary responsibility of the government.
The research recommended the use of online booking for ultrasound patients to reduce their waiting time. Organisations have to continuously provide innovations in order to improve their service. Change is a continuous process in organisations, as without change organisations become stagnant. Many organisation members resist change because it disturbs their normal course of activities. We recommended the use of online booking system wherein the attending physician would just input the names of patients scheduled for ultrasound, and the system would schedule the patients’ appointment in the radiology department. This would reduce waiting time and increase customer satisfaction. This study used primary and secondary research in the application of organisational development on a government hospital.
Review of the Related Literature
Introduction
Patient satisfaction is dependent on factors related to: 1) level of care acquired; 2) empathy; 3) reliability; and 4) responsiveness. Other related factors that will affect feedback are: 1) physician conduct; 2) efficiency; and 3) service availability. The present study focuses on the importance of service availability and the process of change. Therefore, it is important to highlight the fact that service availability is linked to waiting times, convenience, and availability associated with health care experiences (Naidu, 2009). Wait time is an important consideration not only in the health sector, but also in organisations that are labelled as service companies. It is widely accepted within the corporate world that organisations worry about the length of their queues because customer waiting time can negatively affect customer feedback regarding the performance of the company. Business leaders also fear the possibility of losing clients if waiting time is too long (Bielen & Demoulin, 2007).
Bottlenecks, long queue lines and unnecessary waiting time are always associated with low productivity (Naidu, 2009). These issues are also associated with unnecessary expenses (Barrick, 2009). In the context of the health care industry, patients, and various stakeholders are sensitive to the impact of delays in the delivery of related services (Gijo et al., 2013). From the point of view of patients, the unnecessary delays negatively affect productivity (Taner et al., 2012). For example, employees have very limited time when it comes to securing a doctor’s appointment (Keilar et al., 2010). Employees are compelled to file a request in advance (Kohn, 2011). In some cases, they need to request a leave of absence. For such reasons, patients cannot afford delays in the delivery of health care services (Bielen & Demoulin, 2007).
In most cases, employees try to squeeze in the time to visit health clinics and hospitals during lunch breaks. Prolonged stay in a primary health care facility requires more time, and in this case, patients may have to spend a whole day away from work. The patient seeking to avail the services of the radiology department expects to receive quality service during a specific time period (Atinga et al., 2011). Patients in a primary health care facility expect a particular standard when it comes to treatments and diagnostics protocols (Willoughby et al., 2010). Without a doubt, it is disadvantageous to the patients if they are unable to avail of the services required during the time that they requested the same (Miller & Chalapati, 2015).
Inconvenienced clients are not going to be pleased with the delays (Gunderman & Sawlani, 2012). Nevertheless, this is the best case scenario in the aftermath of long queue lines and unnecessary delays. In the worst case scenario, unnecessary delays lead to health risks and other vulnerabilities (Greaves et al., 2013). Managers of primary health care facilities that are not equipped with appropriate technologies to deal with delay problems are compelled to manage the backlogs through a wait list. However, in areas where the wait list is no longer a viable solution, a phenomenon called “queue jumping” occurs. According to observations made regarding the ill-effects of queue jumping, administrators lament the fact that in hospitals the scarcity of resources created severe consequences. As a result, people were compelled to save themselves, and those who are close to them. They were compelled to intervene in behalf of patients, friends, or family, and they ignored those who were not known to them (Cunningham et al., 2013). This is not an unacceptable practice because it will lead to unnecessary conflicts that will further reduce the quality of health care services in the hospital.
In order to solve management issues related to unnecessary “wait time” in Dubai hospital, this study attempts to analyse the related literature regarding the reduction of wait time through Information Technology or computer software.
Search Strategy
The aforementioned objectives demand the framework for the search strategy. The focus is on related literature that discussed the significance of wait time in the context of the health care industry. The search strategy narrows down the search for literature that discussed the impact of wait time in the radiology department and other related needs (Gunderman & Sawlani, 2012). However, the search for related literature expands to include the use of Information Technology in reducing wait time (Cunningham et al., 2013). Inclusion of research materials was based on how IT was utilised in the health care setting. It also includes the search for literature that illuminated recent inventions, and innovations linked to the improvement in the delivery of health care services, particularly in the context of reducing wait time (Westbrook, 2007).
Review of Themes
The search framework explained the thematic type of inquiry into literatures that are relevant to the topic. These are listed as follows: 1) The significance of wait time reduction; 2) Innovations in the field of Information Technology with regard to improving health care delivery systems; and 3) The problems inherent to the application of Information Technology to reduce wait time in a health care facility setting.
The Significance of Wait Time Reduction
According to an educational perspective on wait time in the radiology department, the patients that went through the scanning equipment spent considerable time in the waiting room. Yet this phenomenon and the waiting experience are matters that health experts did not give much thought, because these issues were not addressed in the curricula of most medical schools (Gunderman & Sawlani, 2012).
The end result of reducing wait time in terms of health care delivery systems is enhanced client satisfaction (Naidu, 2009). Enhanced satisfaction is a guaranteed by-product from the point of view of patients and other stakeholders (Cunningham et al., 2013). Wait time reduction also eliminates or mitigates the impact of health risks in connection with the failure in the delivery of certain health care services (Willoughby et al., 2010). In some studies on early diagnosis and early prevention strategies, there are certain steps in the health diagnostic protocol that are very critical to proper diagnosis and management of patients’ health care needs. Therefore, it is very essential that relevant data must be collected as fast as possible, in order to decrease the report generation time, and improve the overall process (Gijo et al., 2013). Radiology departments under Dubai hospitals will experience tremendous improvement in client satisfaction if the managers of the health care facilities are able to reduce wait time for patients requiring radiology procedures.
Innovations in the field of Information Technology in Health Care Delivery
Health care facility managers must consider the feedback from patients and other stakeholders (Blackley et al., 2012). Clients of the hospital directly affect the financial health of the said institution. It is for the best interest of hospital management to improve customer satisfaction, particularly in the area of health care delivery systems (Greaves et al., 2013). Succeeding revelations regarding the issue of wait time reduction will reveal the link between the financial capability of a specific health care facility and its capacity to invest in IT-related technologies (Miller & Chalapati, 2015). Therefore, there is a certain degree of symbiosis between improving health care services, and the ability to further improve the same (Lodge & Bamford, 2007).
Before going any further, it is important to point out that the need to reduce wait time using technology is not a novel contribution to the study of health care management (Zabada et al., 2001). As early as two decades earlier, health care facility administrators voiced out their concerns regarding delays in health care delivery (Hart, 1995). They also commented on the possible impact of using IT to address the problem of delays and long que lines (Kovner & Knickman, 2011). However, the application of technology was not made in such a way that an IT solution was created to directly solve the problem. The application of technology was not done in such a way to efficiently gather information regarding the said issue. The end goal was the integration of detailed statistical data creates strategies for improved health care delivery (Hart, 1995). In the 21st century, the end goal must go beyond the analysis of data. It must end up in the creation of a viable IT solution based on the current population’s access to computers and their ability to use the same. As early as a decade ago, technology was used to address the problem of service availability. But nothing concrete was created to specifically design an IT-based solution that will speed up the process of registration and scheduling health care delivery.
More often than not, the staff who enter data that are used to determine wait times, the data they create as they interact with triage, the patient registration process and medical record systems, the same trickle down into the federal and accountability domain, and the information play a role in significant policy debates (Westbrook, 2007). The focus of conventional strategies to use IT-based solutions was to assist administrators manage data related to health care delivery, but these were not specifically designed to reduce wait time (Kohn, 2011). Hospital administrators in Dubai must move beyond the conventional use of Information Technology, and develop an online booking system to lower backlogs with regards to the number of patients requiring imaging services as a requirement for their respective medical diagnostic needs.
One of the primary issues related to long queue lines is the inability of hospital administrators to anticipate the influx of patients demanding access for a specific type of health care service within a specific time period. The apparent solution is a two-fold process. First, hospital management must anticipate the number of patients coming in at a particular time of the day, and the specific needs that require a particular type of service. Second, hospital management must develop a system of scheduling to effectively manage the influx of patients on a given time schedule.
A report on efficiency issues provided by Miller and Chalapati (2015) related to human resource scarcity, provided the following observations:
- The management of human resources was a critical waste in terms of resource management in the said health care facility;
- However, it was a secondary issue with regards to the patient waiting time;
- The main issue was the inability of the health care facility to control patient arrivals.
With the existence of a mechanism to see patient appointments, the facility was able to identify patients that required specific care and call the attention of junior doctors so that they could better manage the flow (Miller & Chalapati, 2015).
In a study designed to determine the impact of IT solutions to the radiology department of a primary health care facility, the researchers made the following conclusion, the Computerised Radiology Information System (“CRIS”) allowed health workers to use computers for encoding patient details and relevant information such as request card. This is visible to the staff at all sites, enabling health workers to track patients. Related procedures in terms of the need for review and authorisation can be finalised and recorded. As a result, printed information no longer need to move from one area to the next. There is no need to move hard copies of files from the reception desk to the radiologist’s tray. This reduces delays. In addition, the Picture Archiving and Communication System “(PACS”) allows scanned images to be accessed in different sites. This is a time saving mechanism (Greaves et al, 2013).
The innovative solution called CRIS is good news for Dubai hospitals administrators interested in creating an online booking system to manage patient flow. This means that the hospital does not have to start from scratch. The IT-based solutions generated from studying the implementation of the CRIS system will provide a wealth of information that also serves as a template for developing systems specifically designed for Dubai hospitals.
Even the most sophisticated IT infrastructure and IT software cannot resolve the human resource aspect of the problem. It has to be made clear that the success of a particular management initiative is affected by several factors, such as, the numerous challenges in terms of resource management. In many hospitals, health care workers are very busy and operating at a relentless pace with not enough breaks. Thus, hospital administrators must realise the importance of commitment to the task at hand (Willoughby et al., 2010).
An online booking system is an example of an IT-based solution that reduces waiting time due to the efficiency of transmitting pertinent information regarding patient’s needs. Nevertheless, an IT-based solution must be complimented with other management strategies that effectively reduce wait time due to the removal of blockades to efficient patient flow.
The following strategies were documented as effective improvements to a radiology department’s management program: 1) Improve the efficiency of the scanners, such as, the acquisition of scanners that utilises faster and less redundant sequences; 2) improve the efficiency and quality of machines so that old machines must be replaced with new ones; 3) improving patient flow and throughput, such as insertion of intravenous access sites in advance, and outpatients are made to change into gowns in a timely manner; 4) at the other end of the booking process are clerks responsible for informing patients regarding the specific time of scheduled scans, it is imperative to hire clerks working in night shifts to improve the communication process between the health care facility and its respective patients; and 5) the need for efficient signing off of final reports by radiologists (Keilar et al., 2010).
Additionally, hospital management must consider other components of the work flow process that significantly affects the length of time needed to complete a particular task. In a study that combined manufacturing management theories with health care management principles in the context of radiology examinations, the proponents of the study remarked on the typical inefficiencies in a normal work flow process. More often than not, the radiology department suffers from examination repeats. These are byproducts of inefficiencies. Even after investing in the latest equipment, many radiology units are still struggling with the impact of human errors. Valuable resources are wasted due to the misinterpretation of the images by radiologists. Hospital administrators must combine management techniques with information technology to optimise patient flow for greater efficiency and better clinical outcomes (Taner et al., 2012).
Effective management strategies coupled with practical steps to improve the health care delivery systems are needed to reduce wait time. Administrators of radiology departments in Dubai hospitals must go beyond the conventional use of technology for the sake of recording data. It is imperative to develop IT-based solutions like an online booking system for patients requiring the use of the facilities under the control of the radiology department.
Inherent Problems in the Application of IT in order to Reduce Wait Time
It is not enough to simply acquire new technology in order to solve a particular problem. According to a report of a study that examined the value of improving patient flow, the significant findings from the Flow Cost Quality Programme were the technical insights into service design alone. These are not sufficient to achieve meaningful change. If hospital administrators aim to acquire more radical benefits by giving first priority to optimising flow, it is on how they approach change and the organisational context where they are assured of a satisfactory outcome (Blackley et al., 2012).
A project management team must be created to collect relevant information regarding wait time in the context of the radiology department in a particular health care facility in Dubai. After collecting critical information needed to design an appropriate solution to the given problem, the project team manager must begin mapping out the implementation phase of the project.
An unexpected outcome of an IT solution is to create a dehumanising effect on health care delivery. According to the study on patients’ perspective regarding wait time, one must consider the size, complexity, and technological sophistication of health care facilities, because it has the power to dehumanise both patients and health workers. It must be made clear that every patient wants to be seen and treated as a human being, and not just a mere statistic (Gunderman & Sawlani, 2012). Thus, it is not enough to simply develop powerful IT-based solutions. Hospital administrators must enhance the delivery process taking into consideration the need for empathy and demonstration of genuine care for the patient’s quick recovery.
A major problem encountered by administrators during the implementation phase of a management initiative to establish IT-based solutions for a given problem is the lack of support from stakeholders or the flawed design of the system because of the failure to consult stakeholders. After the challenges confronting the patients were identified, the first stage of the implementation process was the identification of the primary stakeholders in the health care process. The first stage of the analysis revealed interrelated factors comprising a complex health care system. Researchers discovered the presence of internal stakeholders, such as, doctors, health care staff, and patients. They also discovered that the opinions of internal stakeholders were often times in conflict with external stakeholders, such as, regulators, politicians, and investors. In addition, the two groups of stakeholders had different perspectives when it comes to the definition of value and waste (Miller & Chalapati, 2015).
The failure to consult stakeholders leads to the unexpected creation of roadblocks. In a study made on the importance of collaboration in the implementation of organisational change, researchers discovered that in many cases, the need to change the system was perceived negatively. They also said that changes were only possible when the carefully developed change programs has the approval of internal stakeholders (Lodge & Bamford, 2007). Administrators of health care facilities in Dubai must study the expected conflicts in the context of implementing change or changing the culture of a particular workplace.
Another unexpected consequence of developing IT-based solutions is the discovery that the use of cutting-edge technology is a costly endeavour that does not guarantee an acceptable return on investment. According to one report, there is proof that IT-based solutions do lower costs. However, those savings are not always delivered to the organisation that made the investment (Kovner & Knickman, 2011). This is a challenge for hospital administrators that are answerable to the hospital’s board of directors or the investors that established the said health care facility.
Implications for the Project
The review of literature revealed the significance of reducing wait time. It is clear that unnecessary delays and service unavailability is a cause for client dissatisfaction. If the health care facility in Dubai is viewed as a profit center, then, it is imperative to ensure cash flow. Profitability based on positive earnings is only possible if the administrators are able to sustain reliable and efficient health care delivery systems. One of the problematic areas is the utilisation of the equipment under the radiology department.
Aside from the prospect of a failed business operation, the incentive to solve long que lines and unnecessary delays in service delivery is also rooted in the need to mitigate the impact of unethical behavior of health workers due to the pressure created by an unmanageable wait list system.
It is interesting to note that IT-based solutions in the past were geared towards the administrative functions of managers. In other words, computers and other computer-related equipment were acquired and utilised to help managers control the recording and accessibility of data. The main purpose of the data collection was not to speed up the work flow process, but to use the information to develop hospital policies. The policies that were developed were not always related to the reduction of wait time. Most of the policies were created to help reduce expenses and increase profitability. It is important to point out the insight regarding the lack of information regarding the nature of wait time in the radiology department. It is interesting to highlight the fact that colleges and universities are focused on other aspects of the health care process. But the plight of the patients that were forced to endure unnecessary delays is not always in the forefront of discussions and management decisions.
It is also important to highlight the fact that the mere creation of an online booking system is not enough to solve the problem. One of the critical components of the project design and implementation is the need to consult stakeholders, and the need to secure the support of influential leaders within the workplace. If an influential leader was not persuaded to support the need to implement specific change, such as the use of a new management system, it would be difficult to encourage other health workers and key personnel to seriously consider learning the intricacies of the new system.
The failure of implementing change programs is usually due to the failure in the design. It is imperative to consider the feedback of patients, physicians, and other stakeholders to develop an appropriate IT-based solution that is both practical and functional. It is impractical to spend resources in developing a solution that is difficult to implement and difficult to manage.
Another critical aspect in the creation of an online booking system is the inherent challenges when it comes to Information Technology. IT infrastructures are expensive to upgrade or overhaul. The most problematic aspect of the cost of establishing IT-based solutions to reduce wait time is the fact that IT-related software and tools are made obsolete in a matter of months or a few years. There is also the problem of spending additional resources for regular upgrades. The prohibitive costs pile up when administrators consider the need to train users regarding the intricacies of new technology
It is not enough to develop a system that is easy to use in a hospital setting. The online booking system must be accessible to outpatients. In addition, the designer must consider the need for creating a system that is accessible through mobile gadgets.
Finally, the hospital administrator must consider the return on investment. It is prudent to develop a business model that will enable the hospital to enhance its revenue stream in order to sustain the new online booking scheme. Furthermore, the said hospital administrator must consider other aspects of the work flow process in order to reduce wait time. The patient’s ability to communicate their needs is just part of the solution. The other aspect to the solution strategy is the availability of resources. Therefore, it is also important to reduce the work load of health workers by eliminating unnecessary repeats.
Summary and Conclusions
It is not enough to simply develop a solution to reduce wait time. It is also important to consider the requirements and consequences of developing an online booking system to improve patient flow. A project manager must be empowered to gather the necessary information and develop an implementation strategy that considers all the different aspects needed to ensure success.
The critical aspect to the implementation strategy is not only the capability to develop practical and functional IT-based solution to reducing wait time. It must also consider the capability to pool resources in order to finance the implementation process. It is therefore prudent to use available information with regards to the successful use of similar technologies. Dubai’s hospital administrators are not required to build from scratch. The successful implementation of online booking systems in the Western world are useful in developing an IT-based solution that will solve the challenges of wait time reduction in the context of Dubai’s health care sector.
Aside from developing the online booking system, hospital administrators must look into the implementation of other strategies that will help reduce wait time. Thus, management strategies adopted from the manufacturing sector such lean management strategies and Six Sigma management strategies must be utilised to look into the inefficiencies within the patient flow process. Hospital administrators must examine the other aspects of the health care delivery system, specifically with regards to the needs of the radiology department. For example, an efficient inventory program must take control of some aspects of the management system of the radiology department in order to reduce breakdowns and unnecessary delays due to equipment failure. It is also important to reduce the need to repeat certain processes. Aside from changes applied to the technical aspect of the health care delivery system, the project manager must also look into the human resource aspect of the project as well.
Methodology and Methods
Introduction
This section provides a description of the methods and techniques used in the dissertation, on how the research reached this point where an online booking system was needed to be introduced in the hospital, as well as the methods of recruiting the participants, the gathering of information and data from the participants and the development of the questionnaire.
We usually refer the activities in this section as those which answer the questions what and how: what was done and how was it done? The organisational change is a significant activity and the method of change is a process that occupies most of the contents in the chapters we have formulated and the chapters that contain the evaluation and the concluding parts.
Methodology
This study used qualitative and quantitative research, employing primary and secondary techniques of study. Primary research is about using interviews and questionnaires, while secondary research involved review of the literature and about works done in the past. Through questionnaires and interviews, researchers collect primary data, which are considered fresh and original because they come directly from respondents who are knowledgeable of the issues. Secondary data are those already gathered and statistically analysed, using dissertation tools (Kothari, 2004, p. 95). In this study, we used a combination of secondary and primary research to gather data and provided a critical analysis using both data. The technique is a combination of the two, which was quite challenging but it produced a new set of ideas and knowledge that can be useful for further research.
Quantitative research involves relationship. In this research, we are concerned with the number of outpatients who responded that their patient satisfaction increased with the application of OD, which specifically the online booking system.
Primary research consists of evaluating how the patients, the main beneficiary of the organisational change, felt about the existing problem in the radiology department of the hospital. The sample was taken from a population of outpatients and radiologists of the hospital. The organisation, including the doctors, nurses and staff, also comprised as part of the beneficiaries of the change: they were a part of the change but they helped in making the change take place.
Researchers cannot define the world through what they merely see and perceive, but also through what and how the respondents see and feel of the world around them (Oliver, 2012, p. 144). Therefore, we can classify this study as ethnographic research, which is a way of knowing what the respondents understand and view of the world around them. This is very important in the organisational change we were trying to apply to a hospital and in providing high-quality healthcare.
The literature review discussed in chapter 2 focused on previous works of accomplished authors and researchers about patients’ wait time and computer software, which could be used in online booking system for the ultrasound section of the hospital. Analysis and disadvantages were made regarding the use of manual booking, and the advantages that can be derived through online booking, which makes use of a software and the internet to connect with patients. The software also allows physician and patient interaction, in which the patients will have complete knowledge about his/her sickness.
How the survey was conducted
This Researcher sent a total of 500 letter-requests to outpatients of the hospital. This was not done at the same time because the survey was conducted in two phases: the first phase was conducted when the hospital was still using manual booking (the old system), and the second phase was conducted when the hospital was already using online booking system (the new system).
Since it was a two-phase activity, we first sent 225 letter-requests to outpatients whose names appeared in the list of outpatients scheduled for ultrasound. Of the 225 letters sent, only 220 got a positive response, meaning they were the first set of participants who were to participate in the survey while manual booking was still in effect. After this first activity, when the first sample took time to answer the questions, the hospital implemented the online booking system for the outpatients. A team of IT personnel installed the computer software, and inputted all the necessary data and information and connected this online. We were one of those who requested for the application of an online booking system, but we knew the hospital was already taking steps for such implementation.
This time, this Researcher sent the second set of letter-requests to another set of participants, in which out of the 225 letters sent, 221 got a positive response. The total number of participants for the first and second phases of the survey was 481. On the other hand, the radiologists took and answered the survey questionnaires when the online booking was already in effect. In other words, they had a different experience as they witnessed the advantages and disadvantages of both manual and online booking systems (the old and new systems). The questions focused on the feelings and complaints (dissatisfaction) of the patients before the implementation of the change, and their reaction (satisfaction) after the doctors and staff of the radiology department implemented the change. Themes or variables emerged from the questionnaire and these are explained below.
The second set of participants was recruited and contacted only after the first set of participants have had participated in the survey and when the online booking system was already in effect. The mechanics were not explained to the participants and to the radiologists, but they knew that an online booking system was to be implemented after the manual system. This can be explained through a diagram below.
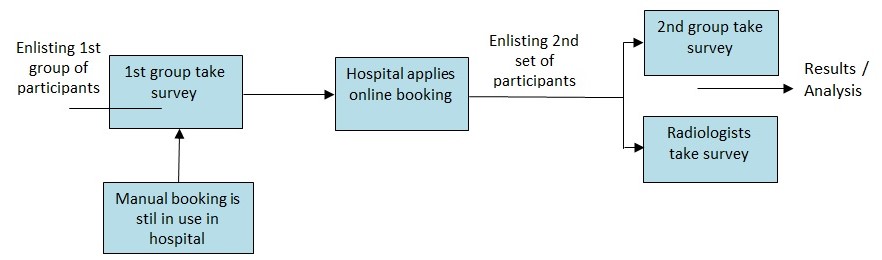
Using two groups in the survey allowed us to compare their experiences without the one experiencing both activities. Moreover, if we used only one group of patients to experience the old and the new systems of booking for ultrasound, that will not be realistic. For example, if 200 outpatients were to be scheduled for ultrasound using the manual booking of scheduling, they could not anymore be used for ultrasound for the second time (using online booking system) because by then if some got well in the treatment and it would be difficult to contact them. We could not submit patients to undertake another ultrasound for the same sickness or for the sake of studying the two methods of ultra sound scheduling. We had to apply the method of change in accordance with what was actually happening in the hospital. By having two sets of participants, we could draw their responses to the questionnaires. The first and second groups have had different experiences and the first experience did not affect the second experience, but we could compare them.
I informed the participants that the results and all information about the survey would be for academic purposes, and these would be integrated into a database with a username and password only I had access. We afforded necessary respect to the participants’ opinion and comments and informed them that there was no right or wrong answer. Their opinions and ideas were not to be judged, but were valuable to the academic community and future research. This research also afforded the necessary ethical considerations, such as respect for human rights of all involved in the survey.
Online booking means the attending physician will input the names of outpatients and the system itself will provide the scheduling. It also allowed patients to view the schedules of ultrasound and x-ray, give them time to ask questions to their doctors, and give them a chance for a patient-doctor online interaction. This is the first of its kind for the radiology department of the hospital to have such a technology, although the hospital’s website had long been in effect. The website also helps in hospital-patient interaction.
When the software was installed, the names of the 221 participants (the second set out of 481 participants) in the survey were integrated into the system and scheduling of ultrasound. By connecting the software online, scheduling became visible to all patients, but only individually. This means if one were scheduled for ultrasound, he/she sees his/her name in the list who will undergo ultrasound, including the date and time, but they could not see the names of other patients as this is confidential, per program of the computer software. The patients could also ask questions and express their views and complaints in the website.
Critical Review of Approaches to Organisational Development
The Principles of The Transformation Programme 2007-2010
The principles used in “The Transformation Programme 2007-2010” are key features in the approach to organisational development. This acts as guide in the organisation’s impetus for change, which focuses on the patients and the health providers. As we figured it out in the introduction, change is a compulsion to make service better. Quality is not just a feature of Health Service Executive (HSE), because it also delivers “care, comfort, support, expertise, help, hope, encouragement, protection,” and much more, to clients and patients (Health service executive, 2010, p. 7).
What could be more encouraging when an organisation enhances the lives of people in the community? It pictures service in the truest sense of the word. While population is growing in the UK and elsewhere, more and more people are also encouraged to work in healthcare.
The organisation’s vision can be summarised into a few key themes:
- quick and trouble-free access to “high quality care” (Health service executive, 2010, p. 9)
- faith in health and social care delivered by the organisation
- recognition of the staff’s fundamental role
- pride that the staff feels in their role and what they do to make life better for others (Health service executive, 2010, p. 9).
In summary, an organisation’s performance standards and measures of success are “easy access, confidence and staff pride” (Health service executive, 2010, p. 9). This is about vision and goals, and “The Transformation Programme” motivated this to happen to organisations it has promoted. We do not only look forward and are not merely hopeful, but are certain that this would happen to the outpatient programs hospital under study.
The challenge of using limited resources for the greater number of people is a principle of economics that has become in parallel, or synonymous, with the principle of HSE; it is encouraging, adequate and accurate. In the history of humanity, there has never been an exact amount of resources for a particular population. It even goes with the family – resources are also scarce for the family, and the head of the family must be skilful enough to make the limited resources meet the needs of the family, no matter how big. There is always scarcity around. HSE’s model is more challenging than providing for the population needs – and in the initial stage you feel that it is difficult to accomplish – because it is about fulfilling the needs with high-quality service. Organisations and people within organisations may ask, “If it is difficult, why should we do it? Why do we have to do it?” Another may think and say, “How could we do it in the healthcare service? How do we make our community happy?”
Precisely, we do it because it makes people happy. That is why it is challenging. In the HSE model, we find that there are solutions provided to future problems. HSE finds teamwork important. Teamwork is one of the most innovative solutions to problems in organisational development (OD). Difficult and impossible tasks are accomplished with teamworking. This is implicit in the HSE application.
Healthcare providers have to work with effective teamwork to provide high-quality service. Physicians and nurses, health workers in the clinic and those performing fieldwork have to coordinate their efforts so that they can provide high-quality health service, or their treatment activities might not be successful. The term “high quality” is stressed in this model; meaning it is not just quality, it has to be high that can enhance happiness and improve quality of life of even “the least of our brethren,” to quote a passage of a very important Book. The Transformation Programme’s vision also helps in finding the right direction and stimulates focus on the projects and practices to make organisations stick to their mission and manage resources properly.
The organisational development (OD) for the hospital under study can use the Transformation Programme’s six priorities (Health service executive, 2010, p. 11), as we highly recommend it.
- An integrated service for the different phases of the care process
- Arrangement of major, community care to deliver maximum service to all
- Arrangement of hospital services to provide cost effective healthcare
- Implementation of a method to prevent and manage chronic disease
- Provide benchmarks for performance measurement and management in the chosen organisation
- Motivate all staff to provide quality health care service
These six priorities can give us a glimpse (and a conclusion) of how focused the organisation should be in providing high quality healthcare. As the maxim goes, “we should not falter and we should not be weak in order to win”. Indeed, in seeking to implement high-quality healthcare, we are looking for perfection. Failure is for the weak. The barriers and problems along the way can be addressed when the boat reaches there. Meanwhile, measures have to be installed to deal with future problems, although there are no problems that will remain unsolved if the team stays focused and united.
In the context of the HSE perspective, the organisation has to employ all resources and personnel for the implementation of projects. The OD under study will have to get everyone’s cooperation to provide strength. “Everyone” refers to the staff, doctors, nurses and all “crew” in the radiology department and the IT people who will implement the online booking system, to include the outpatients in the ultrasound section of the hospital and their own families. Teamworking in the change process is demonstrated in figure 2 below.
Another approach to organisational development is to develop a partnership agreement among the various stakeholders to ensure a smooth flow of the change involved. The agreements provide general considerations requiring a united effort to improve efficiencies in healthcare service. As stated earlier, collaboration is a must in the application of change. Written partnership will improve this collaboration. In other words, this will seek allegiance from the stakeholders. While this is commendable, it is a new approach to the application. Will top management accept this approach, and will the patients understand the meaning of partnership? There are doubts regarding the written partnership among the stakeholders, as provided in the approach. For all we know, the patients are only up to having treatment and having a little comfort in their present physical state. The purpose of written partnership is to get the commitment of the stakeholders, in particular the patients.
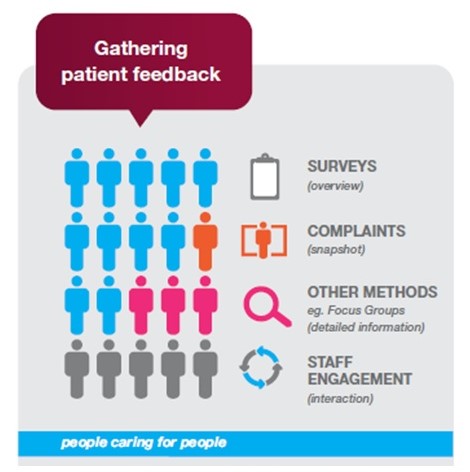
Using patient feedback is a model approach to enhance the organisation’s system of helping the patients (see figure 2 above). Patient feedback is important to improve the data for needs assessment, understand patient feelings when in contact with health providers, and know results of care (National Healthcare Charter, n.d., p. 4). Using patient feedback is sometimes not acceptable for people who do not want to hear negative comments. It is understandable because human nature tends to prefer to receive positive comments than negative ones. However, in the healthcare profession this is significant in improvement of service.
Patients always have reason to complain. A little pain will add to their discomfort, and they have many things to complain about in terms of healthcare delivery. Healthcare providers know and understand these complaints, the minor and major complaints, and they know how to eradicate the discomfort. Merely asking for their feedback can give some “peace of mind”. On the part of the healthcare providers, in particular the hospital, this will greatly improve their service. A few hospitals do this, asking patients how they could improve their service. However, if we want high-quality delivery of service, it is high time that all hospitals and healthcare providers, government or private, do it for the sake of the patients.
Rationale for OD Model Selected
We have selected the Health Service Executive (HSE) model as a model of change because it is applicable for large and small organisations, in particular the hospital setting. The model has a practical solution in providing health services. In Ireland, the model has centred its services on patients for high high-quality healthcare (HSE, 2013).
HSE is not just a framework for change; rather, it details the activities that organisations can use in the process of change. Instituting change is not an easy activity for organisations, in particular healthcare institutions. It requires careful planning, educated people to introduce the change, a knowledge base to help the staff and in the implementation of change, and technology. Absence of any one of these factors will affect organisational development and the success of the proposed change. A collaborative effort from the various stakeholders is important.
Moreover, we have selected this model because we see its significance to organisations and to our organisational culture. We find this adaptable to our cultural setting. An organisation trying to apply it can modify the model to suit it to their culture, and even improve it.
HSE: The Organisational Model
The whole concept of this model refers to a cycle: the first step goes to the second, and the third, and when it reaches the last step, it goes back to the leadership concept again. Stakeholders have to continually implement and improve the change, as the cycle implies.
The HSE model involves several stages, categorised into: initiation, planning, mainstreaming, and implementation (see figure 3 below). This is a model because other healthcare organisations also use it as benchmark to improve their service, and it introduces logical but effective steps in the process of change.

Initiation
In the initiation stage, we have “to prepare to lead the change,” (Health Service Executive, 2008) and lead by example, which entails working out several other steps to carry out the change. There are activities and characteristics in leading by example, as demonstrated in the figure above. This is known as the leadership role, which involves not just the individual but the entire group who must work as a team and be a leader for the intended change. In leading to introduce the change, there are other underlying steps and sub-steps.
As leaders, we must create a vision for our organisation. Healthcare professionals and workers work for people and they belong to an organisation where they share their goals and vision with other healthcare providers. They must focus on the people, the service users, those in the community who need help, the patients and common folks who need healthcare.
Leaders have to connect with the stakeholders and those in the community. A significant characteristic required of this change is relentless communication, which involves talking and asking everyone about the service they need and the things to do to make an effective change. Relentlessness communication connotes persistence in communicating with services users, in asking for what they need to make them contented with what providers can offer.
HSE can also be introduced to a multicultural setting. Healthcare providers should know the cultural sensitivities of people. Treatment cannot be effective if the patient does not believe in what physicians and nurses are doing. There are two kinds of culture that people in an organisation have to cope with: the organisational culture and the culture of the people in the community. The hospital or clinic has its own organisational culture. When change is introduced in the hospital, the culture might be influenced with the process of change. The introduction of an online booking system can affect the processes, such as the way the doctor talks and deals with the patients. Since the doctor is not used to online booking system, he/she might get confused in the ultrasound scheduling. So does the patient, who does not know internet browsing, or communicating through “chat” in the internet. The internet and online booking can effect change, but in the initial stage, this might create confusion and difficulty on the part of them patients.
Finally, an important aspect of the HSE model is that health professionals and workers should understand that they do not know everything and they need to continuously improve their knowledge and expertise in providing healthcare. Continuous learning is a necessity in the age of globalisation. Activities involving continuous learning include internal and external ones. Employees have to learn organisational knowledge, like what organisational culture can offer. Enhancement of skills can also be obtained internally. Additionally, organisations have to send their employees to training or educational institutions to learn new skills and concepts that can improve their current work.
Planning
First, why is there a need for a plan? What is it for? This has a specific purpose, which is to have a detailed picture of the change and to acquire support. This will give an assurance that there will be collaboration among the people, who will provide their strength and resources for the organisation’s objectives.
In the planning stage, we look for commitment. Change has to be a commitment, not just a passing activity. We have to build commitment from people, workers and staff, and top management down to service users.
Then, we have to determine what the features of this change are. Since we are dealing with an IT software, the change has got to be a bit complicated, because IT professionals, or organisation, might be involved to be a part of the implementing agency to effect the change.
To find out the possibility for successful change and to counter any resistance for change we must know how people should work out the plan for change. HSE shows the factors significant in the change process. Team members and every available stakeholder should help in planning and in attaining readiness and confidence for the attainment of an effective change.
There are activities for self-assessment, wherein the team and the stakeholders test their readiness and ability in attaining change, for example, degree of awareness and of “self-understanding for the vision for change,” and similar other readiness tests. Stakeholders are asked to choose from a scale of “high,” “medium,” or “low,” as to their understanding of “readiness” and “capacity” for change. This type of self-assessment is benchmarking, which is effective in measuring organisational performance.
Health providers should also work fast and provide a sense of urgency in order to effect the change. Kotter (2008) indicates that a successful change has a certain pattern and leaders who want to cause change must create a sense of urgency. Managers can create a sense of urgency by bringing “the outside in”. This means that people inside the organisation have to reconnect with the external world because they tend to be disconnected with the outside environment. Leaders must also send employees out to know what is going on in the external environment. In times of crisis, leaders should be able to seek opportunities. After determining the change, we have to develop an implementation plan.
Implementation
This focuses on putting into action what has been planned so that the objective can be attained. It is important to inform the stakeholders that the plan has been agreed upon and that this is put into action. Implementation is the stage wherein what has been the subject of discussions and planning are now put into practice. Implementation will involve the putting into action the details of the plan, but the change itself will have its own way. In other words, the introduction of a computer software that will provide online booking system will have its own different plan.
Providing every possible means and resource to effect the change will make it a successful endeavour. The model needs team working to be worked out by people delivering healthcare. Healthcare workers working in their individualistic attitudes will not produce good results. All organisations, especially those providing healthcare, must work in this manner. In the fields or within their clinics, doctors, nurses, and their assistants must work in a systematic manner, with efficiency and collaboration, meaning with effective teamwork, so that service users will understand their sickness and will cooperate in the process of treatment. If the team can do this, patients would like to become part of the team. The result is effective treatment and cure.
Development of the implementation plan involves consultation among the members of the team and all possible stakeholders. The change now is ready for implementation, and while it is ongoing, all involved have to maintain the momentum.
The process in the introduction of change is like treating a patient, which has to work out in different stages. This can be explained further with the chart provided in figure 4.
Like treating a patient, the team has to provide diagnosis. First, what type of change should be introduced. Next is what context of change, meaning, the team should know the circumstances and situation why change is necessary. The culture web in the first stage is essential, which means what organizational culture will be affected in the change process, and how will this be dealt with. Another is forcefield analysis, wherein the team should correlate the change with the situation and how will the entire change affect organisational performance.
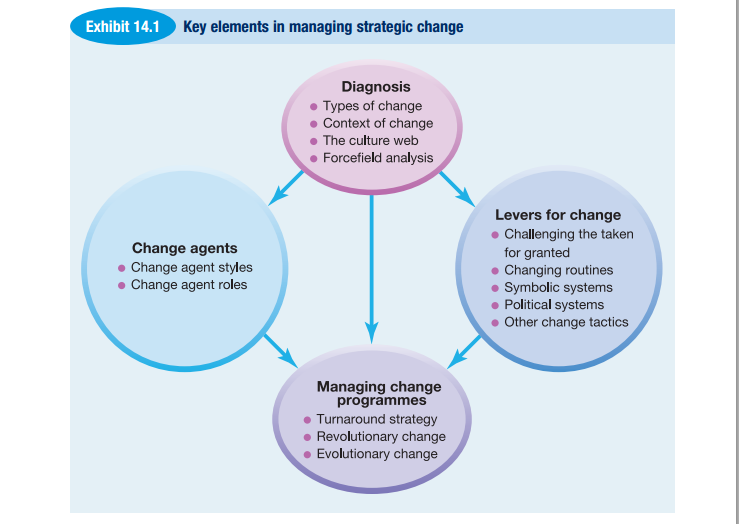
From the diagnosis context, we go to another stage of the process, which is “change agents”. This part focuses on styles and roles. Styles refer to speed and the way change is implemented. Roles of team members are also emphasised. For example, the role of attending physician, the nurses, the staff in the ultrasound section, and the IT people who should teach and orient those involved in the change process.
Mainstreaming
Mainstreaming is aimed at acquiring awareness on the ongoing change process and how this can be successfully attained. This will also involve looking for mechanisms and assessments of the ongoing activities and continual improvement. Mainstreaming focuses on evaluation and learning. Members learn from others, while each member tries to enrich the knowledge and learning of fellow members.
The levers for change include activities for people who seemed not included in the change process, but are really a part of it. They are those taken for granted, the patients maybe who seemed not involved but are the main beneficiaries in the change process. Levers for change also include changing routines when the change is already in place; symbolic systems, that pertains to the hospital’s culture that has to be changed; political systems that may be a part of the culture that has to be changed, and other change styles.
Managing change is also another stage from the diagnosis part. These are programs that refer to the change itself that can lead to a turnaround strategy. It can considered revolutionary because it is drastic and will involve change in the system itself, and it can also be evolutionary.
Theories of change
The HSE model evolved from other theories, although as stated earlier, this is now commonly used. Theorists promulgated concepts to create effective change through a series of actions. The theories of Kanter et al. (1992), Kotter (1996), and Luecke (2003 as cited in Barnard & Stoll, 2010) are herein compared to produce results. This is demonstrated in the table below.
Table 1: A comparison of the different theories of change
Evaluation
Introduction
This section will provide an analysis of the primary research conducted on the hospital’s outpatients and staff of the ultrasound section. The aim of this chapter is to determine how the aim in providing OD to the hospital was accomplished. This will also find out the advantages of online booking system for ultrasound appointment, the steps taken in meeting the aim, and the results of the primary research. The computer software provided in the literature review can give us a picture of how this can enhance organisational development (OD) and provide a number of benefits for the patients. The study used HSE organisational model in the process of applying the change, which is the introduction of an online booking system to reduce patients’ wait time in the ultrasound section.
In order to fulfil the aim and objectives of this dissertation, this research used literature review and questionnaire surveys and interviews. The literature review provided background on OD, the process of change, and the technology to for the ultrasound section of the radiology department of the hospital. Literature is effective because we can draw knowledge from theories and from primary research, which have already been statistically and critically analysed. Through this set of knowledge, this present study can provide a comparison from new ideas and knowledge drawn from primary research.
Out of the 500 request letters, 481 responded, with a response rate of 96 percent. All 15 staff members of the radiology department responded and gave their consent to be part of the survey research, making the response rate, with respect to the staff of the radiology department, to 100 percent.
The respondents’ cooperation was significant in the conduct of the research. This factor is one of the principles of the HSE model, i.e. drawing the participation and partnership of the patients, who are important stakeholders of OD. The participants were informed that the survey was confidential in nature; their names would not be made public; and the study was for the improvement and development of the hospital and its functions, and the outpatients of the hospital. In other words, OD was used to provide high-quality healthcare and enhanced customer satisfaction.
Significance of Healthcare Evaluation
Healthcare evaluation enables an organisation to adopt to change. Without this evaluation, OD cannot be effective and the different priorities that we have to implement in order to deliver high-quality health care cannot be realised. We have to use resources and knowledgeable personnel in implementing the HSE model, and get the cooperation of the doctors, nurses and the staff in the radiology department in introducing the change.
Evaluation
We evaluated how online booking enhanced organisational change, affected healthcare, and improved ultrasound scheduling of outpatients of the hospital. Literature review and primary research were used in which a sample of 481 outpatients and 15 staff members of the ultrasound section of the radiology department responded to questions from questionnaires and interviews. Evaluation had to be conducted step by step, or in a gradual manner so as not to skip some small but important items in the change process.
Results
There were 7 questions for the outpatients before the implementation and 7 questions after the implementation of online booking, which means each group of participants had 7 questions each to answer. Nine questions were directed for the radiologists who answered the questionnaires after the implementation of online booking system. The questions were converted into themes or variables during the analysis and in order to construct tables and graphs.
Questions were closed and open-ended questions. Closed questions were answerable by “yes or no,” while open-ended questions required a short opinion or comment (maximum 3-4 lines) from the respondents. Questions were provided in Arabic, but a translation in English was also provided. We made sure that the respondents understood the questions and we knew they did because they answered most of the questions. Consolidation of the responses was quite taxing and laborious because of the large number of respondents. However, we conducted an indepth analysis of the answers as to the respondents feelings and reactions regarding the hospital’s system, before and after the application of an online booking system.
Then a second set of questions were directed to all groups of participants, including the radiologists, and instructed them to rate the sentences using the five-point Likert scale: “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree”. This was in addition to the separate questions for the first and second groups, and for the radiologists, as listed in the questionnaire. These sentences are the following:
- We wait for days to get an appointment.
- Patients are crowded and wait outside the radiology section.
- Treatment is effective.
- Workload is organized and effective.
- Patients’ wait time is reduced.
- Treatment does not take time.
In analysing the respondents’ answers to the open-ended questions, we categorised their responses into themes. For example, the second question asked about patient satisfaction, in which the participants provided several sentences. Some comments referred to a theme, or variable, like “reduced patient’s wait time,” which means that answers of several participants referred to that theme. There were several themes produced out of the participants’ answers to the questions.
The aim of dividing the participants into two groups was to draw different opinions from two groups of people with different experiences: one group experienced manual booking, and thus they experienced longer waiting time; another group experienced the application of online booking, which led to reduced waiting time.
The first question dealt on demographic, like age and educational attainment of the first set of respondents who answered the questionnaire before the implementation of online booking system. This question had to be asked again for the second set of respondents who answered the questions in the course of the implementation of the online booking system.
The responses of the participants give us an overview of what has been happening at the hospital, in particular the outpatient department and the ultrasound section. This organisation was really in need of change, and we had this right timing. The first set of participants provided negative opinion and comments of what was going on: outpatients were spending more time waiting and had to go to the radiology department for scheduling. The situation exacerbates their predicament and worsens their sickness because they exert more effort and have to wait before being subjected to ultrasound or x-ray. Patients were not provided enough information about their sicknesses because they did not have time to ask as the doctors were in a hurry to attend to the long line of patients.
The second set of participants, who answered the questionnaires when the online booking had already been implemented, gave positive responses and all praised the new system, although they could not compare the new system from the old system because it was presumed that they did not experience the manual booking of ultrasound patients. Change gave them satisfaction.
We have to compare two scenarios here: one with no online booking system and one that has. The second scenario involved change and it was a positive OD. Change is advantageous for the organisation. Our concept of OD and the model we used applied in the organisation enabled a good change for the hospital – to move forward and be competitive. As discussed in the introduction, change is a part of any organisation and it cannot survive if it does not know how to adjust to change.
Results summary for Q1 – Age and educational attainment for the first set of participants
Table 2: Response rate for demographic of partici
(Before the implementation of online booking system)
Q1 had two questions addressed in the demographic – age and educational attainment, as this was necessary because online booking and browsing over the internet needs a little amount of education. Age is also necessary in knowing the opinion of the young and old generations.
There were five age groups: 1) 21-25 year-old; 2) 26-30 year-old; 3) 31-35 year-old; 4) 36-45 year-old; and 5) 46 years and above (see figure 5). The first groups was composed of 48 participants, the second 41, the third 51, the fourth 56, and the fifth 44 participants. From the different age demographics, there were 67 elementary undergraduate, 53 elementary graduate, 46 high school undergraduate, 49 high school graduate, and 24 college level participants, in respect to their educational attainment.
The second question dealt directly on factors affecting patient satisfaction. This type of question was addressed to the outpatients and the radiologists. The aim was to draw the opinion of the different sets of participants. In order to measure this type of question, we had to categorize the responses into themes. The themes are enumerated in table 3.
Table 3 is a classification of themes that emerged from the questions. Answer options in table 3 refer to the themes or variables that emerged from the questions in the questionnaire. For instance, the theme or variable “reduced wait time” refers to questions 3, 4, 10, 15, 17, 19, 21, 22, which the participants responded to positively.
Majority of the participants (n=136 or 28%) were of the opinion that reduced wait time was a significant factor that affected patient satisfaction. This means that 136 (or 28% of 481) from the first and second group of participants responded that reduced wait time increased patient satisfaction. The second factor that enhanced patient satisfaction is improved radiology facility, which is also correlated with reduced wait time. Reduced pain and suffering came next, and doctors’ and nurses’ efficiency both attained minimal scores. We can state here that, per results of the survey, the themes “reduced wait time,” “improved radiology facility,” and “reduced pain and suffering” were the factors that increased patients’ satisfaction the most.
The number of responses for reduced “waiting time,” “improved radiology facility,” and “reduced pain and suffering” is significant. Majority of the participants gave weight to “reduced wait time” as a factor that can give patient satisfaction (refer to figure 6). This can be drawn from their responses.
Excerpts of patients’ responses on “reduced wait time”
There were many responses on the issue of “reduced wait time,” and the causes of patients’ wait time, considering that this was the main issue of the survey and the problem posed by the research and the staff of the hospital to the participants. The interviews conducted provided many insights, which were recorded but could not be cited all here for lack of space. A few of the important comments are provided below.
“Yes, reducing my wait time as patient can help the healing process and improve my situation.”
“Wait time is really a problem. This should be the main focus of this government hospital. I should have my ultrasound right away so that the doctor can prescribe my medicine, but it takes time before I can avail of the ultrasound facility.”
“It matters if we have to wait before the doctor or any health provider can provide treatment. But I am really dissatisfied with the doctor or the hospital if they cannot provide prescription because they have to wait for my ultrasound results.”
“We have to wait before the radiology department gives us an appointment. Before we can be accommodated, we still have to walk and go to the radiology department. This is a waste of time for us who have other appointments or job to do.”
“I do get sick more after I spend a lot of time in front of the doctor, or if I have to exert a lot of effort.”
“It helps if wait time is reduced, but the doctor can do nothing because she has to wait for the results of the ultrasound.”
“Health providers should reduce my pain. If I have to walk from the outpatient department to the radiology department for scheduling and wait for the ultrasound and results, this will exacerbate my suffering. I should have access to your facility now because I need treatment now. But that is not what is happening. How can I have satisfaction?”
“I only get satisfaction if I can rest the whole day. I don’t want this service of allowing me to wait for hours.”
“This hospital has added more to my sickness by letting me wait for hours before I get my schedule. I am dissatisfied with their service.”
“Sometimes, I have to wait for the whole day before I get my schedule.”
“There are so many patients, with only one ultrasound machine, and the scheduling really takes time.”
“I have to come back the next day before I get my schedule, and I have to walk from the clinic to the ultrasound before I end the process. It is like a punishment to me. The doctor takes pity on my situation but she can do nothing.”
Excerpts of patients’ responses for “reduced pain and suffering”
“I am satisfied if my doctor examines and treats me right away, so I can go home, take my medicine, and rest for as long as I want until I get well.”
“The staff should do something to alleviate my suffering, not exacerbate it.”
Excerpts of responses for “improve radiology facility”
“The radiology department should do something to improve their service before we talk about satisfaction.”
“The only way to provide satisfaction for the patients is to provide another ultrasound machine so that many patients will be accommodated at the same time.”
Excerpts of patients’ responses for “doctor’s efficiency”
“Quick diagnosis and treatment from my doctor will give me satisfaction.”
“Rapid treatment and letting me go home after the doctor give me treatment and prescription will give me satisfaction.”
Excerpts of patients’ suggestions to improve healthcare
“Let the doctor do his job quickly and without giving problem to the patients. Allowing the patients to wait can add more problems than treatment.”
“Scheduling of ultrasound and all the hospital should do to help me alleviate my pain and suffering.”
“Perhaps, you can apply some new technology to make your service faster and effective. I’ve heard of this online booking and I think it can help. However, the patients should be informed, or someone should explain the matter so that patients will know what to do.”
“There is a long waiting list for patients before the doctor checks the patients. Wait time does not only apply to the radiology department; there are many outpatients the doctors have to check. The hospital should hire more doctors.”
“Technicians conducting ultrasound for patients must be careful in order to avoid accidents. Sometimes, in their haste to accommodate many patients, accidents occur. More staff should be added to conduct the ultrasound.”
“The only way to help patients is to hire more doctors and improve the facilities of the hospital. They should also add ultrasound clinics.”
The second set of participants who experienced the implementation of online booking system gave positive comments about the system. The attending physicians, staff and radiologists of the hospital supported the views and positive comments regarding the new system. The comments after the implementation of the online booking system are categorised in table 4.
Table 4 Categorised Overall comments regarding the new system (Participants (n=221) provided several comments, and this explains the response count to be over 221.)
Table 4 is about the staff’s positive reaction for the new booking system. The staff’s rating for reduced wait time is 27%, which means 61 (27% of 220).
The percentage shown in table 4 above reflects the satisfaction rate of the participants.
Comparison of Patient Satisfaction
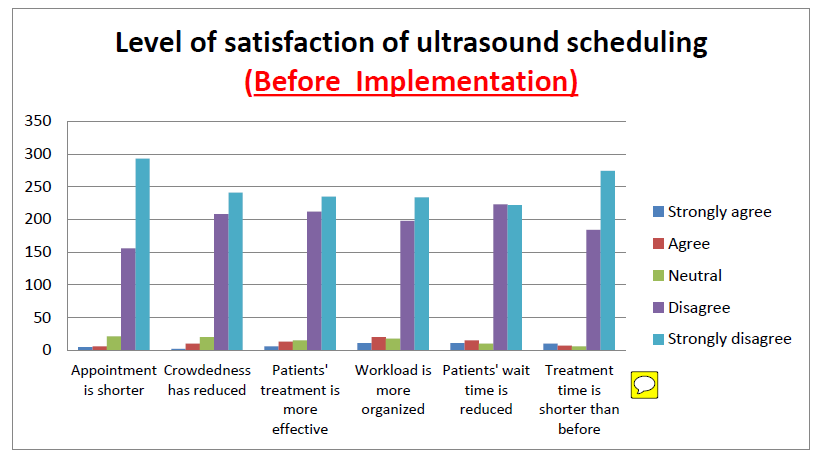
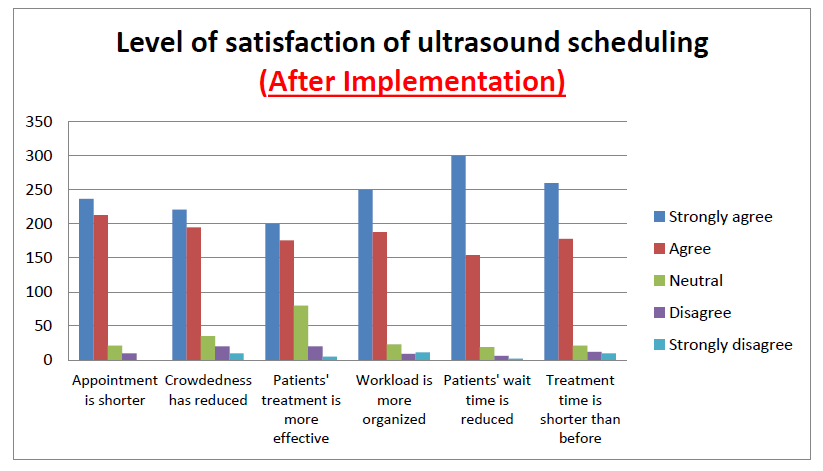
The two groups participants and the radiologists were asked to rate the following sentences from a five-point Likert scale: “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree”. This is in addition to the questions listed in the questionnaire.
- We wait for days to get an appointment.
- Patients are crowded and wait outside the radiology section.
- Treatment is effective.
- Workload is organized and effective.
- Patients’ wait time is reduced.
- Treatment does not take time.
Summary and Conclusion
In this chapter, we gave an indepth analysis and evaluation of the aim of the dissertation, which was the application of an online booking system, and the results of the instrument which is the submission of questionnaires to the participants.
The primary research used questionnaires submitted to 481 outpatients and 15 staff members or radiologists of the radiology department of the hospital. There were two sets of participants employed in the survey because the research had to determine the opinion of two sets of people: one who experienced without online booking and another who experienced online booking. We could not use only one set of participants to experience manual booking and online booking because if we were to apply this, we had to maintain communication with the same patients. If patients were to get well after they had had ultrasound, they would not be available again for another ultrasound. In other words, they would not need another ultrasound if they got well of their illnesses. So, it was better to have two sets of participants.
On the other hand, the second set of participants experienced reduced waiting time and increased patient satisfaction when online booking system was introduced. This registered when they answered to rate the method of scheduling from a 5-point Likert scale.
They were satisfied with their health service provider, and provided many positive comments regarding this technology application. They now have time to ask questions through the hospital’s website. The organisational change was conducted thoroughly with the help of the HSE service model.
Discussion and Conclusions
Introduction
This study correlated the literature review with the primary research. First, the literature review provided vast amount of knowledge on the importance of change and organisational development (OD), which is a significant undertaking in this period in history where organisations in almost all fields of human endeavour are mushrooming. Change is for strategic advantage and survival at the same time. Other topics in the literature included the adoption of change, which has to be a continual process, the different models, and the various reactions and impact to change.
The literature also provided background on the software to be used in the change process. Online booking system for ultrasound patients is available from a company that programs processes according to an organisation’s need. It was the responsibility of the hospital management to look into and make available such software. In truth, there was no problem with this because there were IT people who provided a feasibility study and in-depth analysis of the needed infrastructure that could give way for the installation of the software.
The job of this Researcher was to help in the preparation of the change. We had to pass through different stages, as described by Lewin’s theory (as cited in Barnard & Stoll, 2010) that change can encounter the unchanging present behaviour, which then moves into a new behaviour, and finally the “refreezing new behaviour” (Barnard & Stoll, 2010, p. 2). These three stages have been used as framework in developing change (Todnem, 2005 as cited in Barnard & Stoll, 2010). However, this theory has been maligned in the few studies conducted and there is little empirical study to support it.
The hypothesis states that online booking reduces patients’ waiting time and enhances patient satisfaction and their attitude toward their healthcare provider. This was proven in the primary research as evidenced by the comments and opinion of participants regarding the benefits of online booking system. The number of participants that provided positive comments to the application of online booking system was significant. Majority were of the opinion that the OD application in the hospital improved patient satisfaction and reduced wait time.
The participants experienced reduced wait time and enhanced patient satisfaction. It was supported further by the evidence from the literature when we focused on various case studies and researches by authors and experts in the field.
In the analysis of the approaches to OD, we used the principles of “The Transformation Programme 2007-2010,” in order to provide an effective change to the organisation in this case study. Measures of success and performance standards for the organisation are “easy access, confidence and staff pride” (Health service executive, 2010, p. 9). This guides our plan and activities for the hospital and in deciding to apply online booking system as an organisational change to ensure “easy access, confidence and staff pride” for this organisation.
Easy access means patients (regarded as customers) can have healthcare service at their own flexible time, or at the shortest time they need healthcare. When a patient says he/she has easy access to healthcare, it means they can contact the doctor anytime they want healthcare, whether it is emergency or outpatient care. The doctor should be able to provide healthcare at the patient’s satisfaction. Confidence means patients have confidence of their healthcare providers. Staff pride refers to the staffs’ ability to provide healthcare and the stakeholders are proud that their healthcare providers can deliver what they need.
The HSE model provides a gradual change, but there are planned approaches that introduce rapid change, which is unpredictable. In our project, change cannot be considered rapid because the gradual process refers to the time the beneficiaries are ready to accept it from the time the change was applied.
Many of the outpatients did not have internet connection, but the internet was not very much a necessity as their doctor could provide them their ultrasound scheduling without the patients being online. The HSE model can be said as effective because it has been used by large organisations with remarkable successes. The only thing it was not effective was because the change was to be introduced involving aged respondents or seniors, who from the start did not want to participate. However, it became a big success when they still participated and gave us their feedback which were very inspiring.
There were positive results on the application of online booking in the ultrasound section of the radiology department. Positive results emphasised that the sample participants, who were outpatients, saved time and effort in going to the radiology department, but most of all, their waiting time was significantly reduced.
The aim of applying OD and introducing a software for online booking was to reduce the waiting time. The attending physician would just input the name of the patient in the system, which then provides scheduling for ultrasound. This online booking also provides doctor-patient interaction, thereby providing extra time for treatment and high-quality healthcare. The hospital’s website provides doctor-patient interaction. Outpatients are able to post their complaints and suggestions and doctors respond to their complaints. A website administrator manages the website.
Project Impact
This is a focus on patients’ wait time, in particular the time patients spend before they avail of the ultrasound facility in the hospital. Some words or terms have been mentioned by patients and even doctors and health providers regarding patients’ wait time because this has been a common problem in clinics and large hospitals, for example, “pain-in-the-neck,” an unsolvable problem, or problem that goes with healthcare delivery.
Doctors and hospital administrators would like to deal with it but many would argue that it is hard to solve this problem with a small facility, which serves a large population but has no budget to hire new doctors and purchase new equipments. Patients have to suffer and bear what the hospital can offer. In this hospital under study, the problem of patients’ wait time was a complicated one, and it involved sub-types of patients’ wait time. This means there were many causes, but we had to select one type of patients’ wait time to make the problem solvable. For instance, we selected patients’ wait time before they could avail of the ultrasound section of the hospital. The doctor and the patients had to wait before this scheduling, so that both doctor and patients were victims, including the staff. When online booking system was introduced, the problem was solved, but it did not happen so easily because the process was about change and organisational development (OD). The process involved people, technology, and activities.
The results of change had a tremendous impact on the organisation, in particular the doctors and staff, and outpatients themselves. This Researcher interviewed some of the doctors and nurses about the impact of online booking for ultrasound patients. They were thankful, enthusiastic, and positive of the future of online booking, considering that treatment is now made easy with rapid results from ultrasound and radiology. At last, they could breath so easily now and converse with the patients without so much complaints of their facility. Now, they could go on with their normal activities and improve their service of providing high-quality healthcare. Most doctors opined that this was not only a simple activity or simple solution to a small problem, because everything and everybody was affected and a beneficiary.
The reactions of the staff who were part of the survey was also encouraging. They were asked patient satisfaction, the factors that put the patients into inconvenience and the remedies for these factors, and the costs of the entire OD. With respect to the costs, the staff could not give a definitive answer, but they provided the costs not in terms of the monetary aspect but in the practical benefits that the change could provide to the hospital itself and to the patients. They affirmed the patients’ benefits, although it was too early to state the concrete benefits considering that many of the participants were already in their senior age and they could not provide a long-term impression on the benefits of online booking. However, the staff participants were optimistic about the OD and they provided insights about it. They also stated that in the long run they would want the OD process to continue and they would suggest the matter to top management and the doctors and nurses assigned with the outpatient department and the different clinics.
The patients were also very thankful, although from the start they were sceptical and did not want to accept change. They argued that any change in the hospital would exacerbate the bad conditions and low performance of the doctors and staff of the hospital. When this Researcher interviewed them, in addition to the questionnaires, they were also very enthusiastic and happy about the “simple” solution. Some of the patients had internet connection, so that we were able to chat with them and interview them online. Most of their comments about the impact of the online booking are positive. Most of the patients of the second set of participants were aged citizens who could hardly walk from the clinic to the ultrasound section. Going to and from the clinic and ultrasound facility was really tiresome for them. With the online booking, they could go to the facility only when they had seen their names published online, along with the schedule for ultrasound.
While there were positive results, there were negative comments from the beginning because we can consider this as a gradual change. Since it is a gradual change, we cannot derive all the possible benefits in a short time.
Stakeholders
The survey drew a number of observations and experiences, which were quite contrasting. These came from the stakeholders themselves. It was also the intention of this Researcher to get their opinion, ideas, suggestions and comments. The stakeholders were outpatients and their families, the doctors and nurses, the staff and radiologists of the ultrasound and radiology department, and all the others affected by the change. Their reactions were varied, but as a whole, they were positive and, as stated in the hypothesis, they proved our hypothesis that reducing patient’s time can enhance customer satisfaction.
The first set of participants were not satisfied with their health service provider. Their waiting time allowed them to have more pain because they had to wait for long hours before they could not have access to the ultrasound machine. Complaints and “murmurings” of the participants were common reaction of patients who suffer from being part of waiting list, or long queue in hospitals. Many of them wanted to complain, but since they had illnesses there was no time to complain. All they wanted was a doctor’s prescription and medicine to alleviate the pain and suffering. We could just imagine patients going to the ultrasound section to wait for their scheduling, and returning to their attending physician again to wait since he/she is attending to other patients. This was a painstaking process for patients, especially the seniors, who had no family to guide and attend to their needs. The predicament was exacerbating. There were some of the prospective participants who did not want to participate in the survey, and it was only when we explained to them that we could assist in answering their questionnaires that they gave us a nod.
The second set of participants were those who took the survey when online booking was in effect, and we got their positive responses. The stakeholders’ opinion and suggestions formed part of the rich data and knowledge for this dissertation and for future research.
Practice
We can refer this section of the dissertation to practice for our profession. This is a practice, which is tantamount to actual practice of my career as a health provider that includes my vision and goals as a student and professional. It is a worthwhile experience to be a part of an organisation, but at the same time I am continuing my learning process. Organisations should encourage their members and employees to continually learn and improve their craft and talent because it is a need in this time of intense of globalisation and stiff competition among individuals and organisations.
Theory
We are faced with theories as we go along in our various pursuits as students and as professionals. The theory that we espoused at the beginning of this dissertation focused on the relationship of health providers and their patients, and the enhancement of this relationship. The organisation, the base for the relationship of these stakeholders, must conduct continual organisational development, and that OD must be able to improve that relationship. A theory that we have proven is that reducing patients’ wait time enhances their satisfaction as patients or customers of the organisation. Another theory is to apply the OD to minimise the impact of wait time. There are other related theories we discussed and introduced in the review of the literature in which some were proven true and correct through our primary research.
Strengths of the Project
The strength in our project lies in the fact that there was actual application and we draw the cooperation of almost all the stakeholders, from top management down to the staff, including the outpatients. We can say that there was big success because the hospital is now using online booking, and has reduced patient’s wait time in going to the radiology department for ultrasound.
There was collaboration on the part of the Researcher, the staff of the radiology department and hospital management. We provided a plan, I laid out my student knowledge and experience as a professional, and the staff and management were very open and cooperative about online booking. The activity was one of those endeavours they had overlooked in the course of conducting business and in delivering healthcare. Perhaps, they were too busy. There are small activities that can serve the best purpose and change big things, even the system itself, which we often overlook.
The strength in this activity lies in the fact that it served so many people. Although it cannot be said that it is a lasting solution, it will benefit the patients and the hospital staff for many years. It is not lasting because, as discussed earlier, organisations have to continually change and adopt with change in this time of intense globalisation and competition.
Another strength is the availability of technology. A computer program can be made to suit an organisation’s needs, and it is possible if one has the funds. Although it was the hospital’s responsibility, the program itself was discussed between this Researcher, management and staff of the hospital. It was not to be the concern of only one party; it had to be the concern of most of stakeholders who understood what IT and computer programming is. When the software was installed in the hospital’s computer infrastructure, the result was an almost perfect program. There were no glitches and the requests of the users were easily granted.
Limitations of the Project
This Researcher had limited resources at the beginning of the project. Relying on technology to reduce patients’ wait time is only one of those simple solutions. The best solution should rely on people, not on technology. This is a limitation because people in the hospital, the staff, doctors, and management, are not permanent. They change too. This activity of reducing patients’ time should be applied institutionally; meaning it has to be a common practice of the management to conduct a study on reducing patients’ wait time on a regular basis.
Future studies and follow-up of the project might not be provided, and they can forget all about this project in the future because of so many reasons. It is the job of the hospital management and concerned individuals to conduct a follow-up of the project. Whatever will be the outcome in the future will depend on how the people are receptive of the change. That is why, it is has to be institutional. However, they can peruse from past studies, such this one, of the importance of reducing patients’ wait time.
Recommendations
Change may come from the healthcare providers themselves, and from the employees. Motivations should come from their respective organisations so that change will be easily accepted and successful.
Care must be changing and improving all the time. Integrated service should be introduced during the different phases of the care process.
The community must be like an organisation, which must prepare for change so that the members can receive maximum service. Hospital services must provide cost effective healthcare.
Healthcare organisations must have continual change and must know how to adopt with change, which must be institutional and not mere individual change. As discussed in the introduction and in the literature, change is disturbing, but disturbing in the sense that it alters the status quo and stirs the water to have a ripple effect, which can be for the benefit of all. The ripple effect will provide benefit for all stakeholders.
Research on reducing patients’ time must not stop when it has been addressed and has provided minimum benefits for the patients and all the other stakeholders in the healthcare sector. It cannot be addressed in one single instance; it has to be continual. That said, this study is only one of those “small” activities that should be enlarged by other researchers who have the necessary resources and organisation. Small clinics and large hospitals with a bigger population base need this kind of research. We highly recommend that future researchers use this dissertation as one of their references.
Summary and Conclusion
This dissertation dealt on several issues, emphasising on organisational change and the significance of this change to the members. These issues are of prime importance to human existence because it involved healthcare and to organisations since it is about organisational improvement. As we tried from the beginning to draw data and information from different sources, we were groping for words, but it was only for a short time. This is because vast information and data were available from various sources, like online databases (journals and articles), physical library (books and news items), and many others.
Healthcare is not a lonely subject; meaning, it is a common issue and problem of many organisations and nation states. Many have tried to address it; others have failed but some have been successful. The choice of model in the introduction of change and organisational development is important, and we have to follow those who have led and made their successes in this endeavour.
This dissertation provided those information and data, collected from valuable sources about OD and high-quality healthcare. We worked on actual research and compared our findings with past researches. It is with pride that we recommend this as future reference and hope that it will be helpful for clinics struggling to reduce patients’ wait time.
Reflections “on practice” according to Gibb’s Reflective Cycle
Description of the event
The study we worked on involved organisational development (OD), which is a concept of change in an organisation. The hospital and its many departments and sections can be the best resource for an organisation change, since our project involves providing high-quality healthcare. Our model for organisational change was the Health Service Executive (HSE model), which emphasises high-quality healthcare as a necessity in this time of rapid change in organisations. In particular, our project involved the introduction of an online booking system for the conduct of ultrasound in the radiology department of the hospital. The aim was to reduce patients’ wait time in order to provide patient (or customer) satisfaction. The project started at the beginning of December 2014 and completed on 30 March 2015.
The project had to go through three different phases with its own definite timeline. It went and proceeded to its final work run as scheduled without many problems and barriers because of the teamwork and coordination of the different stakeholders involved in the project.
Feelings
In the beginning, there was a vision, which then transformed into goals and objectives, and the will to work for it. We all have visions and goals. We sometimes experience it in our lifetime, but we just do not consciously know that it is there. As we experience it, dream or think of it, we do not know what to do. We have to discern why it is happening to our subconscious, and why it looks like it is real, but sometimes not. In discerning it, you have to act on it, and with respect to mine, I acted on it, and I acted fast.
When my vision focused on my dissertation, I acted fast to accomplish it because I knew, at the back of my mind, that I was going to succeed. Why did I feel I was going to succeed? This is because in everything I do I give my all; everything, every resource at my disposal – talent, thoughts, experiences. I do it in my personal undertaking, but also in respect to my student activities. This is what I am as a person, and this makes me unique as a human being. I also work hard for what the institution, my Alma Mater, has entrusted me to do and I exert all efforts, talents, and resources to attain my vision and goal.
This is the time that I feel I must strive hard to attain my vision. I think this is the beginning of my way to perfection. We are all led to that perfect creation. I know I am being tested by the hands of time, or, I am being molded like clay so that I can be that person that I can be. Who is molding me? We mold our own clays, but we are also molded so that we can be formed into what that Force wants us to be. Religious people call this God. Science simply calls it a “Force”. But let me not be ashamed about it, because I believe in God, and I know he is molding me to where my destiny should be.
Evaluation
There were suggestions about changes in the hospital. This organisation needed to cope with changes constantly occurring in the 21st century. It was good that top management of Bur Dubai was not indifferent as I found out that they wanted to introduce organisational development (OD) long before I introduced to them the need for technology to be integrated in their system. They formed a committee about integrating technology and functions, and I felt relieved and became more motivated to provide them my knowledge of online booking and the successes that can be attained by adopting to change. This online booking is a must in the ultrasound and radiology department.
My opening salvo was good and so I made some more moves by asking the cooperation of the staff and all other stakeholders of the project. Without the support of the doctors, nurses, and all staff to the introduction of online booking and doctor-patient interaction through the hospital’s website, things would not go as smoothly as they should be. We also informed the outpatients of the hospital’s plans of applying online booking and doctor-patient chat in the website. Many of them were positive about it but there were those who felt skeptical.
Patients who had been going in and out of the hospital and had become “immune” to the hospital’s old and rotten system were the ones who were skeptical of the purported change. In truth, they did not want any change for the organisation; they just wanted out, but they could do nothing. This is one of cheapest government hospitals of the country, which can give them the necessary healthcare, if only management knew how to handle small management problems. I thought this was the opportune time to make the change, and this was the best time to gain their sympathies and trust again to their government and their healthcare providers.
There are lessons I learned from this project. Qualities of leadership can be learned. Leaders can motivate followers and make teamwork a part of their strategies to attain their goals. I also learned something from the staff and health providers. They are committed people. I never knew this until I worked with them. The complaints against them that they were inefficient, that they only worked for their salary, and their (the patients’) complaints were not attended to, were disproved when I worked with them, hand-in-hand, to make the project a success.
Analysis
The Health Service Executive (HSE) model is a benchmark model, which has been in use by the Ireland’s Health Authority and by other large health providers. We recommended this model for our case study because of the principles and approaches, which are for the implementation of high-quality service. As we noted elsewhere in the dissertation and in this Reflection paper, the model pushes for high-quality healthcare and implementing it is really a challenge for organisations, which are opting for change and high performance. HSE model has also drawn success stories from implementing organisations, and using this for our project will certainly lead to success.
Change is based on organisational change theories espoused by Kanter et al. (1992), Kotter (1996), and Luecke (2003, as cited in Barnard & Stoll, 2010). The stages we used in the change process followed the HSE model, which are: “initiation, planning, implementation, and mainstreaming” (Health Service Executive, 2008). We provided timeline for each stage. The theories are based on experiences of individuals and organisations, and researches of authors and theorists. This is now used by organisations.
Conclusion
I really felt enthusiastic and challenged about this project as this is a test to the knowledge, learning and resources I accumulated from the time I started as a young learner. Yes, this is a test and a challenge that will remain in me until I have started my career and a future life with the world of competitions. My colleagues who have become close friends, like brothers and sisters to me, are equally enthusiastic.
Action Plan
There was a need for an action plan for the team to execute. The team was composed of doctors and staff of the hospital, including myself. The plan was conceived taking into consideration the principles and approaches of the HSE change model. It was carried out gradually, but with our firm determination to succeed despite the number of obstacles and barriers.
Reflections “in practice”
Reflection (1)
Technology changes trigger a revolution in internal functions and activities. However, in the applied change, technology improved organisation and customer interaction, which enhanced the development process of the hospital into an organisation of the twenty-first century.
When the software was installed, I thought it was “all’s well that ends well”. But no, it was the beginning of another problem. The beneficiaries, the patients, were not cooperative at first. They did not want to browse the internet and see about online booking. Added to this is the fact that many of them did not have computers and internet connection. We explained to them that even without computer and internet, they could still be benefited with the new system as their doctor would just input their names in the system and their ultrasound schedule is already done.
We prepared very hard for the project, from the planning stage to the actual implementation of the project. We had physical, intellectual, emotional, and psychological preparations. It was a challenging feat, which drew our personal talents and capacity as working individuals.
The staff and technicians of the ultrasound section were very professional and patient, but they had negative thoughts in mind. They were beginning to doubt. It took patience, perseverance, tenacity, and care in introducing the change. This is what we introduced and discussed about the change model, the HSE model. It takes everything to introduce change in the healthcare sector. All we want is to provide a high-quality healthcare for the people of Dubai. I can say that it is worth it.
Reflection (2)
The team members told me that they liked this idea but did not know if we could successfully do it. I interrupted their negative thinking and inspired them to just do it because if we show our interest and determination, Somebody up there will just complete what we have started. We need self-confidence and the will to do it, and add some inspiration to complete the spices. It was a learning experience and an experience that will last for a lifetime.
As we went on, the team became more effective. The problems and barriers along the way were dealt with resilience and expertise by the work team who devised a work plan to make the project run smoothly. We introduced change as needed, but there was resistance on the part of some who were experienced differently. We expected this because resistance is part of change. However, it did little effect because when those few stakeholders felt that change was a part of organisational processes and it was to enhance high-quality health care, they proceeded and accepted it like a gift, and worked for and gave it to the patients like a gift.
Reflection (3)
I would hear negative talk from people to whom this change, this noble endeavour was dedicated to. “This is another ploy of the hospital authorities to cover up for their inefficiencies!” I heard it several times from the patients. I did not ask myself, “How could they say like that?” That was understandable. We knew from the start, from the time we were discussing and planning, that there would be resistance to change, and that resistance will come from the very beneficiaries of the change.
Reflection (4)
Resistance is a barrier to change. We had to seriously deal with it because it was what made change disturbing. As we discussed in the Introduction, people do not want change because it disturbs and alters the normal course of things. However, resistance makes the work more challenging. Our team welcomed it not as a problem but a motivation to strive more for success of the project.
Reflection (5)
Organisational development is a key to the success of organisations, and this OD is disturbingly one of those keys. We recommend this OD to be the subject of future studies, and for other organisations to study and implement it. However, the details of the study, with respect to the information provided by the participants in the survey, cannot be revealed to others, as these are confidential.
References
Allee, V. (1997). The knowledge evolution: Expanding organizational intelligence. New York: Butterworth-Heinemann.
Atinga, R., Abekah, G., & Domfeh, K. (2011). Managing healthcare quality in Ghana: A necessity of patient satisfaction. International Journal of Healthcare Assurance, 24(7), 548-563.
Barnard, M. & Stoll, N. (2010). Organisational change management: A rapid literature review. Web.
Barrick, I. (2009). Transforming health care management. MA: Jones and Bartlett.
Bielen, F. & Demoulin, N. (2007). Waiting time influence on the satisfaction-loyalty relationship in services. Managing Service Quality, 17(2), 174-193.
Blackley, J., Burley, G., & Duffy, M. (2012). Improving patient flow. Web.
Cunningham, N., Reid, L., & MacSwain, S. (2013). Ethics in radiology: Wait lists queue jumping. Canadian Association of Radiologists Journal, 64(1), 170-175.
Drummond-Hay, R. & Bamford, D. (2009). A case study into planning and change management within the UK national health service. International Journal of Public Service, 22(4), 324-337.
Gijo, E., Scaria, J. & Antony, J. (2013). Reducing patient waiting time in a pathology department using Six Sigma methodology. Leadership in Health Services, 26(4), 253-267.
Greaves, C., Gilmore, J., & Bernhardt, L. (2013). Reducing imaging waiting times: enhanced roles and service-redesign. International Journal of Health Care Quality Assurance, 26(3), 195-202.
Gunderman, R. & Sawlani, K. (2012). Waiting in radiology: The patient’s perspective. Academic Radiology, 19(11), 1421-1423.
Hart, M. (1995). Improving out-patient clinic waiting times: Methodological and substantive issues. International Journal of Health Care Quality Assurance, 8(6), 14-22.
Health service executive: A users’ guide to managing change in the Health Service Executive. (2008). Web.
Health service executive: The transformation programme 2007-2010. Web.
HSE: Our structure. (2013). Web.
Improving team working: A guidance document. (2010). Web.
Keilar, A., El-Maraghi, R., & Schweitzer, M. (2010). Improving equitable access to imaging under universal access medicine: The Ontario wait time information program and its impact on hospital policy and process. American College of Radiology, 7(1), 573-581.
Kohn, L. (2011). Electronic prescribing. Washington, D.C.: Diane Publishing.
Kovner, A. & Knickman, J. (2011). Jonas and Kovner’s health care delivery in the United States. New York: Springer.
Kothari, C. (2004). Research methodology: Methods & techniques (2nd ed.). UK: New Age International Publishers Ltd.
Kotter, J. (2008). Shared urgency: Make it part of the culture. Leadership Excellence, 3(1), 3-4.
Kotter, J. & Schlesinger, L. (2008). Choosing strategies for change. Web.
Lodge, A. & Bamford, D. (2007). Health service improvement through diagnostic waiting list management. Leadership in Health Services, 20(4), 254-265.
McAuliffe, E. & Vaerenbergh, C. (2006). Guiding change in the Irish health system. Web.
Miller, R. & Chalapati, N. (2015). Utilizing lean tools to improve value and reduce outpatient wait times in an Indian hospital. Leadership in Health Services, 28(1), 57-69.
Naidu, A. (2009). Factors affecting patient satisfaction and healthcare quality. International Journal of Health Care Quality Assurance, 22(4), 366-381.
National healthcare charter: Your service, your say. (n.d.). Web.
Oliver, C. (2012). The relationship between symbolic interactionism and interpretive description. Qualitative Health Research, 22(3), 141-154.
Robbins, S. (2001). Organizational behavior (9th ed.). New Jersey: Prentice Hall, Inc.
Westbrook, J. (2007). Information technology in health care 2007. VA: IOS Press.
Willoughby, K., Chan, B., & Strenger, M. (2010). Achieving wait time reduction in the emergency department. Leadership in Health Services, 23(4), 304-319.
Zabada, C., Singh, S., & Munchus, G. (2001). The role of information technology in enhancing patient satisfaction. British Journal of Clinical Governance, 6(1), 9-16.
Appendices
Questionnaire
Questions for the patients (before the implementation):
- Please state your age and educational attainment.
- What factors give you satisfaction as patient of this hospital?
- Does reducing wait time improve your satisfaction? (Participants can answer “yes” or “no”.)
- How long is patients’ wait time before the doctor provides the schedule?
- Do you know what is online booking? Is online booking a viable option than the current processing?
- What other suggestions can you give to help improve healthcare delivery?
- Please rate your level of satisfaction on current ultrasound scheduling. (Put check on the box that corresponds to the scale of your choice below:
- Strongly Agree
- Agree
- Neutral
- Disagree
- Strongly Disagree
Questions for the patients (after the implementation):
- Please state your age and educational attainment.
- What can you say of the hospital’s online booking system?
- Do you feel satisfied of the new booking system?
- Has online booking reduced your pain and suffering
- Has improved facility increased your level of satisfaction?
- Has doctors’ and nurses’ service efficiency increased your satisfaction?
- Please rate your level of satisfaction with the implementation of online booking system. (Put check on the box that corresponds to the scale of your choice below:
- Strongly Agree
- Agree
- Neutral
- Disagree
- Strongly Disagree
Questions for the staff:
- How do you measure patient satisfaction?
- What are the usual complaints in your department?
- Do you think patients’ wait time reduce patient satisfaction?
- How long will it take for patients to wait before he/she is scheduled for ultrasound?
- Is online booking a viable option than the current hospital practice?
- Who will implement online booking, who will be involved, and what is everyone’s role?
- What other factors put your patients to inconvenience?
- If patient satisfaction is enhanced, how will this benefit the radiology department and the hospital?
- Have the hospital services increased patients’ level of satisfaction?
Rate the following sentences using the five-point Likert scale: “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree”. This is in addition to the questions listed in the questionnaire:
- We wait for days to get an appointment.
- Patients are crowded and wait outside the radiology section.
- Treatment is effective.
- Workload is organized and effective.
- Patients’ wait time is reduced.
- Treatment does not take time.