Introduction
To respond properly to the requirements of the project, I would critically analyze the relationship between tobacco smoking and lung cancer. Word wide, tobacco smoking remains the leading cause of avertable ill health and death (Hecht, 2002). According to Cunningham (1996), tobacco use causes cancer, heart disease, lung disease, harms the baby for those women who smoke during pregnancy, as well as exposes non-smokers to risks of secondhand smoke. Despite the numerous efforts that have been made by various government and non-government agencies in almost all corners of the world warning people about the risks and dangers of tobacco smoking, the prevalence and use of tobacco among different age groups as well as a gender are still widely spread all over the globe.
According to Cunningham (1996), tobacco use was then and remains today the number one public health enemy. Cunningham points out that the effects of tobacco smoking on health are very dangerous and as a result, the issue requires a critical and significant solution. Although in the past, the use of tobacco products has been associated with first-class countries whose citizens are considered to be rich, recent, the situation has changed because even the citizens of those countries that are commonly referred to as third-class countries have taken up the practice of using tobacco products. As a result, the multinational companies that manufacture and sell tobacco products have spotted markets in low-income countries, and recently, they have carried out massive multimillion advertisements to attract more consumers with the sole aim of making more profits without educating consumers about the negative effects of using tobacco products. Among these products, cigarettes are the most frequently consumed. According to Kuper, Adami, and Boffetta (2002), tobacco products contain more than fifty carcinogens that may increase the risk of cancer by causing mutations that disrupt cell cycle regulation, or through their effect on the immune or endocrine systems. Experts and scholars agree that lung cancer, which is the endemic type of cancer, is the most common cause of death in the world. For example, Hecht (2002), points out that lung cancer which is mostly associated with cigarette smoking is the leading cause of death in the world.
In the literature, Hecht (2002) asserts that larger projections on the increase of the rate of mortality resulting from lung cancer have been predicted since the beginning of the 19th century. Diverse scientific and psychological researchers made predictions from various parts of the world. Researchers argue that cigarette smoking has rapidly become a preferred lifestyle behavior for most people. The preference is more rampant among the youth who consider cigarette smoking as a way of achieving a desired social class status for example the celebrity lifestyles.
The rate of death resulting from lung cancer due to tobacco smoking is very high. For instance according to Hecht (2002), deaths related to lung cancer complications due to cigarette smoking in the USA were 150, 000 people, and in the UK, where lung cancer causes 87% of illnesses, the deaths were about 34 000 people in the year 2000. Indeed, these are very worrying trends that possess major challenges to the mission and vision of the public health sector all over the world.
Hypothesized association between tobacco smoking and lung cancer
According to Hecht (2002), there is a strong positive relationship between the number of cigarettes smoked per day and the incidence of lung cancer. As a risk factor, an increase in tobacco smoking increases the risk or the probability of lung cancer development. In fact, according to Hecht (2002), around eighty-five to ninety percent of all lung cancers are majorly caused by tobacco smoking or exposure to secondhand tobacco smoke.
Kuper, Adami, and Boffetta (2002) assert that in scenarios where there are constant smokers, one in two regular or constant smokers will die due to tobacco smoking-related sickness. Among those who die from tobacco smoking-related diseases, in a group of four people, almost one person dies from lung cancer. The authors point out that regular tobacco smokers have a very higher probability of dying from lung cancer than those people who do not engage in tobacco smoking or expose themselves to secondhand tobacco smoke. They further argue that regular people who smoke tobacco regularly are fifteen times more likely to die from lung cancer than those who have never smoked tobacco in their life or those who have never been exposed to secondhand tobacco smoke. They also point out that people who start smoking tobacco at a younger age are at higher risk of developing lung cancer as opposed to those who begin smoking tobacco in their sunset age. Equally the authors argue that for people who start smoking tobacco at an earlier age but stop the habit later in life, the chances of such kinds of people developing lung cancer are greatly reduced.
Generally, following various research that has been carried out in the past in different parts of the world, most people are nowadays aware of the connection that exists between tobacco smoking and lung cancer. From the literature, it is evident that the hypothesized association between tobacco smoking and lung cancer is that ‘an increase in tobacco smoking increases the probability of developing lung cancer’.
Historical development of the relationship between tobacco smoking and lung cancer
According to Cunningham (1996), the hypothesized relationship between tobacco smoking and lung cancer is well ‘documented on both an epidemiologic and a molecular basis’. A very large number of lung cancer cases have been directly linked to tobacco smoking. Cunningham (1996), remarks that although health issues concerning tobacco smoking have been debated during much earlier periods, the effects of tobacco smoking on health received greater attention in the twentieth century. Zander et al. (2008), states that in the year 1924, writer Irving Fisher wrote an article titled ‘Does tobacco injure the human body?’ in this article, Irving Fisher argued that a person who desired to stay fit and remain healthy had an obligation to omit smoking tobacco. The article was published by Reader’s digest and provoked a lot of interest in the tobacco industry. Science published another article written by Raymond Perl of Johns Hopkins University in the year 1938, the article argued that people who did not smoke lived a longer life compared to smokers.
In the context of the association between lung cancer and tobacco smoking, as earlier as 1912, scientific reports although they lack solid proof from researchers indicated the existence of a relationship between tobacco smoking and lung cancer. The reports attributed the increase in tobacco smoking to lung cancer. For example, in a small scale study that was carried out in Germany in the year 1939 between lung cancer men patients and healthy men of the same age group, the researchers found out that lung cancer men patients were more likely to smoke and become heavy smokers than were the health men. In the year 1947, a Canadian physician Dr. Norman Deralue carried out a large-scale study at St. Louis hospital. He analyzed a group of fifty patients who were hospitalized due to lung cancer complications and another group of fifty patients who were hospitalized due to other complications. From the analysis, Dr. Deralue found out that ninety percent of lung cancer patients had smoked and only fifty percent of those hospitalized from other complications had any smoking history. These finds indicate a high positive association between lung cancer patients and tobacco smoking (Cunningham, 1996).
Cunningham (1996) points out that medical students Wynder and Graham carried out another large-scale study in 1950. The study found out that on average, almost ninety-nine percent of the six hundred and five men who had been hospitalized with lung cancer had been smokers for the previous twenty years and around fifty-one percent of them had smoked more than twenty cigarettes on daily basis over this period. In the control group of the patients who had been hospitalized from other diseases not related to cancer, around eighty percent were smokers where only nineteen percent had been smoking more than twenty cigarettes per day. The findings of this study were published in the Journal of American Medical Association (JAMA).
Another large research that found a statistical association between cigarette smoking and lung cancer was carried out by a group of scientists among them Levin Morton. The results of the study were published in the American Medical Journal (Cunningham, 1996). In September 1950, Dr. Richard Doll and Dr. Bradford Hill examined the smoking patterns of lung cancer patients in twenty London hospitals. From their analysis, the two doctors found that majority of the lung cancer patients had regular tobacco smokers. Based on this observation, the doctors concluded that lung cancer was associated with higher percentages of cigarette smoking (Hecht, 2002).
Since 1950, many further studies have been carried out. A good number of these studies have accumulated evidence that shows that increase in the risk of lung cancer is associated with prolonged tobacco smoking. The studies have equally shown a progressive increase of the smoking habits in women as well as men, a decrease of the lung cancer risk development among smokers after cessation compared with smokers who continue smoking, and the increase of the risk for ‘adenocarcinoma’ of the lung of smokers in the recent years (Kuper, Adami and Boffetta, 2002).
Kuper, Adami, and Boffetta (2002) point out a list of five controlled case studies that were carried out in 1950 which identified a link between cigarette smoking and the development of lung cancer among men. The findings of the studies had some ground-breaking contributions to public health since they identified a relationship between tobacco smoking and the development of lung cancer. The findings from both the studies were published and made public in British and USA. These studies are as follows: first is the study that was carried out by Wynder EL and Graham EA to find out whether tobacco smoking was a possible etiologic factor in bronchogenic carcinoma. The authors analyzed six hundred and eight-four proved cases and their findings were published in the American Medical Association Journal. Doll R and Hill AB carried out the second study titled ‘smoking and carcinoma’ and their findings were published as a preliminary report in the British Medical Journal. Levin M and Goldstein H carried out the third research titled ‘Cancer and Tobacco smoking’ and their and their findings were too published as a preliminary report in the British Medical Journal. Schrek R, Baker L, Ballard G, and Dolgoff carried out the fourth research titled ‘Tobacco smoking an etiologic factor in the disease. I. cancer’ and Cancer Research published results of their findings. The fifth research titled ‘Tobacco smoking habits and cancer of the mouth and respiratory systems’ was carried out by Mills C and Porter M. and the Cancer Research equally published the outcomes of their findings. All these studies identified a link between tobacco smoking and lung cancer development. However, despite the findings of the studies, the doctors and the medical fraternity at large were opposed to the idea that tobacco smoking contributed to lung cancer infections and they rejected the results of the studies. This is because according to Kuper, Adami, and Boffetta (2002), most of the professionals in the medical field as well as scientists during this time were tobacco smokers.
Hecht (2002), asserts that although the findings of the five controlled cases received a lot of resistance from both the public and the professional fraternity at large, they stimulated the formation of larger studies later to determine whether the findings were factual. The cohort studies indeed determined that there existed a relationship between lung cancers and tobacco smoking and added other diseases like coronary heart disease, stroke, and chronic lung cancer among many other ill health effects.
Mechanism(s) through which the relationship between smoking and lung cancer occurs
According to Alamian and Paradis (2012), an individual’s health behaviors predict the likelihood of the person developing cancer and the direction the disease takes. Tobacco smoking is a health impairing behavior, which predisposes individuals to high possibilities of developing lung cancer. Concerns on the effect of behaviors and the relationship of developing lung cancer have been attributed to the fact that a larger percentage of ‘mortality from the leading causes of death is caused by behaviors of individuals and that such behaviors are modifiable’ (57). Behaviors express influences on one’s health by either protecting or conveying health risks, by leading to early detection or treatment of the infections, and by producing a direct biological change.
According to Zander et al. (2008), smokers in different parts of the world consider tobacco smoking as a social activity. People consistent with cultural values and the importance of personal relations consider cigarette smoking as a normal activity. They smoke high rates of cigarettes on daily basis. For instance, Hecht (2002) asserts that most Asians like the Indians consider smoking a hookah, a contraption that bubbles tobacco through water, as an activity that should be carried out days after a hard day in fields. Hecht (2002), further points out that the use of hookah to smoke has equally become a habit in most of the New York and Los Angeles bars. According to Hecht (2002), in China, tobacco is mixed with opium and smoked on daily basis and is equally used as a medication. There has been a higher rate of lung cancer infections among these groups of individuals who consider smoking as a normal habit.
Exposure to secondhand smoke is also associated with lung cancer. According to Cunningham (1996), non-smokers who are exposed to tobacco smoking environments, increase their risk of developing lung cancer. Research shows that side-stream smoke that comes from both the cigarette filter and the mouth of a smoker make up around eighty-five percent of the tobacco-smoking environment. This, therefore, implies that non-smokers who are exposed to tobacco smoking environments either at their homes, at workplaces, or in refreshment areas can easily be infected by lung cancer because of inhalation of tobacco contaminated air through the respiratory system. For example, according to Cunningham (1996), research attributes family circles of lung cancer to parental smoking lifestyles. Children who are brought up by parents who are regular smokers have a very high risk of developing lung cancer compared to those who are brought up by parents who do not smoke. Equally, there is substantial evidence connecting the development of childhood ill-health conditions to tobacco smoking during the periods of preconception and pregnancy.
Cunningham (1996) asserts that before tobacco laws came into effect in Canada, cigarettes and other tobacco products were popular Christmas and father’s day gifts. ‘Manufactures sometimes placed regular products in specially decorated Christmas packages and retailers had special displays for special occasions (40). Of recent, reported cases of ill health among the youth due to lung cancer developments have increased rapidly. This is because, as reported earlier, the rate of tobacco consumption among the youth is very rampant. Most young people use tobacco smoking as a strategy that enables them to cope up with stress, achieve good positive moods as well as a means of associating themselves with their preferred social classes.
From the analysis above, it is very clear that the mechanisms through which the relationship between tobacco smoking and lung cancer occurs are social and behavioral. This is because most people, especially the youth, start smoking tobacco as a way that can enable them to achieve their desired social status or due to influences from others.
Variables that may confound the relationship between tobacco smoking and lung cancer
In the dissertation desk reference: the doctoral student’s manual to writing the dissertation, Calabrese (2009), defines a confounding factor as a variable that affects the results that were not foreseen by the researcher’ (32). Calabrese argues that a confounding factor may change the perception originally held by the researcher about the relation that exists between the variables under investigation. The existence of confounding effects suggests that a third variable or variables explain, at least partially, the observed observation between an independent variable and a dependent variable (Calabrese, 2009). In epidemiological studies that are normally carried out to determine the causes of diseases, it is possible to find out that various variables may possess significant risks that affect the development of a particular disease either independently or as a result of the association between them. To maintain credibility as well as the integrity of their works, it is, therefore, necessary for researchers to do all they can to the best of their knowledge to identify and report confounding factors that mitigate the study’s findings as well as describe how the confounding factors disguised the relationships between the study’s primary variables.
Generally, not everyone with the same or similar tobacco exposure develops lung cancer. Both smokers and people who have never smoked or got exposed to tobacco develop lung cancer. This is because different people ‘have different susceptibilities to cancer risk factors, including lung cancer risk factors’ (Calabrese, 2009). Although tobacco smoking is associated with chronic obstructive pulmonary disease, when confounding factors are taken into consideration, the chronic obstructive pulmonary disease has been implicated as an independent risk factor for lung cancer. Leary (2012), points out that another critical confounding risk variable for lung cancer is asbestos exposure. Research shows that workers who are exposed to asbestos are at a higher risk of developing lung cancer compared to those who have never been exposed to asbestos. Leary (2012), remarks that incidences of lung cancer are high in patients who have had head and neck malignancy. Equally, tobacco smokers who are regular alcohol drinkers are at higher risk of developing lung cancer than those smokers who don’t drink alcohol.
It is therefore critical to take into consideration all the confound factors when studying the association between tobacco smoking and the development of lung cancer. This is because the presence of these factors may disguise the results of a given study.
Knowledge gap
Most research in this area has been focused on the association between tobacco smoking and lung cancer development. For example, Dr. Richard Doll and Dr. Bradford carried out their research in London using a random sample of hospitalized lung cancer patients in September 1950 to determine whether there existed a relationship between lung cancer patients and tobacco smoking. Another research carried out by Mills C and Porter M aimed at determining the association that existed between tobacco smoking habits and the cancer of the mouth and respiratory systems. Cunningham (1996) reviews a collection of earlier studies that have been carried out by various individuals as well as government and non-government entities and whose findings had a groundbreaking contribution to public health. Renowned medical journals like the American Medical Journal and the British Medical Journal have published the results of these studies. The objective of most of these earlier studies was to find out the relationship that existed between lung cancer and tobacco smoking as well as the association between the effects of exposure to secondhand tobacco smoke and the development of lung cancer.
Although some studies have been conducted on the association between tobacco smoking and the development of lung cancer, it is clear from the above-reviewed studies that there is no known study on the variables that may confound the relationship between tobacco smoking and the development of lung cancer. This, therefore, leaves a research gap that needs to be addressed.
Areas for future research
Since most studies that have been carried out are focused on the relationship between tobacco smoking and lung cancer, in the future, research should be carried out to determine whether there is an association exists between other tobacco products for example smokeless tobacco or snuff (chewing tobacco) and development of lung cancer. Equally, in the future, scientific research should be carried out to determine the association that may exist between various variables that may confound tobacco smoking for example alcohol drinking and the development of lung cancer. Since some smokers have reported positive health outcomes from smoking i.e. positive mood effects and use of tobacco smoking as a strategy for coping with stress, medical research should be carried out to determine the particular chemical contents of tobacco that bring about these positive health outcomes reported by some smokers. If determined, a scientific exploration should be carried out to determine the possibilities of manufacturing tobacco cigarettes free of harmful chemical contents that increase the chances of cancer development.
Research theory
According to Polt and Beck (2008), a theory is a systematic or figurative explanation of some aspects of reality. In research, theories guide researchers to formulate and base their concepts and arguments concerning various variables of interest in trying to explain some aspect of the world. They play a crucial role in aiding researchers to formulate and design a research project both in quantitative as well as in qualitative research types. In qualitative research, research theories enable researchers to conceptualize all the variables of the study. These variables are either independent or dependent. The independent variable is that factor whose value determines changes or affects the behavior of the dependent variable. In a study, independent variables can easily be manipulated and their presence or degree determines the change of the dependent variable. That is to say, an independent variable is the presumed cause, while the dependent variable is the presumed effect of the independent variable. Using a research theory, researchers can construct a model or a framework that offers an orienting view with clear conceptual underpinnings of the study variables.
The theory that can enable one to study and determine the association between different risk factors i.e. tobacco smoking risk and the development of lung cancer is the theory of causal explanation.
Overarching reasons for choosing the theory of causal explanation
According to Woodward (2003), the theory of casual explanation provides a comprehensive account of explanations from different fields of science and in everyday life. Casual explanation theory enables a researcher to engage some relevant previous literature thus enabling them to point out mistakes that have been committed by others and try as much as possible to avoid them. Since epidemiological studies on lung cancer focus on tobacco smoking and some other facets, this theory, therefore, becomes the most relevant for studying the relationship between lung cancer and tobacco smoking. Woodward (2003) further asserts that most of the previous studies that were carried out to determine the connection between lung cancer and tobacco smoking have utilized the theory of causal explanation. For example, researchers who carried out the controlled case studies of 1950 to determine the connection between tobacco smoking and lung cancer utilized this theory in carrying out their studies and in explaining the findings of their studies which provided a breaking-contribution to public health science.
Since both smokers and non-smokers develop lung cancer, it is therefore important when studying whether increases in tobacco smoking increases the risk of lung cancer, to take into consideration the confounding factors which may expose further the risk of smokers developing lung cancer. The theory of causal explanation will enable a researcher to study not only tobacco smoking effects but also take into consideration potential confounding factors to maintain the credibility of his/her findings.
Major constructs of the theory
The theory of causal explanation enables research to take into consideration all the independent factors that are assumed to be explaining the change of the dependent variable. This, therefore, implies that in applying the theory to test if increases in tobacco smoking increase the incidence of cancer, all variables that have been associated with lung cancer development can be included as the constructs of the theory. The major constructs that can enable a researcher to test the hypothesized relationship between tobacco smoking and the development of lung cancer are tobacco smoking behavior, the intensity of smoking, gender, genes of the smoker, diet, environmental exposure among many other confounding factors as independent variables and lung cancer on the other side as a dependent variable.
A graphical presentation
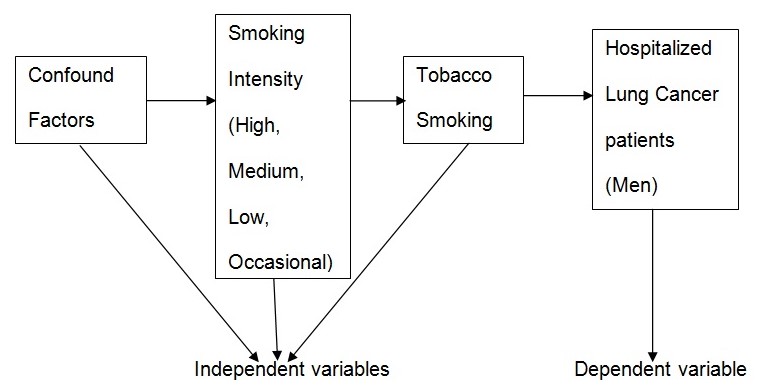
Specific major study constructs
Since it is not possible to encompass all aspects of the theory, my study will examine only hospitalized men’s lung patients who have at least smoked tobacco in their life and lung cancer development risk. To test the study hypothesis properly, smokers will be grouped into regular heavy tobacco smokers (those who smoke more than ten cigarettes per day), regular smokers (those who smoke less than ten cigarettes per day), and occasional smokers while taking into consideration the confounding factors.
References
Alamian, A., & Paradis, G. (2012). Individual and social determinants of multiple chronic disease behavioral risk factors among youth. BMC Public Health, Web.
Calabrese, R. (2009). The doctorial student’s manual to wring dissertation.USA, New York: Rowman & Littlefield Education.
Cunningham, R. (1996). Smoke and Mirror: The Canadian Tobacco War. Ottawa, Canada: International Development Research Centre.
Hecht, S. (2002). Cigarette smoking and lung cancer: chemical mechanisms and approaches to prevention. Lancet Oncology 3(5)461–69.
Kuper, H., Adami, O., & Boffetta, P. (2002). Tobacco use, cancer causation, and public health impact. Journal of Internal Medicine, 4(251)455–466.
Leary, A. (2012). Lung Cancer: A Multidisciplinary Approach.UK, West Sussex: Wiley Blackwell Publishing Ltd.
Polt, D., & Beck, C. (2008). Nursing Research: Generating and Assessing Evidence for Nursing Practice. USA, Philadelphia: Lippincott Williams & Wilkins.
Woodward, J. (2003). Making Things Happen: A Theory of Casual Explanation. USA, New York: Oxford University Press.
Zander et al. (2008). Molecular Pathology of Lung Disease. USA, New York: Springer.