Abstract
The presented project was devoted to capnography during resuscitation of patients in coronary care unit in frames of nursing practice and training. A randomized study conducted in coronary care unit in one of the American hospitals showed high potential of capnography as a tool for monitoring CO2 level while breathing in clinical situations. The study of literature showed not quite sufficient level of nurses’ awareness and competence regarding the application of capnography.
Appropriate project of nurses training based on Kolb cycle method was implemented, with the results assessed with the help of Rogers’ theory of innovations diffusion, as well as survey of nurses’ opinion and satisfaction with training. The assessment showed that such training can serve both as best practice in healthcare facilities and a material for further research in the field of capnography application in clinical situations.
Introduction to the Project
Nurses’ knowledge about clinical devices used for monitoring, assessing, and treating patients with heart conditions is an essential factor for achieving quality of patient care and organizational effectiveness (Cook & Harrop-Griffiths 2019). Studies conducted by Lin, Fang, Wang, Kuo, Wu, and Lo (2017); Novais and Moreira (2015); Pantazopoulos, Xanthos, Pantazopoulos, Papalois, Kouskouni, and Iacovidou (2015) alluded that the lack of knowledge among nurses in using capnography as recommended by the Advanced Cardiac Life Support (ACLS) to capture pertinent information about a patient’s end-tidal carbon dioxide (ETCO2) condition presents uncertainties and poor clinical monitoring practices.
Poor nursing practices as exemplified by the lack of knowledge in using capnography; especially, when success in the patient care is dependent upon the practice knowledge and use of innovative devices such as capnography in a clinical setting (Hamrick, Hamrick, Bhalala, Armstrong, Lee, Kulikowicz, and Shaffner, 2017).
In another study, Hamrick (2017), Heradstveit and Heltne (2014), and Kodali and Urman (2014) linked the importance of using capnography in monitoring and gathering patient information during cardiopulmonary resuscitation events to the critical role of nursing practitioners and the knowledge in using capnography to improve patient quality care. The scholarly debate persists regarding the complexities in instituting clinical monitoring devices in the clinical setting and lack of knowledge to use the equipment effectively. The rationale for this project lies in its potential beneficial effects on increasing nurses’ understanding of the use of capnography and how this can generate positive outcomes for patients in the coronary care unit setting. In the end, the presented in herein could be used to enhance awareness about the project and its objectives.
Capnography is recommended by the Advanced Cardiac Life Support (ACLS) guidelines because it provides information about a patient’s condition. Research indicates that many nurses demonstrate uncertainty when using this method to monitor patients’ end-tidal carbon dioxide (ETCO2) levels because they lack the needed knowledge about capnography use (Lin et al., 2017; Novais & Moreira, 2015; Pantazopoulos et al., 2015).
Poor nursing knowledge about capnography is thus the primary practice problem that this project will aim to address. Improving nurses’ experience with capnography is vital because it would assist in increasing the quality of care for patients. Capnography enhances patient information gathering during cardiopulmonary resuscitation events (Hamrick et al., 2017; Heradstveit & Heltne, 2014; Kodali & Urman, 2014).
The rationale for this project lies in its potential beneficial effects on increasing nurses’ knowledge on the use of capnography and how this can generate positive outcomes for patients in the coronary care unit setting. Chapter one of this proposal contains critical information about this project and the selected practice problems to be addressed. This is accomplished by elaborating on the background of the project, its purpose, significance and explanation into the research problems in determining the appropriate clinical questions. The chapter also presents information regarding project design, such as methodology, organization, assumptions, limitations, and delimitations, to name a few. These details can be used to enhance awareness about the project and its course objectives.
Background of the Project
For reasons that are not always obvious, the practice of resuscitation demonstrates the commitment of doctors to one of the methods of examining patients while denying other, no less informative and useful ones. A striking example is the careful control of the level of potassium in the blood plasma with almost complete inattention to the level of sodium. Another example is the abundance of information on the supply, transport, utilization of oxygen in any critical condition and the lack thereof with respect to carbon dioxide, commonly called carbon dioxide (CO2).
One of the explanations for the described tendentiousness of medical practitioners is a lack of awareness of the importance of measuring the level of sodium and the voltage of carbon dioxide when developing a plan of therapeutic measures. This work is intended, to some extent, to fill this information gap, and is devoted to the use of various methods of capnography in intensive care practice and to ensure the necessary skills of nurses.
Recently, capnography has been given quite a lot of importance as a non-invasive and simple method that allows real-time detection of disturbances in the pattern of respiration due to mechanical ventilation (ALV) and spontaneous respiration, including during heart surgery (Yang et al., 2014). A number of works have been published in which it was shown that capnography makes it possible not only to display the exhaled fraction of CO2 (EtC02), but also to indirectly judge the voltage of CO2 in arterial blood (PaC02). Ferreira et al. (2017), and Sipmann, Bohm, and Tusman (2014) mentioned physiological dead space of the lungs. In addition, the assessment of CO2 metabolism allows diagnosing successfully a number of other disorders of the respiratory and circulatory system.
The combined use of capnography with the determination of PaC02 and the calculation of the gradient between PaC02 and EtC02 (Pa-etC02) expands the possibilities of the method. This gradient changes when the ventilation-perfusion relationship changes, and can also be used to select the value of the positive pressure of the end of expiration after applying the alveolar recruitment maneuver (Sipmann, Bohm, & Tusman, 2014).
The advantage of capnography is that it allows evaluating the function of external respiration in real time, providing important and timely information about violations of the breathing pattern, which is especially important in the postoperative period. Another aspect of the use of capnography is its use in the perioperative period of interventions on the organs of the abdominal cavity and chest, in particular laparoscopic and cardiac surgery.
It is proved that capnography can be an adequate means of controlling ventilation parameters when applying pneumoperitoneum in minimally invasive surgery. A number of published works in which it was shown that capnography allows judging indirectly the value of cardiac output, which is quite important for cardiac patients. However, despite the potential advantages of capnography and the emergence of new modifications of this method, in particular, capnography using a compact computer system in real time and capnography based on the principle of microflow, their use in the perioperative period requires further study.
Cardiac arrest poses a significant threat to patients in coronary care units and is a significant factor that can subsequently lead to a patient’s demise if not addressed timely. As a result, the techniques used to improve the outcomes of patients during cardiac arrests have been widely studied in the literature (Edelson et al., 2014; Mader, Coute, Kellogg, & Harrism, 2014). Capnography has been developed as a measurement tool for monitoring coronary perfusion pressure (CPP) and coronary blood flow. Based on changes to ETCO2 levels, this technique assists to predict new cardiac problems impacting the patient’s condition (Kiekkas, Stefanopoulos, Konstantinou, Bakalis, & Aretha, 2016; Lui, Poon, & Tsui, 2016; Sheak et al., 2015; Venkatesh & Keating, 2017).
Recent studies have shown the effectiveness of capnography in patients with chronic hypercapnic respiratory failure, hypoventilation, severe hypothermia, and metabolic changes (Cereceda-Sánchez & Molina-Mula, 2017; Chhajed et al., 2016; Darocha et al., 2017). However, the widespread implementation of capnography and practice improvement has been hindered due to nurses’ uncertainty and reduced awareness in the application of capnography procedures and practices. According to Dioso (2014) and Duckworth (2017), nurses working with cardiac patients are required to understand the technique of ETCO2 monitoring to be able to apply it correctly.
The knowledge of resuscitation techniques also impacts nurses’ professionalism and readiness to intervene (Bullock, Dodington, Donoghue, & Langhan, 2017). Hence, contemporary researchers stress the importance of preparing nurses to apply capnography along with other techniques during cardiac arrests. It is possible that addressing knowledge barriers about capnography would improve the quality of care in cardiac units and improve patient outcomes (Israel, 2014; Jaffe, 2017; Kuisma et al., 2017; Nassar & Schmidt, 2016). This project is based on the need for increased capnography efforts in coronary care units and the connection between nurses’ knowledge and the application of this technique within the coronary care setting.
Problem Statement
It is not known whether nurses’ knowledge of capnography is solely associated with the use of this tool during cardiopulmonary resuscitation. Based on research, it is essential for nurses working in coronary care units to apply evidence-based techniques to prevent patient deaths from cardiac arrests. Capnography can help to achieve more successful outcomes in these settings since it provides more details about the patient’s condition and indicates the risk of complications (Hassankhani, Aghdam, Rahmani, & Mohammadpoorfard, 2015; Heradstveit & Heltne, 2014). Some authors suggest that nurses must possess the necessary knowledge, experience, and training to provide quality care (Dioso, 2014; Duckworth, 2017).
The primary population affected by the problem includes patients with cardiac issues who are at a high risk of a cardiac arrest and patients within a coronary care unit environment. The limited understanding of capnography can present barriers to its use within a clinical care setting. These limitations can affect the quality of care provided to the patient population, increasing the possibility of adverse outcomes following a cardiac arrest. By implication, a positive relationship between nurses’ knowledge of capnography and their readiness to use this tool would reduce mortality rates.
Therefore, this project seeks to bridge the gap in the literature by increasing the knowledge base of nurses in the coronary care unit with the help of appropriate training based on Kolb cycle method in order to ensure a cycle of accumulation of personal experience, in the future ‑ thought and reflection, and, as a result ‑ action. Since nursing education, training, and quality care is lacking, this project will develop interventions aimed at reducing mortalities from cardiac arrests. Taking into account the problem of lack of nurses’ competence in the field of capnography use during resuscitation of patients in CCU, it seems advisable to develop and implement a project of nurses training and practice, with appropriate mechanism of the intervention efficiency assessment.
Purpose of the Project
The purpose of this project is to explore the relationship between nurses’ knowledge of capnography and its use in coronary care units and the effect of training in capnography use on nurses’ competence in this field. In frames of fulfilling this purpose, the project will provide valuable insight into factors affecting the use of capnography, thus contributing to the field and filling the gaps in the literature identified in the problem statement.
The findings of this project will be beneficial to scholars, practitioners, and healthcare leaders looking to review this presentation. This project will be accomplished using quantitative techniques, including the Nurses’ Knowledge on Capnography Test (Kiekkas et al., 2016) and observations. The variables of the study include nursing knowledge of capnography techniques, the use of capnography during resuscitation, and the correctness of capnography techniques. The first variable is independent, and it is defined as the nurses’ awareness of capnography techniques, purpose, and benefits for the patient. The second variable is dependent and involves the practices of using capnography during resuscitation. The third variable is dependent and involves nurses’ compliance with guidelines and procedures during capnography documentation.
It is anticipated that nurses’ knowledge will have a positive effect on both dependent variables. The design is randomized study with participation of patients and survey with participation of nurses, in frames of positivist paradigm. The population included in the sample will consist of nurses working in coronary care unit of a New Jersey hospital. The study on the use of capnography in coronary artery bypass grafting included 20 patients. Hence, the geographic location of the project will be the USA. Measurable outcomes are as follows, in frames of SMART goal concept:
- Decrease in the number of Adult Medical Emergencies (also known as code blue).
- Increase in the utilization of capnography.
- Assessment of proper ET-Tube placement at the time of intubation.
- Return of spontaneous circulation (ROSC) during code blue.
- Measurement of effective chest compression during CPR.
Although, while each outcome is listed as an individual measure of clinical effectiveness, it is essential to recognize that each exists as part of a pathway for clinical decision making.
Clinical Questions
This project will focus on the relationship between nurses’ knowledge of capnography and their use of this tool during cardiac resuscitation and it will be shown that capnography allows to indirectly judge the value of cardiac output, which is important enough for cardiac patients. The results of the study contribute to the spread of the application of new methods of capnography in cardiac resuscitation, in particular with coronary artery bypass grafting on a working heart.
The accuracy of the real-time capnography technique and microflow technology for these types of surgical interventions is shown, as well as the importance of the nurse’s level of competence for identifying and accounting for indicators obtained by capnography. A correlation between capnographic indicators, blood gas composition and cardiac index was revealed during coronary artery bypass surgery on a working heart. Thus, the project seeks not only to fill in the gaps that exist in the literature, but it will consider several aspects of the topic in the evidence-based framework, on the patients’ sample.
The understanding of nurses connecting a higher knowledge of capnography with frequent use of this tool will reveal the barriers to its implementation (Kiekkas et al., 2016; Turle, Sherren, Nicholson, Callaghan, & Shepherd, 2015). It would be beneficial to determine if increased knowledge is associated with improved compliance with procedures and guidelines for capnography use. Some prior studies have noted that nurses may hesitate to use capnography and other related techniques if they do not feel competent enough (Lin et al., 2017; Lin, Guerguerian, Laussen, & Trbovich, 2015; Novais & Moreira, 2015; Pantazopoulos et al., 2015).
However, it has not been thoroughly investigated whether increasing nurses’ knowledge impacts the correctness of their actions during capnography attempts. By addressing this question, this project will demonstrate if the benefits from an increase in education and training can extend beyond readiness to implement capnography procedures into practice. Based on the information above, the following PICOT question will guide the project premise:
- P Nurses’ competence in capnography use during resuscitation
- I Kolb cycle training
- C Standard nurses education (lectures method)
- O Popularization of diagnostic possibilities of capnography due to increase in nurses’ competence in the field of its use; increase capnography use during resuscitation and its correctness
- T Three months – function of time
Thus, the PICOT question can be formulated as follows: In coronary care units (P), does the increase of nursing knowledge and competence in capnography (I), compared to average or limited understanding of capnography under the conditions of standard nurses education methods (C), increase capnography use during resuscitation and its correctness (O) during the three-month period (T)?
Accordingly, the following questions guiding this quantitative project are formulated:
- Q1. Can nurses’ perceived knowledge of capnography impact the frequency of using this tool during resuscitation?
- Q2. Can nurses’ perceived knowledge of capnography impact their compliance with capnography guidelines and procedures?
- Q3. Can nurses’ perceived knowledge of capnography influence patient outcomes and affect documentation efforts as they pertain to cardiac validation?
To answer these questions, all aspects of the data variables will be examined. Although current evidence does not explicitly address the relationships between these variables, it is possible to make predictions about the results of the project. It is expected that nursing knowledge will influence the frequency of utilization and compliance with clinical procedures. Responses to the clinical questions above will provide further evidence in support of or against this predictive statement. The PICOT question to support the exploration of data factors is as follows:
Advancing Scientific Knowledge
This project will contribute to the development of population health outcomes of patients with cardiovascular diseases by providing evidence to support practice improvements in coronary care due to the increased use of capnography. The undoubted advantages of the method are its information content, non-invasiveness, and the ability to immediately begin monitoring after tracheal intubation. It is also important that it takes only a couple of seconds (Kerslake & Kelly, 2017) to turn on the monitor and attach the adapter to the endotracheal tube. Cardiac arrests can be a common entity among this patient population, and researchers have estimated that 1,000 people in the United States die from cardiac arrest every day (Edelson et al., 2014; Kodali & Urman, 2014; Mader et al., 2014).
This assumption supports the need for continuous improvement in cardiopulmonary resuscitation practices thus allowing for more innovative treatments and more assertive approaches to improving patient outcomes. Some authors have even recommended the used of capnography to improve survival rates (Kiekkas et al., 2016; Lui et al., 2016). However, capnography use in these situations unlikely can be called consistent, thus creating the need for targeted practice improvement measures in the implementation of their design. To improve capnography practices in the coronary care unit, nurses must understand the importance of its use and the effects of capnography on improving patient outcomes.
A clear need for the increase in the knowledge of nurses and the importance of capnography efforts into the improvement on practices would be beneficial in bridging the gap between these two variables. This project will seek to address this need and fill in the gaps in the literature by studying the relationship between nurses’ knowledge of capnography, their use of this tool in resuscitation, and the correctness of capnography use. This project will also provide insight into how nursing knowledge applies to the correct implementation of capnography techniques, and how such techniques are associated with the experience, education, and training that the nurse may possess in their implementation. These factors could contribute to advance practice by providing evidence in support of targeted improvements in nursing education.
The theoretical foundation of the project is comprised of the diffusion if innovations theory. This project will advance this model by identifying the factors influencing nurses’ activities during resuscitation, thus offering a more in-depth look at the workflow in coronary care units. This theory will allow comprising the clinical questions and determining the variables to be examined in the project.
The project will also contribute to resuscitation practice by providing evidence concerning the relationship between nurses’ competence and their activities during resuscitation. The hypothesis is made that nursing education based on Kolb cycle method will ensure diffusion of innovation in healthcare facility due to raising nurses’ competence, which, in turn, will contribute to the increase of capnography use in resuscitation and, accordingly, increase of patient safety and decrease in the number of Adult Medical Emergencies (code blue).
Significance of the Project
The significance of the project lies primarily in addressing the gaps in the scholarly literature on capnography and nurses’ knowledge regarding its use in the coronary care unit. Despite the fact that today capnography is perhaps the only objective method available in wide practice that allows evaluating immediately the effectiveness of heart contractions and deciding whether to stop or continue heart massage, there are practically no studies on the role of nursing personnel in the use of capnography. Meanwhile, the effectiveness of the use of capnography depends on the competence of nursing personnel.
As evidenced by the analysis of current research, articles on capnography focus mostly on the outcomes and implementation of capnography as a tool within this healthcare setting (Kalmar et al., 2018; Langhan, Shabanova, Li, Bernstein, & Shapiro, 2015; Turle et al., 2015). To facilitate the effective use of capnography, it is essential to determine individual factors that impact nurses’ knowledge and the understanding behind the readiness to use capnography in practice. From current observation, it is not known whether increased nurses’ knowledge of capnography is associated with the increased use of this tool during cardiopulmonary resuscitation.
This project aims to explore this aspect of the topic further, thus providing the need for practice improvements and future scholarly work in this area. The results of this project could also lead to the initiation of practice improvements in capnography and enhanced the development of patient outcomes in the coronary care unit setting. This project differs from other studies in the field of capnography use in terms of its focus and builds on other studies concerning the nurses’ perspectives on capnography and its importance in promoting successful patient outcomes (Lin et al., 2017; Novais & Moreira, 2015; Pantazopoulos et al., 2015).
This project also fills in the gaps pertaining to the literature reviews outlined by correlating them with the data provided by studies of capnography and the nurses’ knowledge on the topic and its application within the coronary care unit setting. This project will have critical implications for a variety of stakeholders allowing for the results of the data collected to be achieved through practice improvements in education and training. This, in turn, would contribute to population health by enhancing clinical practice in cardiopulmonary resuscitation and the improvement of capnography efforts within this setting.
Also, it would decrease uncertainty during resuscitation procedures and practices that can stem from a lack of knowledge by nurses, reducing stress and promoting guideline compliance within the coronary care unit. Overall, the project would add value by providing information in support of nursing education and training in capnography based on Kolb cycle method, which would help to advance practice and population health. The significance of the project both in theoretical and practical planes is determined by the fact that it represents an attempt of using diffusion of innovation theory in healthcare. At the same time, the importance of innovations for healthcare can be represented by the following points (Barlow, 2016):
- Innovations make it possible to provide better medical care, achieve a therapeutic result and, therefore, restore or improve the patient’s initial physical status (medical component).
- Lead to a higher degree of satisfaction with the medical care of the population. Innovative activity in medicine should be determined by the needs of patients (social component).
- Aimed at the payback of the medical diagnostic process ‑ health care should be relatively cost-effective (economic component).
It is obvious that it is important to combine the treatment process (introduce into the treatment process) and service innovations ‑ to provide services that are qualitatively improved in terms of characteristics, introduce new ones, increase their consumer value and significance for the recovery of patients.
Rationale for Methodology
The mixed project methodology will help to address the above-described issues by collecting meaningful information on the topic of capnography use and nurses’ knowledge. The methods, representing the primary methods of data collection to be used are quantitative (method of statistical analysis) as well as qualitative methods ‑ observations and survey (Kiekkas et al., 2016). The use of a quantitative methodology is justified by the need to explore individual factors affecting practice in coronary care units, explicitly focusing on nurses’ knowledge and their application of capnography.
Quantitative methodologies have many benefits that are relevant to the proposed project. Initially, not only do they provide a higher level of validity and certainty of results due to the use of statistical tools for data analysis, but they also assist with data collection instruments in proving validity and reliability (Ali & Bhaskar, 2016; Center for Innovation in Research and Teaching, 2020a; Center for Innovation in Research and Teaching, 2020b; Heale & Twycross, 2015; Leppink, O’Sullivan, & Winston, 2016; Watson, 2015).
Observations in qualitative methodologies are useful for answering these questions by clarifying objective information and providing tailoring of any proposed hypothesis into the assessment of project needs (Campbell, 2017; Guo et al., 2016; Nelson, 2018). This means that the use of the selected methodology will provide the information required for fulfilling the purpose of the project. With the aim to ensure higher level of validity of research, survey (interview) method will also be used, to assess nurses’ attitude and satisfaction regarding implementation of new method of training.
The alternative qualitative methodology has been considered for the project, but it contains many limitations that would influence and hinder the reliability of data findings. Qualitative methods are concerned with abstract concepts, and thus their ability to provide objective information is limited. This is one of the core concepts behind their use and their limitations into understanding the participants’ behaviors and attitudes rather than specific activities or knowledge levels can affect the results of the data (Austin & Sutton, 2014; Barnham, 2015; Flanagan, Greenfield, Coad, & Neilson, 2015; Gunnell, 2016). In addition, qualitative instruments are usually not measured for validity and reliability, which increases the risk of bias. This is partially due to qualitative tools focusing on the collection of data that cannot be measured objectively and tested for correctness (Katz-Buonincontro & Anderson, 2018; Rowley, 2014).
Based on the information above, the chosen approach of a quantitative study proves to be more effective than its qualitative alternative at answering the selected clinical questions. Each clinical question posed for the project considers the participants’ level of knowledge and its connection to the use of capnography and guideline compliance. By addressing the clinical questions with correlational methodologies, not only would the data provide the answers to address the gaps in the projects design, but also address the questions into whether improvements in nursing knowledge in the use of capnography has any significance in influencing its use within the coronary care environment.
Mixed research method is a direction of sociological research that has been widely used in recent years, but still remains insufficiently conceptualized. There is a misconception that mixed methods research simply mean any combination of methods (Clark & Ivankova, 2015). Rather, this definition means a multimethod study, while a study using a mix methodology is a combination of precisely qualitative and quantitative methods.
It is important to understand that “mixing” implies a combination of qualitative and quantitative methods, when one method harmoniously complements the other. A synergistic effect may be a measure of harmony: “1 + 1 = 3,” as Fetters and Freshwater (2015) write (Fetters and Freshwater as cited in Clark & Ivankova, 2015). The combination of qualitative and quantitative methods within the framework of one study is advisable when such a design allows getting more in total than both parts give separately.
To implement “mixed” studies combining qualitative and quantitative methods, it is important to understand the nature, possibilities, and limitations of each approach. For example, the main characteristics of traditional quantitative research are the focus on deduction, confirmation of theories/hypotheses, explanation, standardized data collection, and statistical analysis. The researcher acts as the main ‘tool,’ where his subjectivity is the basis of cognitive opportunities. The views of the supporters of quantitative methods are based on the general principles of positivism, where observables and objects are equated in their properties to physical phenomena.
Adherents of qualitative methods offer an alternative to positivism ‑ an interpretive approach based on such areas as constructivism, idealism, relativism, humanism, hermeneutics, postmodernism (Clark & Ivankova, 2015). The fundamental point of “mixed” design in the study is the condition that a combination of methods is a combination of the strengths of each of them. Thus, the main argument of mixed studies is that the data obtained from a combination of methods will exceed the possibilities of using one method (Poth, 2018). In our study, it is assumed that a quantitative method uses a statistical analysis of the hospital’s KPI and a randomized study in which all patients were randomized to normal ventilation and hyperventilation groups before surgery, which differed in parameters of ventilatory support during surgery. Survey (interview) is the selected quantitative method.
Nature of the Project Design
The correlational design was selected for the project as it best fits its goals and purpose. The purpose of such a study is to detect and describe the specific features of the selected population or to identify and describe more or less stable individual characteristics that allow predicting the behavior of people in certain situations. The result of the study will be the detection of differences between the selected population and the “norm” or the detection of correlations between several parameters of one selected population (for example, between the success of managers and their locus of control) and hypotheses about possible interpretations of the results obtained. This design relies on quantitative data collection and analysis methods to explore the relationship between two or more variables (Ingham-Broomfield, 2014).
The variables in correlational research are not manipulated in any way, which will allow the project to reflect the current situation in a New Jersey coronary care unit setting. (Price, Jhangiani, Chiang, Leighton, & Cuttler, 2017). The critical stage of correlational research is data analysis, which is specifically concerned with determining whether one variable influences the other and how those influences can shift data analysis and design. For this purpose, a correlational study using scattergrams, regression analysis, and correlation analysis was applied to obtain correct data analysis (Cronin et al., 2014). The specifics of the correlational design are relevant to the project because they align with its purpose and the identified clinical statements. Since the project is focused on the correlation of nursing knowledge, the use of capnography, and guideline compliance, the correlational design is best suited for this project.
The data for the project will be collected from at least 50 nurses working in the coronary care unit in a New Jersey hospital. The size of the sample is small for a quantitative data analysis sample but could determine any existing relationships among variables through the application of the capnography instrument in the improvement of cardiopulmonary resuscitation attempts, and the appropriate data collection and analysis of patient outcomes (Martínez-Mesa, González-Chica, Bastos, Bonamigo, & Duquia, 2014). Additionally, limitations exist which may include the geographical location of the project and the size of the coronary care unit which could hold a significant impact into the design of the project.
Some data collection procedures include testing the nurse’s knowledge in the use of capnography by the NKCT tool and observations of cardiopulmonary resuscitation procedures which provides the objective information to answer the clinical questions provided in this project’s premise (Campbell, 2017; Kiekkas et al., 2016; Nelson, 2018). The data obtained from testing and observations will be analyzed using scattergrams, regression analysis, and correlational analysis to determine the relationship between two pairs of variables (Cronin et al., 2014). The analysis will fill in any gaps in the literature, thus, addressing the practice problem and answering the clinical questions for this project.
Definition of Terms
This section provides a brief overview of the data variables and operational terms of the project:
Nurses’ competence in capnography
This is one of the two variables to be investigated in the project, and it includes nurses’ awareness about capnography techniques and benefits, as well as their competence about technical equipment use and ETCO2 levels interpretation (Lin et al., 2017; Pantazopoulos et al., 2015). This project will use diffusion of innovations theory developed by Kiekkas et al. (2016) to evaluate nurses’ knowledge.
The use of capnography
This is the second variable to be considered as part of the project and will reflect the use of capnography during cardiopulmonary resuscitation attempts (Novais & Moreira, 2015; Pantazopoulos et al., 2015).
The correctness of capnography techniques
This is the third variable in this project, and it is referred to as the correctness of capnography application. It reflects nurses’ activities during capnography, focusing on their compliance with relevant guidelines and procedures (Novais & Moreira, 2015; Pantazopoulos et al., 2015).
Cardiac arrest
This term is defined as “the cessation of cardiac mechanical activity confirmed by the absence of a detectable pulse, unresponsiveness, and apnea” (Tobi & Amadasun, 2015, p. 132). Cardiac arrest leads to the patient’s death if the appropriate care is not provided immediately.
Cardiopulmonary resuscitation
This term identifies the process of restoring blood flow during a cardiac arrest using chest compressions and artificial ventilation (Kodali & Urman, 2014). There are specific, detailed guidelines on how to perform cardiopulmonary resuscitation that hold the foundation into the need of assessment into nurses’ knowledge on the use of appropriate techniques in their adherence.
Capnography
Capnography is a non-invasive technique to monitor the concentration of partial pressure of carbon dioxide (Kiekkas et al., 2016). It can aid to track the patient’s progress and support decision-making during cardiopulmonary resuscitation.
Coronary artery bypass surgery
Operation that allows restoring blood flow in the arteries of the heart bypassing the site of narrowing of the coronary vessel using shunts (vascular prostheses).
Assumptions, Limitations, Delimitations
As part of the proposal, it is essential to note the assumptions, limitations, and delimitations applicable to this project. The following methodological assumptions were used as part of designing the project:
- The information gathered from the participants will reflect the overall situation in a coronary care unit in New Jersey. Although the sample is small, and there may be individual differences among the participants, it is assumed that their attitudes and perspectives will match those of nurses working within a similar setting under similar situations.
- The nurses selected for the project will have time to participate in the testing portion of the proposed hypothesis. The chosen quantitative methodology implies that each participant will complete the NKCT tool chosen for testing nurses’ knowledge of capnography use (Kiekkas et al., 2016) in the correct assessment of the nurses’ knowledge on the subject and its importance within the clinical setting. Nurses have a busy schedule and an expectation to participate in the study to obtain the appropriate data can improve patient outcomes.
The project is also likely to be affected by certain limitations. These limitations may include:
- The lack of funding affected the prolonged data collection process. Providing compensation to nurses for taking part in testing would increase the response rate and nurses’ willingness to participate in the project.
- Ethical considerations. While conducting studies involving human subjects, scholars face many ethical challenges (Sanjari, Bahramnezhad, Fomani, Shoghi, & Cheraghi, 2014; Zyphur & Pierides, 2017). For example, it may not be possible to conduct observations or test participants as planned.
To address the limitations presented above, it is also vital to apply some delimitations. The proposed delimitations within this project are as follows:
- Institutional support for recruiting and testing participants. This could help to improve nurses’ willingness to participate in the project and remove the obstacles to conducting observations.
Contingency planning for ethical compliance in performing an analysis could help to identify potential ethical constraints and plan for using alternative tools or techniques if necessary.
Summary and Organization of the Remainder of the Project
Overall, cardiopulmonary resuscitation is an essential process in coronary care settings, and additional techniques could increase the chances of survival. Capnography proves to be a valuable addition to the standard CPR procedures in monitoring the patient’s condition and predicting adverse events (Hamrick et al., 2017; Heradstveit & Heltne, 2014; Kodali & Urman, 2014; Venkatesh & Keating, 2017). In the examination of the data collected, barriers to consistent implementation of capnography use and its effects would necessitate the importance of examination into the knowledge of the nurses and their utilization of these concepts consistently into practice. Some studies suggest that many nurses are hesitant to apply such techniques due to the lack of proper training and experience (Lin et al., 2017; Lin et al., 2015; Novais & Moreira, 2015; Pantazopoulos et al., 2015).
This topic has limited evidence in the works of literature, and thus continues to create gaps in data collection on how nursing knowledge affects their readiness to use capnography and compliance with procedures. By advancing the knowledge into this area, the insight gained could be useful for nurses in the improvement of patient outcomes and practice. This present DPI project will seek to address this problem by establishing the relationship between nurses’ knowledge, the use of capnography, and how they correlate into contributing to positive patient outcomes. The literature review provided in Chapter two will present an in-depth view of the barriers associated with capnography use as they relate to nurses’ knowledge through the examination of scholarly findings on the topic and its importance within the clinical setting. Chapter three of the proposal will explore the selected correlational methodology for data collection and analysis.
Literature Review
Capnography as a monitoring tool is applied in a variety of clinical settings, including the operating theatre and coronary care units (CCUs) because it allows nurses to assess patients’ end-tidal carbon dioxide (ETCO2) levels (Conway et al., 2018). These levels help understand the efficiency of a person’s metabolic and respiratory functions while in the coronary care unit. Additionally, during cardiopulmonary resuscitation (CPR), capnography provides an evaluation of both the cardiac function and organ perfusion allowing monitoring of the effect of CPR efforts and predictions regarding the restoration of spontaneous circulation (ROSC).
This project focuses on the gap between the existing guidelines from national healthcare organizations for using capnography in a clinical setting and a nurse’s ability to implement this approach in real life. Understanding the specifics of using capnography during cardiac arrest is vital for ensuring an improvement in the percentage of successful resuscitation attempts. To bridge the gap in knowledge and practice, the nursing knowledge of continuous patient ETCO2 monitoring is investigated in this literature review. The purpose of this DPI project is to analyze the application of capnography usage within the CCU setting. Therefore, this literature review aims to investigate the impact of continuous monitoring of patient ETCO2 levels, the efficacy of using capnography during CPR, and the current state of nursing knowledge about the application of this tool.
The objective is to locate evidence that would help understand the current skills and knowledge that nurses possess regarding capnography monitoring. To access capnography usage during CPR, an examination of a correlation in the application of this tool and the impact it has on the knowledge of nurses should be considered. The relationship between nursing knowledge on capnography and patient outcomes would be emphasized, and this review will be conducted using evidence-based studies. The organization of this chapter is as follows: initially, the background information about applying capnography within a hospital setting, and evidence regarding mortality rates during CPR will be presented.
The overall topic of capnography in medicine, its use, and its impact on patient outcomes will be explored. Additionally, the clinical questions that are the focus of this project will be presented in this section. Next, the theoretical foundation section will focus on nursing care theories that will be utilized for developing a practice improvement strategy. Finally, the review of literature section will provide a synthesis of studies and evidence supported by clinical inquiries about the use of capnography in CCU and the correlation between nurses’ knowledge and CPR outcomes.
Subsections provide the assessment of background information, including the history of capnography invention, its initial application, and first scholarly publications describing the specifics of respiratory monitoring. Next, theme 1 reviews the connection between nurses’ knowledge, organizational factors, and patient outcomes. Subsequent subsections focus on the diversity of application offered by capnography, its use in coronary care units and during resuscitation, and the issues that may contribute to improper utilization of capnography.
The review was conducted using online libraries such as Elsevier, NCBI, and PubMed to locate relevant evidence-based publications about capnography and the most recent descriptive and empirical studies to develop a cohesive understanding of this instrument. The reviewed articles were selected based on publication date, number of citations in other sources, quality of evidence, and limitations cited by the authors. Besides, the methodology and study design and its appropriateness with the research scope were examined. Wright (2017) argues that although capnography has been used in the clinical setting for many years, the actual use of this approach was limited.
Anesthesia procedures and the practice of using capnography instruments for monitoring cardiac attacks have gained attention in its application in the healthcare setting. It is important in CCU since the implementation of capnography tools improves the number of successful resuscitation cases, suggesting that aspects that obstruct the adequate application of this instrument exist. One of the limitations placed on the esteemed outcomes of capnography utilization derives from the knowledge base that individuals may possess when utilizing the tool.
Theoretical Foundations
In modern socio-economic conditions, innovations in healthcare are especially necessary and in demand. They are a powerful impetus for development both in the field of disease prevention and treatment, and in the field of socio-economic development of industry organizations, contributing to the expansion of the range of medical services and their fundamentally qualitative improvement in order to increase the life expectancy of citizens and strengthen their health
Direct practice improvement, in fact, represents introduction of innovations which requires application of appropriate theories. In studies of the specifics of the innovation process, one of the most famous and popular is the theory of diffusion of innovations by E. Rogers. The diffusion (distribution) of innovations is the process by which new ideas, technologies, and offers are distributed between members of the social system through communication channels for a certain period of time (Rogers, 1995).
Under the social system in the theory of diffusion of innovations is understood a group of interconnected elements united by a common process of solving a problem or task to achieve a common goal. Elements or members of a social system can be individuals, informal groups, organizations, etc. In the context of studying the diffusion of innovations, we study the structures of social systems, group norms and decision-making models within them, as well as those organizational changes that appear in these social systems as a result of innovation (Rogers, 1995). A communication channel is a means of exchanging information about innovations between elements and substructures of a social system.
Rogers proposed a model of the process of consumer involvement in the adoption of innovation, which includes the following stages: recognition, interest, evaluation, testing, recognition. Graphically, this theory has the form of a standard bell-shaped curve (normal distribution curve), divided into five parts according to the class of consumers at each stage. The mathematical interpretation of the circuit has the following form (Rogers, 1995):
Nt-Nt-1=k×Nt-1×M-Nt-1, (1)
where Nt – the number of people who have accepted innovation at time t, M is the maximum number of potential consumers, M-Nt-1 is the number of people who can be attracted.
Graphically, the function has the form of an S-shaped curve and reflects the three phases of the introduction of new products: attracting first consumers (slow growth), sharp growth, saturation (growth slowdown). The driving force of the diffusion process is the interpersonal communication of real and planned consumers. Each new customer becomes a source of product information for the potential following: the more there are, the higher the likelihood of innovation.
As the number of uninformed consumers decreases, the process gradually gives way to the opposite trend (Rogers, 1995). Community homogeneity, like “class,” can adversely affect the speed of diffusion, creating barriers to the transmission of information, and this also needs to be taken into account. The consumers in our project will be nurses, because this project focuses on improving nurses’ ability to use capnography in CCU units. The phenomenon that is examined through the explored literature is the knowledge of nurses’ and the correlation with the cases of using capnography. The focus is on nursing knowledge of capnography use as an independent variable and mortality rates as a dependent variable.
Review of the Literature
The complications connected to varied airway events often occur outside the operating theatre and result in high mortality rates. Kerslake and Kelly (2016) state that in 70% of explored cases application of capnography would help mitigate the adverse impact of airway complications or prevent deaths of patients. These statistics are valid for patients dependent on artificial airway support. In addition, capnography application in CUU units can provide valuable input in monitoring ETCO2 levels during resuscitation. The following subsections will examine the evidence suggesting the necessity of utilizing capnography during CPR and the current evidence relating to nurses’ knowledge of this instrument as well as data relating to its application.
In the United States, the American Heart Association advises on using capnography during CPR. In Europe, the NAP4 guidelines, which are published for medical institutions both in Europe and the United Kingdom, use of capnography is obligatory for patients subjected to anesthesia, regardless of the devices used for airway support (Kershake & Kelly, 2016; Soar et al., 2015, Link et al., 2015). Additionally, patients receiving advanced life support should also receive continuous capnography monitoring to detect any life-threatening changes. While this suggests that capnography can be helpful in preventing mortality or airway complications in patients within varied clinical settings, the use of capnography during resuscitation procedures is the topic that requires additional exploration.
The appearance of the capnography curve has an independent diagnostic value. Below, there is a curve characteristic of a healthy person. Several key points are identified on the curve, allowing considering the location and significance of these points during the respiratory cycle, consisting of successive phases of expiration and inhalation (Fig. 1).
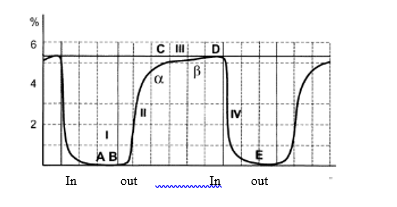
Point A corresponds to the beginning of the exhalation phase, when air enters from the dead space (trachea and bronchial tree), filled with atmospheric air, which almost does not contain carbon dioxide. Point A normally corresponds to a zero value of CO2 concentration on the capnogram curve. The interval AB (stage I expiration) reflects the ongoing movement through the sensor of the device air from the dead space in the initial stage of exhalation. The concentration of CO2 during this period of time continues to remain zero.
Point B corresponds to a fracture of the curve at the beginning of a rapid increase in carbon dioxide concentration – at this moment air from the respiratory tract (inhomogeneous in CO2 concentration) begins to flow to the capnograph sensor, in which the alveolar component begins to play a larger and larger role. The BC interval is designated as the stage of the capnogram, during which the atmospheric air of the dead space is quickly replaced by the alveolar (point D, is the final part of the BC interval).
Point C of the capnography curve corresponds to the moment when the first portions of air from the alveolar space begin to flow to the sensor of the apparatus. The CD interval (stage III) reflects the concentration of CO2 in the air coming from the alveolar space. This interval is characterized by a smoothly rising, almost plateau-like form, which in healthy people does not change its appearance until the end of the expiration phase (point D).
At point D, the concentration of carbon dioxide reaches its maximum. This point, in connection with its great practical importance, has its own designation – “partial pressure of carbon dioxide at the end of expiration” (PetCO2). Capnographs can be calibrated as a percentage or mmHg. In healthy people in a state of complete rest, RBt02 is 4.5-6.0% (an average of 5 or 36 mmHg). From point D, the inspiration phase in the respiratory cycle begins.
During mechanical ventilation, the patient’s respiratory rate is determined by the ventilation parameters that are set by the doctor (unless auxiliary ventilation modes are used, which allow the patient to take independent breaths). In a number of modern capnographs, the counting function f is incorporated structurally and this parameter is automatically displayed on the monitor screen.
A sharp decrease in cardiac output leads to a significant decrease in blood flow through the lungs. Despite the rapid growth of PaCO2 (“turning on” the bicarbonate buffer against the background of developing metabolic acidosis), due to pronounced hemodynamic disorders, an increase in the ventilation-perfusion ratio and, as a consequence, a decrease in PETCO2 are noted (Aminiahidashti, Shafiee, & Sazgar, 2018).
When performing CPR, palpation of the pulse and auscultation of heart sounds, measurement of blood pressure by an indirect method, observation of the pulse oximetry curve (Sp02) are usually not very informative, since external cardiac massage does not provide proper cardiac output. Many artifacts arising from the mechanical impact on the body of the resuscitated one also join this. The focus on ECG monitoring is also insufficient, which allows one to recognize asystole and ventricular fibrillation, but with electromechanical dissociation it can lead to premature cessation of cardiac massage and the onset of irreversible changes in the brain.
In addition, in conditions of closed cardiac massage, the assessment of the cardiogram is almost impossible due to multiple artifacts. In this situation, the capnogram is the only technique (with the exception of echocardiography that is inaccessible in emergency situations), which allows one to judge the presence of blood flow and ventilation. During CPR, the information content of capnography exceeds all other monitoring methods (Hoff et al., 2019).
It is believed that if during CPR it is possible to increase PETS02 to a level equal to or greater than 15 mm Hg, resuscitation measures are carried out efficiently and there are very high chances of saving the patient. The achievement of such values of PETS02 is often associated with the restoration of independent blood flow (if sodium bicarbonate was not infused at that moment) (Hartmann et al., 2015.). With the restoration of independent cardiac activity, the level of PETS02 begins to increase rapidly and soon reaches normal values.
Capnography is also successfully used for hypoventilation. Hypoventilation refers to the state of gas exchange, in which the MOD is insufficient to maintain the normal gas composition of arterial blood. As a result of hypoventilation, hypercapnia, hypercarbia and gas acidosis are noted (Nassar & Schmidt, 2016.).
The following causes lead to hypoventilation (Nassar & Schmidt, 2016):
- Reduced MOD.
- Increased carbon dioxide production.
- Recirculation of air in the breathing circuit.
- An increase in respiratory dead space with unchanged ventilation parameters.
Capnography has diagnostic significance in the first three conditions. An objective sign of hypoventilation is the persistence of PETS02 over a period of several cycles of more than 5.7% (at normal atmospheric pressure) or, respectively, 43 mmHg (Turle et al., 2015).
It should be noted that in patients suffering from chronic obstructive pulmonary disease (COPD), the level of PETC02 almost always exceeds normal values (Urman & Kodali, 2014). With this pathology, one should not strive to achieve normocapnia in the process of mechanical ventilation, since this naturally leads to a breakdown of the natural compensation mechanisms that have formed in the patient, which is accompanied by severe hemodynamic disorders and, subsequently, significantly complicates the process of weaning the patient from the mechanical ventilation device.
In patients with obstructive pulmonary disease, blood supply to the alveoli suffers less than ventilation. Carbon dioxide entering the alveoli from the blood, due to constantly narrowed bronchioles, is released much longer. The delay in emptying the alveoli from carbon dioxide can vary in different parts of the lungs. This is manifested by a peculiar slope of the plateau of the capnographic curve (opening of the angle a), reflecting the delayed release of CO2 from the affected areas of the lungs (Monnet et al., 2013.).
A sudden short-term increase in PETC02 can be caused by various factors that increase the delivery of CO2 to the lungs. The most common explanation for this change in capnogram is the intravenous infusion of sodium bicarbonate with a corresponding increase in the elimination of CO2 by the lungs. Similar changes in the capnogram occur when the turnstile is removed from the limb, which opens up access to the lungs of blood saturated with CO2 (Monge García et al., 2012.).
The rise of PETC02 after infusion of sodium bicarbonate is usually very short-lived, while the similar effect after removing the turnstile lasts longer. In conditions of adequate mechanical ventilation, none of the above events poses a serious threat and does not indicate any significant complications (Monge García et al., 2012).
In fig. Figure 2 shows the shape of the capnogram characteristic of rapid depressurization of the respiratory tract during mechanical ventilation (defective cuff of the endotracheal tube, exit of the endotracheal tube beyond the glottis).
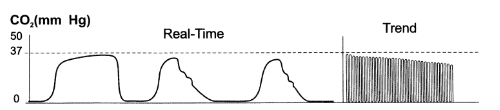
Another, quite common variant of changing the usual form of capnogram is sawtooth oscillations during an exhalation plateau. These oscillations are due to the contraction of the heart, which can be transmitted to adjacent areas of the lungs and cause jerky air movements in the airways. Typically, cardiogenic oscillations are observed in individuals with a relatively small tidal volume in combination with a low respiratory rate. In these patients, this form of capnogram is a variant of the norm (Turle et al., 2015).
Transfer of the patient to mechanical ventilation in many cases involves the use of muscle relaxants. Capnography may be useful for monitoring the depth of the advancing neuromuscular block. Since the diaphragm is more resistant to the action of muscle relaxants, its contractility is restored earlier than in skeletal muscles. When recovering the ability of the diaphragm to contract, characteristic changes appear on the capnography curve (Monge García et al., 2012.). The appearance of incisures on the plateau of the exhalation phase should be considered as one of the early signs of a decrease in the effectiveness of muscle relaxants and an early restoration of skeletal muscle contractility.
Background
The understanding of capnography invention, its initial use, and current trends will help enhance the knowledge of the implications of application and prospects for the future development of capnography. From a historical perspective, capnography is a relatively new approach to evaluating a patient’s health state. The introduction of capnography to the clinical setting in the United States occurred in 1978, and registered nurses began using this tool in recent years to aid patient care (Harper, 2005). However, capnography as an instrument was developed in the 20th century, indicating a long history of using capnography in medicine.
Gravenstein, Jaffe, and Paulus (2005) state that capnography can be used to measure CO2 levels, metabolism, circulation, and other useful metrics, providing an extensive assessment of a patient’s well-being that is useful not only in emergency care but also in day to day monitoring of patients. Therefore, capnography as a monitoring tool provides medical personnel with a better understanding of patient health state because the interpretation of waveforms can serve not only as a measurement of ETCO2, which helps define the purpose and importance of this DPI project.
Alternatives to capnography and their limitations
Capnography is not the only method for evaluating these vital signs, but it is more efficient when compared to others, which impacts the quality of care and is especially crucial during CPR where timing and efficiency of actions can affect the likelihood of survival. According to Gravenstein, Jaffe, and Paulus (2005), capnography is “the continuous recording of CO2 partial pressure [pp] in inspiratory and expiratory gases” (p. 184). A similar method titled capnometry exists; however, it does not provide an opportunity to monitor a patient’s CO2 levels, instead of giving a numerical assessment at a given point in time.
Project 1. History of capnography use in CCU
Capnometry is quite limited in its capabilities and can only assess alveolar ventilation and detect the presence of reverse gas flow in the respiratory circuit (reuse of an already exhausted gas mixture). Capnography, in turn, not only has the above capabilities, but also allows evaluating and monitoring the degree of tightness of the anesthesiology system and its connection with the patient’s airways, ventilator function, evaluating the functions of the cardiovascular system, as well as monitoring some aspects of anesthesia, in which violations can lead to serious complications. Since abnormalities in these systems are diagnosed using capnography rather quickly, the method itself serves as an early warning system in anesthesia.
Capnography, as an instrument, has been applied in medical settings for over forty years. The first article describing the application of this monitoring tool in a clinical setting, more specifically during resuscitation, was published by Kalenda (1978) in which the author suggests that monitoring pulmonary perfusion during cardiac massage performed for patient resuscitation can enhance the outcomes. The presence of a capnography tool allows nurses to control the process more accurately and adjust the cardiac massage as necessary, affecting the efficiency of the resuscitation efforts.
The patient cases presented by Kalenda (1978) suggest that changing resuscitating strategies reduces patient mortality rates. Thus, capnography should be an integral part of the CCU setting (Eola et al., 2019; Gutiérrez et al., 2018; Lui, Poon, & Tsui, 2016). Hence, capnography will aid nurses to diagnose pulmonary embolism, which requires nurses in the coronary care unit to stop resuscitation efforts. Like the evidence presented by Kalenda (1978), more recent literature such as articles by Hartmann, Farris, Di Gennaro, Roberts (2015), suggests that applying capnography during resuscitation helps decrease mortality rates.
Principles of capnography and specifics of the application
The implementation of capnography monitoring may be obstructed not only by the capabilities of a hospital but also due to the opinion’s that medical personnel has regarding this tool. Nurses’ perception of capnography and acceptance of using this tool as an essential method for enhancing patient safety varies and indicates the inadequacy of applying capnography (Clark et al., 2018; Izrailtyan, Qiu, Overdyk, Ersion, Gan, 2018; Langham, Li, & Lichtor, 2016). Therefore, multiple studies illustrate the positive effect of capnography for CPR. While capnography is not the only approach to measuring CO2 levels in a clinical setting, it is the most efficient and accurate.
It improves the nurse’s ability to diagnose respiratory issues and mitigate them, which is especially crucial during CPR. The main principle of capnography tools’ work is the evaluation of CO2 levels, which is useful in determining the production of CO2, lung perfusion, patient’s respiratory patterns, and alveolar ventilation. The capnometer measures the CO2 concentrations using a gas sample collected from a patient (Kellshake & Kelly, 2016). Capnography trace or waveform is the graphic representation of results with time and partial CO2 pressure displayed on X and Y-axes. Hence, the continuous monitoring that this instrument provides is vital in the context of the CPR set.
Capnography allows monitoring the concentration of the carbon dioxide (CO2) in the respiratory gases of the patient. In medicine, this tool is currently used during anesthesia or in intensive care units, while some new studies suggest that using capnography CCU can improve patient outcomes. Capnography allows the medical personnel to monitor the inhaled and exhaled gases. Another benefit of this approach is that it presents an indirect assessment of the patient’s partial pressure in the arterial blood.
The importance of using capnography not only in the operating theatre but also in resuscitation or other emergencies is connected to its ability for detecting airways complications in patients. The general theme of the literature is that capnography has a statistically significant impact on patient outcomes during CPR. A specific practice problem is the impact of nurses’ knowledge on the practice of using capnography in CCU during CPR. Hence, the topic of this paper is practice improvement that will help nurses use capnography tools and interpret results for adjusting resuscitating efforts in CCU.
Subtheme 3. Applying capnography during resuscitation
Examining the scholarly articles on the topic of capnography for resuscitation in the CCU setting can help evaluate the current best practices using evidence-based suggestions and understand the methodology and specifics of the chosen approach. While the discussed literature reviews the utilization of capnography in various settings, further research can help improve the application of this tool in a clinical setting. In general, capnography is helpful in the operating theatre during anesthesia. This non-operative practice allows monitoring of patients. According to Pantazopulus et al. (2015) “low ETCO2 levels may indicate hyperventilation, apnea, esophageal intubation, occlusion of the endotracheal tube, leakage in the ventilation system, poor systemic and pulmonary circulation, hypothermia, massive pulmonary embolism, or ineffective chest compressions” (p. 1053).
The systematic literature review conducted by the authors outlines two main themes connected to the application of this tool exist; implementation and interpretation of results. The latter is especially relevant for the issue of resuscitation because of it a nurse or other medical professional as to be capable of quickly assessing and interpreting the results of monitoring to adjust resuscitation or adjust the inhalation tubes for patients. The use of capnography in CCU resuscitation can improve the number of successful patient cases. However, filtering practices allowing medical personnel to receive reliable results from capnography tools must be implemented since fast oscillations connected to chest compressions can obstruct the resuscitation.
Capnography can be used to reduce chest compressions when resuscitating patients. This methodology was developed by Leturiondo et al. (2019) and Merckx, Lambert, Cantineau, and Duvaidestin (1992) and incorporated capnography-based chest monitoring tailored for the purposes of cardiopulmonary resuscitation. The issue with the approach currently used in medical establishments is that chest compressions affect the accuracy of automated ventilation detection, which can endanger the patient. Leturiondo et al. (2018) developed an algorithm that considers this issue and allows detecting of insufficiencies inpatient ventilation.
Hence, the accuracy of results and reliability of capnography affects the outcomes of resuscitation efforts. This methodology suggests that while applying capnography during resuscitation helps improve the patient state, more developments, and evidence-based research is required to develop practice improvements. The authors used the following variables – number of distorted ventilation and patient outcomes. According to Cook and Garrop-Griffin (2019), “expired carbon dioxide is routinely detectable during the management of patients with recent cardiac arrest, even in the absence of chest compressions” (p. 439). This evidence provides support for the use of capnography in CUUs.
Project 3. Implications of capnography in medicine
The explored evidence suggests that practice improvement guidelines should incorporate strategies for educating and training medical personnel to use capnography in emergencies, for instance, when resuscitating a patient in a CCU unit. According to Aramendi et al. (2017), “capnography permits monitoring ventilation, but the chest compressions provided during CPR corrupt the capnogram and compromised the accuracy of automatic ventilation detectors” (p. 41).
The authors explored 83 episodes of cardiac arrest both in the hospital setting and outside the clinical setting, to determine the best practices for using capnography in resuscitation. The findings suggest that an approach using only a capnography tool can be a valid strategy in the resuscitation process. A study by Stites et al. (2017) revealed that capnography could reduce the number of opioid-induced respiratory issues. The clinical setting observed by the authors implemented the utilization of capnography, and the outcomes suggest a statistically significant improvement in the PCA efforts. The methodology used by the authors of the explored studies suggests that short-term cohort research is the best practice for approaching the issue. Most researchers explored evidence by examining patient records, implying that retrospective studies are conventional approaches to discussing this topic.
Theme 2. The impact of nurse competence in capnography on patient outcomes. The effect of the diffusion of innovations
Education of medical personnel regarding the capnography tools and the interpretation of results has an impact on the use of this tool. While capnography has been used in a clinical setting for almost fifty years, some literature findings suggest the need to dedicate more attention towards educating medical personnel to use this method appropriately for monitoring a patient’s health state and detecting possible heart failure (Langham, Li, & Lichtor, 2017; Long, Koyfman, & Vivirito, 2017). This is a vital component that helps ensure that medical professionals can interpret the capnography traces adequately (Kerslake & Kellt, 2016; Clarke et al., 2018). Another aspect is the attitudes and perception of nurses that may view capnography as an unnecessary tool that obstructs rather than helps inpatient care.
Subtheme 1. The impact of knowledge about a tool and its application in a healthcare setting
The ability to apply capnography is also affected by the technical expertise that enables using innovational instruments and tools, and it is essential to ensure that nurses possess sufficient knowledge to implement capnography in the critical care unit. Wright (2017) argues that “with overwhelming lack of proper training related to new technology devices such capnography, a sound developmental training program regarding the use of capnography can positively affect patient safety and outcomes” (p. 10). The question of education and training proves to be an essential aspect in developing improvement practice suggestions since the ability to use the capnography is crucial for adequate measurement of CO2 levels and adjustment of resuscitation strategies in accordance to this assessment.
The research conducted by White (2015) suggests that nurses who undergo a training showcase better knowledge of the appropriate application of capnography and studies by Saunders, Struya, Pollock, Mestek, and Lightdale (2017) and Subramani et al. (2016) focusing on the correlation between education or training and quality of work displayed by nurses support the conclusions. Since this aspect has clinical value and can impact patient outcomes, it is suggested to develop and implement education programs that target this problem.
Subtheme 2. Nurses knowledge and improvement of practice
Assessment of death associated with failure to apply tools such as capnography can provide an insight into the severer of the problem. Pantazopoulos et al. (2015) argue that only 20% of patients that receive resuscitation survive, despite the recent advancements in the techniques and technology application used to monitor the process and improve the outcomes. Moreover, in the setting outside the hospital, the statistics suggest a survival rate of only 10%. Hence, determining the issues that contribute to the high mortality and possible best practices to help reduce the number of adverse incidents can help design guidelines for medical practitioners. One aspect is the application of capnography, which provides continuous monitoring of the patient’s respiratory system. The examined studies use quantitative approaches to assess the metrics associated with survival.
Project 2. Determining the need for supplemental training to facilitate capnography use
As was previously mentioned, some researchers point out that the use of capnography, as a part of CPR requires additional attention because the waveform can be distorted by chest compressions, indicating a need for additional training required for nurses working in CCUs. Leturiondo et al. (2018) state that over 70% of waveforms examined in their study was distorted because of resuscitation efforts. This requires the development of an algorithm specially tailored towards CPR that would mitigate the impact of chest compressions on capnography results, minimizing the distortion.
The focus of capnography application during resuscitation efforts is on determining whether the endotracheal tube was placed correctly, ensuring that the performed chest compressions are done correctly, and detecting ROSC. Additionally, Leturiondo et al. (2018) argue that capnography can be utilized to develop a prognosis for patients. Ventilation rate monitoring is essential during CPR because it helps nurses detect hyperventilation and prevent adverse patient events. Leturiondo et al. (2018) and Ristagno et al. (2015) state that in general visual inspection of the waveform is enough for tracking breathing patterns of individuals. Because the reliability of results produced through capnography during CRP can be questioned because of distortion, it is necessary to conduct further research.
Nurses and factors relating to their work have a direct impact on patient outcomes, and improvement of practice approaches or hospital environment can enhance health-related metrics in patients. This hypothesis suggests that a variety of factors, including the availability of capnography tools, is hospitals, skills that allow nurses to use and interpret waveforms, personnel perceptions of the technique, and the overall attitude of a healthcare organization can affect the practice of using capnography in CUU (Jaffe, 2017; Darocha et al., 2017).
The literature findings relating to these issues allow designing a questionnaire that will account for all aspects that obstruct or facilitate the utilization of capnography by nurses, making this DPI more comprehensive. The methodology used in studies by Gong, Lu, Zhang, Zhang, Li, (2015), Chhajed, et al. (2017), Darocha et al. (2017), is a mixed design, incorporating a qualitative assessment of nurses’ opinions, hospital managers’ perception of capnography, and quantitative analysis of patient data. This study will adopt the mixed design technique, which connects the views of medical professionals with actual data.
This topic was explored because the goal of this DPI project is to explore the relationships between nurses’ knowledge about capnography and its application to the number of adverse outcomes in CCUs. Therefore, the relationship between factors that impact a nurse’s work and professional qualities such as education or skills should be explored to determine the significance of this aspect. While alternative approaches to the issue may suggest that quality of care is facilitated only by the specifics of nurse training, it is evident that other factors contribute to this aspect as well.
Theme 3. Capnography in a variety of settings
The focus of this practice improvement project is on critical care units, and resuscitation, but the overview of history suggests that capnography is applied in other hospital units, that have established standard guidelines for using capnography in a clinical setting. In general, capnography is usually used during anesthesia to monitor a patient’s respiratory function, and only in the recent years, the researches and practitioners began exploring the implications and benefits of using this monitoring tool in other hospital units. This contributes to the understanding of the specific information that this DPI should investigate. The methods used in the different works of literature will be reviewed. Kerslake and Kelly (2016) state that “capnography can be used both for intubated and non-intubated patients” (p. 178).
The diversity of metrics that can be assessed using capnography present an understanding of the need to dedicate special attention towards educating medical personnel about how and when to use capnography and how to interpret the results. According to Kershake and Kelly (2016), capnography “can be used to detect displaced tracheal tubes and tracheostomy tubes and to diagnose inadvertent esophageal intubation” (p. 178). Additionally, the authors argue that this method can be applied to monitor the cardiovascular functions of a human’s body. This evidence suggests that capnography is a useful tool that can help enhance the process of patient resuscitation in CCU.
This paper focuses explicitly on emergencies and the prospects of using capnography to improve patient outcomes. The literature suggests that capnography can significantly improve the current practices of resuscitation and CPR. According to the European Resuscitation Council, capnography use “enable ROSC to be detected without pausing continuous chest compressions thereby improving quality of resuscitation and preventing the potential harm caused by administering a further bolus of adrenaline after ROSC” (as cited in Kellshake & Kelly, 2016). Therefore, nurses must possess the knowledge regarding capnography in resuscitation and ability to recognize vital signs associated with ROSC.
Cook and Garrop-Griffinth (2019) argue that the utilization of capnography in the varied clinical setting can serve as a measure for preventing deaths. The authors’ base their conclusions on a study of contemporary practices applied in hospitals. The results suggest that a large percentage of individuals are dying due to misplaced tubes or esophageal intubation, which can be prevented by using capnography. The common reasons cited by the authors are the failure to use capnography and lack of education about this tool that would allow medical personnel to use it in case of emergencies.
Nurses’ ability to accurately identify patterns and interpret waveform results can help in preventing adverse respiratory events. Convey et al. (2019) state that respiratory depression can be detected more easily with the application of capnography while Pantazopoulos et al. (2015) state that “airway management, compression depth and chest recoil, hands-off time, and early defibrillation” are the critical measurements that capnography helps assess (p. 1053).
Airway management is the primary emphasis of this study since it can be used to adjust other elements of resuscitation efforts. However, Pantazopoulos et al. (2015) suggest that current guidelines on monitoring the CO2 levels in a patient gas sample lack clarity and require further examination to develop best practices. Monitoring end-tidal CO2 is used, which involves evaluating the pressure upon exhale. Hence, the importance of the topic discussed in this project is highlighted by this research because explored evidence suggests that a large number of healthcare professionals lack an understanding of how capnography can improve patient care during resuscitation and affect mortality rates.
One should note that conflicting evidence regarding the improvement of patient safety exists. Convey et al. (2019) state that their systematic review findings suggest that different randomized controlled trials produce varied results as some indicate significant improvement, while others suggest no statistically meaningful effect. This issue can be connected to the specifics of use and interpretation of waveforms, which requires the development of a cohesive training practice for nurses and guidelines regulating the application of capnography. Another aspect that signifies the importance of adequate training that will enable nurses to use capnography in a CCU’s setting is the global initiative for using this method in healthcare to improve patient outcomes. This initiative focuses on the utilization of capnography during anesthetize, but it possible that the trend of using this tool will continue and further projects will aim to incorporate capnography in varied clinical settings.
An essential aspect of this project is the ability to accurately assess and measure nurses’ knowledge of capnography use in the CUU setting to be able to compare the two variables. Kiekkas et al. (2016) developed a questionnaire that allows accomplishing this goal titled Nurses’ Knowledge about Capnography Test (NKCT). The questions incorporated in this assessment aim to evaluate the understanding of capnography functions, aspects of end-tidal CO2 levels, waveform interpretation, and specifics of using capnography in a clinical setting.
Ruiz de Gauna et al. (2018) state that chest compression artifact suppressing removes the distortion from waveforms, while studies by Aramendi et al. (2018) and Leturiondo et al. (2018) and Turle, Sherren, Nicholson, Callaghan, and Shepherd (2015) suggest applying automated respiratory monitoring with specific algorithms that help disregard the impact of chest compressions of capnography results. Arguably, the application of such a strategy would require an even more in-depth knowledge of technology from nurses who would use this instrument in their practice during CPRs.
Because of capnography solidifying itself as a preventative measure in accessing CO2 levels and in CPR response, its use within these types of settings should be further researched. De Caen and Maconochie (2018) argue that “Recent systematic reviews suggest, however, that using specific EtCO2 values to guide patient care during adult cardiac arrest is based upon low-quality evidence” (p. 2). Hence, the lack of high-quality literature and reliable data regarding cut-offs and respiratory patterns measured with capnography can explain why the perception of this technique and its use by nurses during CPR is insufficient. Regarding outcome predictions, several studies suggest that capnography can be applied when determining the patient’s state upon CPR.
Subtheme 1. Nurses’ use of capnography affects their decisions regarding patients
As was previously mentioned, capnography can help develop a prognosis for patients, both during resuscitation and monitoring. Zitto, Berardinelli, Butler, Morrison, and Albert (2019) focused their attention on how nurses use capnography results to make decisions regarding patient discharges, using confidence levels assessment. This cross-sectional study observed 133 patients before and after ETCO2 assessments and measured nurses’ perception of the patient’s readiness for discharge. While this study does not provide a follow up illustrating the accuracy of predictions based on readmissions, it is evident that nurses change their prognosis based on the outcomes of ETCO2 levels assessment.
As was previously mentioned, despite that fact that capnography is mainly applied in the operating theatre, most cases of airway complications occur outside this setting. Hence, a need to evaluate the number of such cases and the readiness of nurses to apply capnography in units such as CCU arises. Turle, Sherren, Nicholson, Callaghan, and Shepherd (2015) examined the availability of the actual capnography devices in hospitals across the United Kingdom. This study helps understand whether medical personnel use capnography and compare with patient outcomes.
The methodology applied for the study involves a telephone questionnaire that allowed the researchers to examine the practices of emergency departments and intensive care units concerning their application of capnography. This methodology is consistent with the approach chosen for this DPI, suggesting the validity of findings produced though a questionnaire and quantitative assessments. Out of 211 establishments, only four did not have the equipment necessary to conduct capnography assessment, and only 50% of respondents stated that capnography was used to measure the efficiency of CPR (Turle et al., 2015).
These findings indicate the inefficiency of use connected to capnography utilization in the United Kingdom hospitals. In addition, this study suggests that most establishments lacked the necessary equipment to perform the measurement in general wards. Capnography is currently the most efficient way of evaluating the effectiveness of CPR in a hospital setting. This contributes to this DPI because the factor outlines the reasoning for a need to improve the practice of using capnography during CPR in CCUs. Yilmaz et al. (2018) examined carotid doppler ultrasonography in comparison with capnography to determine the benefits and limitations of the two techniques.
In this study, the patients treated with both methods were examined, and the findings suggest that capnography provides a significantly better evaluation of the ETCO2 levels. Cereceda-Sánchez and Molina-Mula (2017) reviewed the prospects of using capnography in the ED setting for detecting metabolic changes in patients. Since the article is a systemic literature review, the methodology that the authors used involved an examination of 17 studies focusing on the specifics of capnography. The findings suggest that this tool is efficient and cost-effective, which further promotes the need to develop and implement strategies promoting the use of it in the hospital setting.
It is also necessary to understand that nurses in different departments can use capnography, and the decision-making process should incorporate a variety of patient-related factors. Bullock, Dodington, Donoghue, and Langhan (2017) examine patient cases of resuscitation in a pediatric department to identify whether the guidelines by the American Heart Association (AHA) in 2010 are applicable and the specifics of utilizing capnography depending on patient characteristics. The research methodology involved a retrospective review of charts assessing data such as trauma, sex, age, capnography results, and patient outcomes.
The conclusions suggest that the use of capnography in CPR procedures is inadequate since it was applied in only 13% of cases despite the recommendations produced by AHA (Bullock et al., 2017). Moreover, the case reports indicate that individuals who had CPR with capnography were more prone to have a spontaneous circulation in comparison to patients not receiving it. The overall duration of CPR procedures was longer in cases when capnography was applied by the medical personnel suggesting that this instrument improves the accuracy of patient prognosis. This study, alongside other evidence, contributes to this DPI because it highlights the benefits of capnography and lack of its proper application in the United States hospitals.
Subtheme 2. Resuscitation-specific capnography utilization
Capnography is a valuable tool that allows for enhancing the process of monitoring a patient’s respiratory function in an emergency scenario, making it relevant during resuscitation attempts. Examination of the capnography in emergency department helps outline the basis for interview topics that will be applied for this DPI. Haines (2017) examined guidelines and practices used in emergency departments (ED) to provide a qualitative assessment of the capnography application and its benefits.
Since patients in the EDs are at high risk of developing complications because of the respiratory function impairment, this information helps improve the DPI by providing explanations of the application and possible reasoning that explains why this instrument is underused in the United States hospitals. Haines’ (2017) findings are complicit with those of other authors arguing that capnography is beneficial during CPR since it allows the medical personnel to provide continuous chest compressions without a need to check the patient’s pulse.
Project 2. Models of capnography measurement differ and can affect patient outcomes
Although capnography as an instrument is not difficult to apply in a clinical setting because it is non-invasive and requires only the presence of a capnography and a medical professional capable of interpreting the results, there a variety of algorithms and strategies for using this instrument suggested by research, which can make it difficult for nurses to use one approach. Capnography is more efficient when compared to other respiratory monitoring techniques, for instance, pulse oximetry can be used to detect hypoxia, but the results are not produced continuously (Haines, 2017).
Capnography is a non-invasive technique that does not require additional preparations for use, but one should consider the different instruments and their appropriateness within the CCU setting. According to Kellshake and Kelly (2016) currently, two models of applying capnography tools and measuring the CO2 levels exist. The first one is side stream analyzer, which implies taking a sample of gas from the patient’s respiratory tube and placing it in the humidifier filter. This approach is applied in a setting for non-intubated patients because it is more comfortable, and the equipment required for analysis is less bulky when compared to the other two methods. Mainstream analyzers use infrared light that scans the ventilation circuit.
This method is more suitable for monitoring patients during resuscitation.
Some researchers explored the different combinations of tools and techniques to develop the best practice of applying capnography, which can be used in practice improvement. Salen et al. (2001) explored the possibility of combining capnography tools with a cardiac sonographer in order to improve the procedure of patient resuscitation. The objective was to measure the accuracy of predicting resuscitation outcomes using the two instruments in the emergency department (ED). The results support the hypothesis that the combination of the two techniques helps improve the processes of resuscitation and improves patient survival rates.
Subtheme 3. Issues associated with capnography may lead to uncertainties that obstruct nurses from using this tool
While capnography as a tool is relatively simple to apply, the indications of the waveform can be misleading, as several problems with the use of this technique exist. For example, Haines (2017) states that condensation is a common problem that requires medical personnel to remove the tube and flush it with a syringe. The contribution of this topic to the DPI is the need to assess nurses’ knowledge of the troubleshooting techniques that they may need to utilize when using capnography. Another example is a disconnected ventilator that produces a flat trace on the waveform, an indication like that when a patient is not breathing.
Failure to interpret the results leads to the inability of the personnel to recognize esophageal intubation, which leads to either severe brain damage or death (Turle et al., 2015). This suggests that nurse education should incorporate the specifics of using capnography during CPR to ensure that this condition is recognized in time. In addition, some details of waveform interpretation exist since patients who had cardiac arrest caused by respiratory failure tend to have higher ETCO2 levels when compared to others (Turle et al., 2015). Therefore, capnography use and interpretation require a substantial knowledge from a medical professional using the instrument and suggests that nurses’ lack of confidence to apply it can be associated with insufficient experience or training.
Theme 4. Correlation between CPR results and capnography application
This contributes to the purpose of the DPI because empirical evidence and theoretical knowledge about the utilization of capnography in resuscitation can design the questionnaire for nurses to determine their attitudes towards this instrument. Lampe (2017) states that air pressure monitoring is uncommon in non-emergency settings, despite the evidence suggesting that this approach improves the accuracy of CRP. An exploration of the specifics of using capnography during CPR will help enhance the understanding of the knowledge that nurses should possess to use capnography during cardiac arrest.
Subtheme 1. Strategies for overcoming improper waveform interpretation
Researchers such as Aramendi et al. (2018) were able to develop algorithms that allow medical personnel to use programs in a more advanced way, more specifically, for determining the location of ventilation. Hence, it is possible to distinguish between breaths and chest compressions using waveforms. This study has several implications for the burses; it implies the need to improve their current knowledge by providing them with the described algorithm. This can help enhance their confidence in using the technique as well. Additionally, this improves the CRP process in general by mitigating risks of hyperventilation, which is often associated with adverse patient outcomes.
Subtheme 2. Evidence and data are suggesting the prevalence of utilizing capnography during CPR
Nassar and Kerber (2017) argue that despite the significant prevalence of poor outcomes associated with CPR and a large volume of evidence-based research providing guidelines regarding best practices within this domain, the adherence to these suggestions in clinical settings remains low. This suggestion supports the primary claim of this DPI and highlights the need to determine what factors impact the lack of capnography application during CPR and develop interventions that can address these problems. Nassar and Kerber (2017) state that “feedback devices provide instantaneous guidance to the rescuer, improve rescuer technique, and could impact patient outcomes” (p. 1061).
While in their systematic review, the authors cite several elements that contribute to the improvement of CPR practices, capnography is a critical aspect in monitoring chest compression and tracking the return of spontaneous circulation. During CPR, capnography can be used to eliminate insufficiency of chest compressions, since a drop in the ETCO2 levels serves as a good indicator for the issue. Moreover, the recommendations provided by the AHA suggest reaching the level of 20 ETCO2 before examining ROSC.
Project 1. Perception of capnography application during CPR
The previous study suggests that the prevalence of capnography use among nurses use during CPR remains low. However, it is possible that other factors, apart from knowledge and perception, obstruct the adoption of this respiration-monitoring tool. Sahyoun, Siliciano, and Kessler (2018) developed a questionnaire for hospital managers to examine whether the hospitals in the United States and more specifically in the state of New York had equipment that would allow them to use capnography during resuscitation. Hence, the contribution of this research is the ability to evaluate whether nurses have access to these devices and if the lack of capnography tools contributes to the insufficient confidence associated with using these instruments during CPR.
Moreover, this study allowed assessing the attitudes of providers towards using capnography in resuscitation, which is a valuable input into understanding the issue. Sahyoun, Siliciano, and Kessler (2018) state that 95% of the respondents had the devices that allow their personnel monitoring ETCO2 and 97% implemented a protocol for applying them. However, only 54% reported having a protocol tailored explicitly for CPR, which is consistent with the findings of studies by Dioso (2017) and other studies mentioned in this review. The conclusion can be made that despite the availability of capnography, hospital personnel may have difficulty applying these tools because no protocol or guideline that would help them is in place. This supports the need for developing this DPI and introducing it to hospitals in the state.
The assessment of the views of capnography and its actual application in the United Kingdom suggest that more efforts should be dedicated to promoting this approach. Sahyoun, Siliciano, and Kessler (2018) and Duckworth (2017), Hamrick et al. (2017) suggest that the providers in the United States do not perceive capnography as a potent tool for examining the return of spontaneous circulation and have a neutral view of this tool in the context of resuscitation, despite evidence suggesting the efficiency of this method. Hence, the issue is global, and the availability of capnography tools does not result in the application of them by medical personnel.
Kerslake and Kelly (2016) stated that “failure to use capnography in patients dependent on artificial airway caused 70% of ICU-related airway deaths in NAP4” (p. 178). One aspect of the issue is the perception of this tool and the knowledge that allows nurses to use it in emergencies such as CPR. Evidence provided by Clarke et al. (2018) suggests that a large percentage of the observed medical professionals avoid using capnography on the floor since they do not understand the benefits.
Subtheme 3. Enhanced CPR protocol incorporating capnography
One can argue that the lack of guidelines and efforts dedicated to ensuring that hospitals use capnography harms patients when those efforts are not consistent. Carlisle (2015) aimed to develop a standardized protocol for using capnography during resuscitation for opioid-induced respiratory depression (OIRD). This article targets explicitly nurses and their ability to use the tool during CPR. Carliste (2015), and Hassankhani, Aghdam, Rahmani, and Mohammadpoorfard (2015) cites education as a vital factor for promoting the utilization of capnography in a clinical setting.
The findings are based on the nurse interviews regarding the application of the protocol, and the answers suggest that issues are connected not only to the availability of devices and to the system issues and lack of patient adherence. Whitaker and Benson (2016) indicate that approximately 74% of deaths in intensive care units (ICU) can be prevented if capnography monitoring is implemented as standard practice. The primary goal of this strategy is to improve patient safety; hence, the authors also recommend using a standardized protocol and providing nurses with additional training that would fill the gaps in knowledge and understanding of the interpretation of capnography.
Subtheme 4. Other implications of CPR and capnography
Kodali and Urman (2014) suggest that universal application this tool during CPR will allow creating a database of waveforms that can be utilized to improve the existing protocols. Hence, the promotion of using this methodology will help further enhance the practice. Kodali and Urman (2014) conducted a literature search to locate evidence supporting the benefits of capnography in resuscitation published from 1960 and concluded that historically the interpretation of outcomes and attitudes regarding the predictions and evaluating that can be made using this approach changed, since it is accepted that “presence of small obtunded CO2 waveforms during CPR reinforces tracheal location of an endotracheal tube” (p. 332).
In general, capnography use during resuscitation requires the knowledge of not only waveform interpretation, but also the understanding of distortions caused by CPR. This theme relates to the DPI project because one can hypothesize that the complexity of using capnography during resuscitation can be a curial factor contributing to nurses’ lack of confidence when using capnography, especially in emergency cases.
Summary
Overall, the problem that this project explores is the practice of using capnography in the CCU setting during patient resuscitation and the impact of nurses’ knowledge about the tool on the prevalence of use and CPR outcomes. The origin of the issue is connected to evidence presented by scholars, suggesting that nurses both in the United States and in Europe do not apply capnography to guide cardiac massage and track respiratory patterns of patients, despite the availability of capnography tools (Wright, 2017).
This project aims to improve the lack of understanding associated with the perception and knowledge of capnography utilization and patient outcomes. Works, similar to the study by Sahyoun, Siliciano, and Kessler (2018), aim to examine the problem of knowledge about capnography, perception, and the frequency of application. However, the sample size is little, suggesting that more attention should be dedicated to the problem of correlation between knowledge and application. The current literature lacks a study that would focus on this factor and use qualitative design.
The empirical evidence on the topic of capnography suggests that in most cases, using capnography during CPR improves the accuracy of cardiac massage and survival chances. The problem has evolved historically since initially capnography was developed as an instrument applied during anesthesia, but current trends suggest that it can improve the care across many domains (Jooste et al., 2019). However, the ability to use capnography is obstructed by the lack of knowledge and training. Capnography allows medical professionals to monitor a patient’s well-being in CCUs units and nurses in these units should receive not only protocols or guidelines but also adequate training on capnography.
In general, the application of capnography across different domains of patient care becomes more popular. The main trends in applying capnography for patient monitoring within the CCU settings are connected to the promotion of using this tool and improvement of result interpretation that can be obstructed by distortions (Aramendi et al., 2017; Chicote et al., 2019). The primary trend that prevails in the literature is the adoption of capnography for use in a different medical setting, including CCU.
The expansion of the use scope for this instrument suggests that many hospitals will want to have capnography available at each ward, further emphasizing the need to examine personnel’s ability to use this tool correctly (Kellshake & Kelly, 2016). In addition, many researchers develop specific algorithms, including computer programs that help enhance the result interpretation or automate the process of monitoring using capnography (Chicote et al., 2019). One can argue that the general trend is the application of capnography across different units and the improvement of application strategies.
Many studies are based on a small research sample of 20-30 nurses or patients, which can mean underrepresentation. The authors generalize the findings to create a conclusion based on the evidence they collect (Kellshake & Kelly, 2019; Jooste et al., 2019). From this perspective, one can argue that the evidence supporting the efficiency of using capnography in CUU during resuscitation is not justified.
However, other studies focus on exploring patient records to determine the effect of resuscitation using capnography on mortality, which can incorporate enough samples. Conflicts in methodology are connected to the prevalence of quantitative studies that assess the availability of capnography tools, the number of cases where it was applied, and outcomes. Hence, a significant gap in the literature is the lack of evidence that would provide an understanding of nurses’ knowledge of capnography and attitudes towards using this tool. Prior research is done on the topic that explores the chosen phenomena is assessing the prevalence and specifics of nurses using capnography and suggest that in most cases, this instrument is not applied during CPR.
Hence, the phenomena explored in this project are nurses’ knowledge, capnography use during CPR, and patient mortality and the connection between these factors. The majority of the examined studies focus on the advances of using capnography and the specifics of its application (Kellshake & Kelly, 2016). Additionally, it can be argued that a gap in understanding the nurses’ knowledge and its impact on the perception of a tool exists since; suggesting that projects similar to this DPI can enhance the procedures at hospitals.
The methodologies and design used to explore the topic of capnography for resuscitation is an assessment of nurses’ knowledge regarding the use and result interpretation using questionnaires or observations. The literature relates to the DPI since it explores the issue of resuscitation and the benefits of using capnography when measuring CO2 levels. While evidence suggests that using capnography, during resuscitation helps decrease mortality rates, some medical professionals do not use this tool and the ability to identify what factors influence this choice can help design interventions and practice improvement strategies that target the problem (Wright, 2017; de Caen & Maconochie, 2018).
Since this DPI project is qualitative, the studies were chosen for the literature review that explores the phenomena of capnography, its application in CCU, and nurse’s impact on patient outcomes. In this way, the practices and best approaches for using capnography were located that allows one to understand the specifics of this tool. Besides, the qualitative review allows comparing and contrasting different methods and the evolution of using capnography in CPR.
The reason why a qualitative methodology with an application of interviews and assessment of nurses’ knowledge about capnography was chosen for this project is connected to the scope of this DPI. The main goal is to determine the underlying issues obstructing medical professionals from using this tool despite the existing guidelines and evidence that support the necessity of incorporating capnography in resuscitation protocol.
The appropriateness of the DPI’s strategies recommended by the similarities of design in the examined studies since the ones relating to the use of capnography in a clinical setting employed questionnaires and knowledge tests, as well as data such as mortality rates, slimily to the approach chosen for this DPI. The comparison of a different perspective on the topic of capnography displayed in the literature suggests that although this tool is helpful in enhancing CPR efforts, the accuracy of results can be impacted by chest compressions and further improvement of this technique is necessary. On the one hand, the evidence suggests that capnography significantly improves the chances of survival (Wright, 2017).
On the other, additional algorithms and strategies may be utilized to ensure that respiratory patterns are identified correctly. Chapter 3 will focus on exploring the clinical question and on the methodology used for this DPI, using the literature findings.
Methodology
This DPI project focuses on nurses’ knowledge of capnography techniques as they pertain to capnography and its connection with the application of capnography use within a coronary care unit. To validate the arguments set forth; a mixed study of quantitative and qualitative data would be presented to explore the correlational relationship between nursing knowledge of the utilization of capnography and how its usage is pertinent in positive outcome generation with the coronary care units.
The clinical questions to be addressed are whether nurses’ knowledge of capnography impacts the frequency of using this tool during resuscitation and whether nurses’ knowledge of capnography impacts their compliance with capnography guidelines and procedures. Improving nursing knowledge in capnography is essential in increasing the quality of care and resuscitation efforts in generating positive outcomes for patient success rates and promoting increased patient outcomes. This chapter of the proposal will explore the methodology to be used in greater depth, including sampling procedures, data collection instruments, and data analysis methods in the evaluation of the premise set forth.
Statement of the Problem
It is known that nurses working in coronary care units, where the risk of cardiac arrest is high are required to use evidence-based tools and strategies to reduce patient mortality (Israel, 2014; Jaffe, 2017). The capnography tool provides details about the patient’s condition and assists care providers track changes in the patient’s requirements to avoid complications (Heradstveit & Heltne, 2014; Pantazopoulos et al., 2015). Capnography proved to be effective in promoting increased patient outcomes in the detection of abnormalities associated with fluctuations in CO2 levels and following cardiac arrests (Cereceda-Sánchez & Molina-Mula, 2017; Chhajed et al., 2016; Darocha et al., 2017; Hassankhani, Aghdam, Rahmani, & Mohammadpoorfard, 2015).
The widespread application of capnography during resuscitation attempts within specific clinical settings has yet to be achieved due to the lack of specialized training that focuses on the study and understanding of its use (Dioso, 2014; Duckworth, 2017). This subject has not been addressed in literature specifically since most studies focused on the various applications and benefits of capnography.
Hence, it is not known whether increased nurses’ knowledge of capnography is associated with improved use of this tool during cardiopulmonary resuscitation. The problem discussed above affects various patient populations who are at risk of a cardiac arrest, including patients in coronary care units as well as those with chronic cardiovascular conditions. The barriers to consistent implementation of capnography use within a critical care setting prevent care providers from delivering the highest quality of care, thus posing a risk for patients’ survival during a cardiac arrest. Hence, it is essential to study the factors that could hinder the use of capnography in high-risk settings, as this would help to develop evidence-based strategies to enhance capnography use.
Evidence of a positive relationship between nurses’ knowledge of capnography, their readiness to use this tool, and the correctness of capnography techniques would help to fill the gap in current literature expanding on the significance of these techniques. This, in turn, would lead to improvements in nurse’s knowledge and education, establishing a positive influence on survival rates and the quality of care provided to patients.
This DPI improvement project aims at contributing and addressing the hypothesis set forth by evidence on one of the probable factors affecting the use of capnography in coronary care units with emphasis placed on nursing knowledge in the implementation of care practices. Scholars have suggested that insufficient understanding of capnography among care providers may lead to poor readiness to use the tool or incorrect application (Lin et al., 2017; Novais & Moreira, 2015; Pantazopoulos et al., 2015).
These views have not been explored in-depth, and as a result, the evidence to improve education and level of knowledge in capnography among nurses is currently lacking. By exploring the relationship between nurses’ knowledge and their use of capnography during resuscitation efforts, evidence to support or disprove these claims can be provided in this project and its focus. This, in turn, would lead to more informed quality improvement initiatives that would target the core of the issue to enhance capnography use. By providing evidence supporting or disproving the association between nurses’ knowledge and the use of capnography, this project will thus aid in developing interventions aimed at reducing mortalities from cardiac arrest, in the process of coronary artery bypass surgery, and other acute conditions cases in the cardiac units.
Clinical Question
The Clinical/PICOT question for this proposed project is as follows: After the evaluation of current evidence and the clarification of the problem statement, three clinical questions were developed for this DPI project. These clinical questions were designed to address the problem statement by reviewing the relationship between nurses’ knowledge of capnography and their use of this tool during resuscitation.
Q1. Does nurses’ knowledge of capnography impact the frequency of using this tool during resuscitation?
This variable is important because it is suggested that nurses who have inadequate knowledge of capnography would be hesitant to use this tool due to its complexity (Lin et al., 2017; Novais & Moreira, 2015; Pantazopoulos et al., 2015).
A lack of expertise required skills and training in interpretation of ETCO2 levels in emergency situations can place nurses at a disadvantage thus deciding not to use the tool altogether and creating a delay in care by stalling emergency procedures. Alternatively, they could lack an understanding of the benefits of capnography, which would reduce their motivation to apply it to achieve better patient outcomes.
Q2. Does nurses’ knowledge of capnography impact their compliance with capnography guidelines and procedures?
This variable is essential since it suggests whether compliance with capnography guidelines and procedures can affect compliance with its use. As discussed by Novais and Moreira (2015), capnography is a relatively complicated technique, and thus it must be applied in accordance with relevant guidelines and procedures. Using capnography during resuscitation and doing so by following clinical instructions would yield maximum benefits for patients during a cardiac arrest. Capnography is applied during cardiopulmonary resuscitation.
Q3. Does nursing knowledge affect documentation efforts as they pertain to capnography validation?
Answer: This third variable examines the correctness of the documentation of capnography efforts. Although capnography has been utilized, data collection of capnographic events should consistently be recorded.
Based on the selected questions, nurses’ knowledge was chosen as one of the three key variables to be investigated. Nurses’ knowledge reflects nurses’ education, skills, and experience in capnography use encapsulating the center of all the variables mentioned.
In order to collect information related to the three variables, the project will use two different data collection methods: qualitative as well as quantitative data validation analysis. Initially, the nursing knowledge about capnography test will be used to test coronary care nurses’ level of knowledge on capnography (Kiekkas, Stefanopoulos, Konstantinou, Bakalis, & Aretha, 2016). This tool provides a quantitative measure of capnography knowledge, which is useful for getting objective results that can prove helpful in accessing nursing knowledge in their confidence of utilizing the capnography instrument during resuscitation practices and ECO2 monitoring and interventions (Barnham, 2016; Kiekkas et al., 2016).
Secondly, observations will be used to determine the use of capnography and its correctness. This will be provided through the utilization of the facility approved capnography evaluation sheet that will record all the codes occurring within the CCU setting. This sheet will not only record the correctness into the use of the capnography practice but also will be accessed for consistency in this practice.
Lastly, the quality improvement nurse would provide quantitative observations in the form of a capnography event sheet placed in a binder with a recorded score of the capnographic events in the CCU. For example, after each code, the capnography event binder would have data on the capnography event recorded by a nurse on the unit. In the event of a cardiac arrest, examination, and comparison of the consistency, reliability, and validity of the findings through the data collected would be beneficial for the project because it enables the assessment of procedures in an objective manner, thus preventing bias or data distortion (Nelson, 2018).
Qualitative observations could also be helpful in structuring the results for further analysis. For instance, during an inspection of the clinical practice of nurses’ in cardiac events, noting the presence of the appropriate techniques and the overall level of compliance with capnography procedures can be accessed. This would increase the accuracy of results and provide more in-depth information into the benefits and limitations of the results obtained. Analysis of the results using quantitative methods, including statistical, correlation, and regression analysis, would help to clarify the relationship between the two variables.
Regarding the impact of capnography, knowledge on capnography use during resuscitation practices and procedures by the nurses on the coronary care unit would be addressed. Hence, the chosen design supports the purpose of the project and is most appropriate for answering the identified proposed questions.
Project Methodology
The methodology selected for the project would be a mixed study involving qualitative as well as a quantitative approach with emphasis placed on quantitative validation processes. This is justified by the need to explore the subject from an objective viewpoint. The primary benefits of quantitative methods are that they provide accurate numerical information reducing the risk of bias. Additionally, according to various data (Poth, 2018), quantitative methods focus on providing a vast scope of information rather than on exploring the variables in-depth. This means that such methods could be useful in settings where there is a need to collect as much information as possible and draw sound conclusions from it.
In the present case, gathering more information would benefit the project presented by providing more evidence of a correlation between the variables or lack thereof. The data collected in quantitative research is also simplistic in its nature, which makes it particularly useful for observing changes in variables and analyzing data for correlations (Ali & Bhaskar, 2016; Heale & Twycross, 2015; Leppink, O’Sullivan, & Winston, 2016; Watson, 2015).
Quantitative data sources are particularly helpful in obtaining evidence about the effects of one variable on the other, which is the primary goal of this project. It is more useful and practical than the alternative qualitative methodology. In contrast with quantitative data sources, qualitative methods focus on obtaining meaningful information about the participants’ attitudes and beliefs and allow doing so by enhancing the depth of data collected (Austin & Sutton, 2014; Barnham, 2015; Flanagan, Greenfield, Coad, & Neilson, 2015; Gunnell, 2016). Qualitative research focuses on the participants’ perceptions rather than on objective information. In this DPI improvement project, qualitative methods would allow the exploration and examination of nurses’ beliefs about their own knowledge into the implementation of capnography usage and its importance.
This information would be specific to the project’s sample and can render it impossible to use if based solely on the qualitative piece alone when executed into practice (Barnham, 2015). Concerning the second and third variables, qualitative observations would also be less useful because the flow of information will be less structured, thus making it more challenging to establish a correlation (Nelson, 2018). This means that the analysis of the information from qualitative data sources would not be useful in a way that would help to answer the identified clinical questions.
The selected methodology is better suited to answer the posed clinical questions in two ways. By allowing the evaluation of the level of knowledge about capnography objectively, in contrast with qualitative methods, an establishment of the correlation among nursing knowledge could be examined. Given the nature of the problem at hand, evaluating factual knowledge is more important because it provides more information about the effectiveness of nursing education in capnography. Secondly, quantitative data obtained through observations would be more structured, thus making it easier to analyze how nurses’ knowledge translates into their practice. Both benefits would assist in answering the clinical questions using reliable information, thus providing the insight required for quality improvement in nursing education.
As noted above, it is planned to conduct trainings based on the Kolb cycle model. The author of the model, Kolb, proceeds from the assumption that we learn through Activity and Thinking. He found that people learn in one of four ways: through experience, through observation and reflection, through abstract conceptualization, or through active experimentation (Kolb, 1983). Based on this, Kolb developed the repeating cycle necessary to acquire new skills (Kolb, 1983):
- Specific experience ‑ getting the result of an action, “stuffing cones”
- Reflective observation ‑ reflecting on experience
- Theoretical concepts ‑ concludes plans for change
- Practical application ‑ experimental verification
In our project, the duration of training was 2.5 months, with the simultaneous practical application of the acquired skills. The inclusion of nurses in the training process was carried out according to a wavelike principle, with a training duration of 3 weeks for each group, with the aim of further assessing the effectiveness of diffusion of innovations.
Project Design
The chosen design is quantitative correlational methodology, which fits the content of the project and will assist in responding to both clinical questions. Randomized study provided the data for quantitative analysis that focuses on measuring the relationship between two or more variables (Cronin, Coughan, & Smith, 2014). According to Curtis, Comiskey, and Dempsey (2016), “findings from correlational research can be used to determine prevalence and relationships among variables and to forecast events from current data and knowledge” (p. 20). This is particularly relevant to the project because the clinical questions identified in the previous sections focus on the relationship between nurses’ knowledge of capnography (independent variable), their use of the tool (dependent variable), and the correctness of capnography use in resuscitation (dependent variable).
Applying correlational sources into practice would assist in answering both clinical questions with a higher degree of certainty, which will support the fulfillment of the project’s purpose. Quantitative results obtained through correlational research would also assist in practice improvement. For instance, if the results indicate that higher levels of nurses’ knowledge about capnography result in the more frequent and correct use of the tool, this conclusion could be used as a framework for educational interventions targeting capnography use in a coronary care unit setting. The correlational approach uses quantitative data collection methods, including tests, surveys, and quantitative observations (Ingham-Broomfield, 2014).
These methods are also appropriate for the selected project focus and clinical questions because they would allow collecting information about the three variables. One of the most significant features that distinguish correlational data sources from other types of quantitative studies is that the variables are not manipulated in any way (Price, Jhangiani, Chiang, Leighton, & Cuttler, 2017). Combined with the chosen data collection methods, this will allow producing objective data with as little bias as possible and make explicit judgments regarding the relationship between the three variables.
Qualitative data would also be utilized within this project to gain a clearer perception into the nurses’ knowledge of capnography through their own perception of how they may view capnography as an instrument of improvement. For example, in approaching nurses’ knowledge of capnography, asking questions to gain an understanding of how the nurses may view themselves with regards to their capnography knowledge is a skill that needs to be assessed. To solidify nurses’ knowledge of capnography, quantitative studies would need to be performed to assure that any and all knowledge limitations are approached and defined. The specified qualitative data were obtained with the help of survey and subsequent manual analysis (specialized software was not used due to the small amount of sample).
The study on the use of capnography in coronary artery bypass grafting included 20 patients. The criteria for inclusion in the study were the age of the patient over 18 years old, a confirmed diagnosis of coronary heart disease, the planned nature of the surgical intervention, obtaining written informed consent before the study. The criteria for exclusion of patients from the study were obesity of the fourth degree, bronchial asthma, concomitant cardiac pathology, and refusal of informed consent.
The work on the use of capnography in coronary artery bypass surgery with a working heart included 20 patients. The average echocardiographic ejection fraction before surgery was 55.4 ± 8.7% The criteria for inclusion in the study were the patient’s age over 18 years, the planned nature of the surgical intervention, obtaining informed consent, the planned performance of coronary artery bypass surgery on a working heart. The criteria for exclusion of patients from the study were grade IV obesity, refusal to give informed consent, transition to cardiopulmonary bypass (IR) during CABG.
Before surgery, all patients were randomized into two groups, the control and the recruitment group. After connecting standard monitoring, which included ECG, analysis of the ST segment, blood pressure, BaOg, anesthesia was performed using intravenous administration of midazolam, propofol and fentanyl. Intravenous administration of pipecuronium bromide was used to maintain neuromuscular blockade. Propofol and fentanyl were used to maintain anesthesia. Infusion therapy in the intraoperative period was carried out with Ringer-lactate solution. In case of hypovolemia, a solution of hydroxyethyl starch was prescribed for 30 minutes. Intraoperative mechanical ventilation was carried out in a pressure-controlled ventilation mode. In both groups, DO was used, equal to 7 ml / kg of the predicted body weight, PEEP 4 cm H20, Fi02 – 50%, BH – 12-14/min.
Monitoring of EtC02 during the operation and in the next 24 hours of the postoperative period was carried out using an Ondion Microcap Plus apparatus (Ondion Medical Inc, Israel). In 7 patients, an arterial catheter was installed in the femoral artery to perform transpulmonary thermodilution and measure the cardiac index and the global ejection fraction using the PiCCOplus apparatus.
Control measurements were performed at the beginning of the operation, after performing sternotomy, after applying distal anastomoses, at the start of blood flow through shunts, after transferring the patient to ICU, and also after 4, 8 and 24 hours of the postoperative period. During the measurements, hemodynamics and capnography data were recorded, studied blood gas composition In patients of the recruitment group, 15 minutes after the transfer to ICU, the AVEA apparatus (Viasys Healthcare, USA) performed a maneuver of opening the alveoli according to the 40×40 pattern. This maneuver included transferring the patient to the constant mode positive airway pressure (CPAP), peak airway pressure rise to 40 cm H20 for 40 seconds, followed by a peak pressure level corresponding to DO = 7 ml/kg and setting the PEEP level 2 cm H20 above the lower point inflection, determined by the pressure-volume curve.
A study on the use of capnography when performing coronary artery bypass surgery on a working heart demonstrated the adequacy of this monitoring method. At the beginning of the study, a moderate correlation was observed between EtC02 and PaC02 (g = 0.7, p <0.001) (Fig. 3), the total correlation between these parameters at all stages of the work, it also turned out to be reliable (r = 0.65, p = 0.04). These data correspond to the results of studies by a number of authors who studied the accuracy of capnography in patients without pronounced concomitant lung pathology, subjected to Xia implementation of CABG in normothermic conditions IR (Lin et al., 2017).
In the Bland-Altman analysis, the total difference between PaC02 and EtCO2 was 1.9 ± 11.4 mmHg (M ± 2SD) (Fig. 3). This difference is explained by the presence of alveolocapillary CO2 gradient, to a greater extent, the excess of PaCO2 EtC02 values was expressed against the background concomitant COPD present in a significant part of the patients included in the study. It is noteworthy that at the beginning of the study, EtC02 significantly correlated with the cardiac index (r = 0.81, p = 0.05), which also correlates with the data of other authors (Sahyoun, Siliciano, & Kessler, 2018).
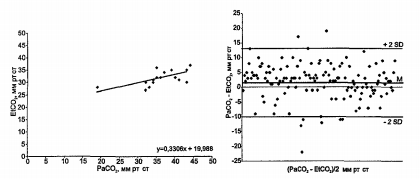
A survey of nurses revealed a high level of satisfaction with the learning process and practical application of skills. Self-reflection in the framework of the Kolb cycle contributed to the assimilation of the competence of capnography (the average rate of assimilation in groups of 87%) and the diffusion of innovations. The greatest interest and level of communication was identified in the second group of training (the next in the learning process after the first), which corresponds to the theory of diffusion of innovations and confirms the effectiveness of the developed project and the selected data analysis methods.
It should be noted that the correlational design suits the purpose and goals of the project and will help to answer the clinical questions. In order to collect data on the three variables, diffusion if innovation theory will be used, based on the results of training in frames of Kolb cycle. Once the data for all variables are provided, data analysis procedures in accordance with the correlational design were applied. Following the procedures of the correlational design will help to answer the clinical questions for the project and provide data for practice improvements in capnography use.
Population and Sample Selection
The populations relevant to the study are nurses working in a coronary care unit environment or a coronary care unit setting. This setting was chosen because nurses are often involved in cardiopulmonary resuscitation. The inclusion criteria require nurses who are qualified to provide emergency procedures during cardiac arrest based on their certification, and the sample will include at least 120 nurses from this population. Collection of the data from a qualitative approach, in the form of asking questions to gain insight into what the nurses’ knowledge may be comprised of with regards to capnography as well as quantitative data sources in the examination into the knowledge of nurses and the use of capnography will be assessed (Ingham-Broomfield, 2014).
The number of nurses displaying knowledge of capnography use as well as proper implementation of the tool during cardiac events in addition to correct utilization of the capnography instruments will be explored to assure adherence in the validation of the data obtained. The selected sample size is rather small for a quantitative study because this design implies collecting data from as many random charts and nurses as possible (Cronin et al., 2014). This is because the size of the sample in this project is constricted by the geographical location of the project and the focus on coronary care units, which limits the number of nurses available for the study. However, still the results of the project, taking into account its effectiveness, can be applied both as best practice and material for further research in the field of capnography.
Since the project does not follow an experimental design, which would require setting the sample size based on power analysis, the selected sample size will likely be enough for a correlational design (Cronin et al., 2014). This DPI practice improvement project will start with obtaining approval from the hospital chosen for the analysis of the study. In order to identify potential participants in the DPI project, the researcher will apply a formulated survey of the nurses working in the coronary care unit of the named institution. The use of quantitative data source examination would be explored for the study, along with the nurse’s responses to survey questions presented.
Nurses will be contacted by e-mail and provided with the necessary information about the project, results, and findings. In order to protect the confidentiality of the nurses and maintain their anonymity in the evaluation of the study and its effects, names, and addresses would not be required in the answering of survey questions. Any identifying information will be stored safely on a password-protected computer and destroyed one year after the end of the project. Additionally, this information will not be used in the project manuscript and will thus remain secret to third parties.
The geographic specifications of the project mean that nurses will be recruited from a single state; in this case, New Jersey, where the evaluation of this DPI improvement project would be performed. Nurses will not have to travel to take the test or participate in observations; instead, all data collection procedures will be conducted at their place of work in a way that does not impair the workflow.
Instrumentation or Sources of Data
There are three separate variables for which data will be collected: nurses’ knowledge of capnography, the use of capnography during resuscitation, and the correctness of capnography use. The survey tool included 30 correct and wrong statements about capnography. The items are separated into four groups: principles of capnography function, conditions affecting end-tidal CO2 pressure, conditions affecting capnography waveform, and indications for capnography use (Kiekkas et al., 2016).
The survey was be delivered to all nurses identified through probability sampling and marked on correctness to determine the level of capnography knowledge. The test will be scored on a 30-point scale, and thus the results will be quantitative. Another source of data used in the project will be the quantitative capnography documentation sheet that specifies how capnography events are recorded in the event of cardiac arrests.
A nurse that has participated in the project can find this tool in a binder outlining cardiac events and recording of the data. Data items on two variables will be collected during observations: binary data reflecting the fact of capnography use during resuscitation (used/not used) and the level of compliance with procedural guidelines for capnography, measured in percentage scores. As the basis for observations, the instructions provided by the Bureau of Emergency Medical Services Trauma, and Preparedness will be used (BETP, 2017).
These guidelines detail capnography procedures, including the positioning of the CO2 sensor, the documentation of findings, and manipulations for the loss of CO2 detection or waveform (BETP, 2017). The activities of the nurse during cardiopulmonary resuscitation will be marked on a scale of 0-4, with one mark for every item category of the guidelines (Placement, Monitoring, Documentation, and Correction). The coded values will be transformed into a percentage score to ease the analysis. Qualitative observations into the survey utilized to test nurse confidence in incorporating capnography within their practice would also be examined.
Assessing nurses’ knowledge of capnography and any barriers that may present themselves as to its use would formulate. This would be to ensure that nursing knowledge is not limited in preventing the utilization of capnography as an improvement measurement but would expand on the knowledge base of its importance by validating the quantitative data presented and addressing any misconceptions in hypothetical application and execution.
Validity
To ensure the validity of the findings in mixed study, In total, two blocks of criteria are proposed. The first block includes criteria common to both qualitative and quantitative research. These include:
- Explication of the scientific context and research objectives (explicit scientific context and purpose);
- selection of appropriate methods;
- respect for participants (respect for participants);
- specificity of the method, adequacy to research issues (specification of methods);
- open research for discussion (appropriate for discussion);
- clarity of data presentation (clarity of presentation);
- assessment of the final achievements in terms of growth and increase in scientific knowledge (contribution to knowledge).
The second block includes validity criteria specific for conducting and publishing a qualitative study:
- disclosure of a certain perspective (owning one’s perspective) – disclosure by the authors of the theoretical, methodological and emotional-personal positions taken in relation to the topic under study, a description of their past experience with this issue, personal opinions;
- description of the sample (situating the sample) – a description of the age, social, gender and ethnicity of the respondents, the number of people removed from the sample, indicating the reasons for this;
- grounding in examples — analysis and conclusions should be illustrated with concrete examples, data, at least two examples should be given on each topic, each individual case should be considered in its entirety;
- providing credibility checks — it is ensured by using several methods of working with data, triangulating, presenting a report to colleagues for possible additions and comments, “supervising” a qualitative research, as well as attracting quantitative data;
- coherence – structured, consistent and well-reasoned analysis, the analysis should be built as a kind of integral history using diagrams and tables;
- achievement of general or specific tasks (accomplishing general – specific research tasks) – an assessment of whether the research meets the task of the general
The proposed criteria are rather creative guidelines for research work and are aimed not at how to evaluate its quality, but at what should be assessed or a specific, specific understanding of the phenomenon being studied.
Reliability
Before the beginning of data collection, data analysis will be required to apply observation criteria to the coronary care unit in nursing practices in cardiopulmonary resuscitation procedures, and data documentation of nurses. This will be provided in marking criteria, and in the comparison of whether the data provided by observations are objective. If there are significant differences in scores, an additional test will be scheduled to determine if the results are due to poor inter-rater reliability of the criteria. If the criteria prove to be unreliable, they will be clarified further and tested again until the level of inter-rater reliability is high. This will ensure the reliability of the data collected through observations, thus contributing to the overall reliability of the findings.
Data Collection Procedures
Before the data collection begins, obtaining institutional approval from the selected hospital to conduct tests and observations in coronary care units is the first step in initiating the process. Once the approval has been obtained data sources requiring a list of all nurses working in the coronary care unit of the selected hospital would be obtained. This would form the basis of the study to access the knowledge of nurses’ working in this setting from a qualitative and quantitative perspective. The software will be used to extract a list of numbers randomly in the identification of adherence in the validation of data (Price et al., 2017).
The nurses involved in the study will be contacted by e-mail, and information about the results and findings would be explored in detail. The study of nurses knowledge and capnography through quantitative evaluations in the use of the institutional provided data source analysis tool, in addition to the NKCT, have been performed with the relevant documentation and procedures ensuring privacy and confidentiality of the nurses partaking in the study (Cronin et al., 2014; Price et al., 2017).
The rights and well-being of the nurses partaking in the study will be protected by securing their personal data without disruption to their workflow or take a long time to complete.
All participating nurses working within the CCU setting will take the test in a controlled environment, such as in a conference room. The test will be completed either after the nurses’ shift or before so that it would not disrupt their workflow. For any nurses who have difficulties in scheduling, the test will be conducted individually. Taking the test in a controlled environment is important to reduce the risk of bias (Price et al., 2017).
If nurses were to take an online test, they would be able to search for additional materials, thus showing a higher level of knowledge than they possess. Hence, the proposed procedure will have a beneficial impact on the quality of the findings. Each test will be completed on the coronary care unit, on paper and marked with the nurse’s identification number to prevent bias in quantitative data results. The other part of data collection will be comprised of quantitative observations of the data measurement tool provided by the institution, which will measure the dependent variables of the use of capnography and its correctness.
The observer will use a list of criteria for observing cardiopulmonary resuscitation procedures. They will mark each criterion as met or unmet based on the nurse’s activities during cardiopulmonary resuscitation. Below each criterion, there will be a list of activities required for fulfillment so that the observer would be able to identify and mark the items quickly. Each correctly completed observation form will also be marked with the nurse’s identification number. Given the correlational design of the study, neither of the variables will be manipulated, so the data collection procedures will be concerned with the recorded information only.
Data Analysis Procedures
For the purposes of the present project, data on three variables will be collected: nurses’ knowledge of capnography, the use of capnography during resuscitation, and the correctness of capnography use. For the first variable, qualitative data would be utilized to obtain knowledge into nurses understanding of capnography. For the second variable, quantitative data will be collected using the Nurses’ Knowledge on Capnography Test, and for the other variables, quantitative observations will be used to assess the use of capnography and its compliance with guidelines (BETP, 2017; Kiekkas et al., 2016). The clinical questions to be answered using data analysis are whether nurses’ knowledge of capnography impacts the frequency of using this tool during resuscitation and whether nurses’ knowledge of capnography impacts their compliance with capnography guidelines and procedures.
The data on nurses’ knowledge of capnography and capnography use during resuscitation will be used to answer the first question, and data on nursing knowledge of capnography and the correctness of its use will be used to respond to the second clinical question. Descriptive statistics will be used to present results in the two categories of data (nurses’ knowledge and the correctness of capnography use).
This will include mean and mode values, as well as standard deviation and variance. However, in order to fulfill the requirements of the correlational design, further data analysis will also be applied to demonstrate the relationship between the three variables. At this point, the raw data will be prepared for analysis through organizing data items by respective nurse identification numbers and then inputting the nurse’s number and the three data items in separate columns. Subsequently, graphic software, such as Excel, will be used to create two scattergrams related to the two clinical questions (Price et al., 2017).
One scattergram will reflect the relationship between nurses’ capnography knowledge and the use of capnography, and the other one will consider nurses’ capnography knowledge and the correctness of capnography use. The analysis of the two scattergrams using statistical software, such as XLSTAT, will be used to determine the correlation coefficient r. The same software will be used for regression analysis of the two pairs of variables. The level of statistical significance for the study is set at p=0.05, which is a standard level used in many studies in nursing (Cronin et al., 2014).
The procedures identified above align with the chosen correlational design since they focus on establishing a correlation between the two variables. The use of specific statistical tools, such as XLSTAT, will help to ensure the correctness of calculations while also supporting the data analysis process. The chosen data analysis procedure also relates to the purpose of the project as it will explore the possible relationship between nurses’ knowledge of capnography and their use of this tool during resuscitation in great depth.
Ethical Considerations
The data shared by the institution and the nurse participants will be stored securely on a password-protected computer, and the participants’ numbers will be used instead of their names during data collection and analysis. The data will be held for one year following the end of the project and will be destroyed by deleting electronic documents and shredding all paper files related to the study. Explanations into the study’s premise would be explained into its entirety to the nurses, and e-mail verification solidifying understanding into the proposed hypothesis would prove useful for the setting presented.
These precautions are in accordance with the European University Institute guide on data protection practices, and they will help to ensure that the participants’ rights will be preserved throughout the duration of the project (EUI, 2019). Additionally, it is important to note that no contact with patients will be made during the project, and thus patients’ health and well-being will not be affected by the project in any way.
Since the present project involves human subjects, it is particularly important to protect their rights and conduct the project in an ethical way (Sanjari, Bahramnezhad, Fomani, Shoghi, & Cheraghi, 2014; Zyphur & Pierides, 2017). The key ethical issues relating to the project are the confidentiality and privacy of personal information provided by the participants and the disruption of nurses’ workflow during the project. Both problems mentioned above, violate the principles of the Belmont Report since they might cause harm to the nurses’ and their patients. In order to address these issues, the project was modeled in a way that minimizes workflow disruptions.
For instance, testing will take place outside of the nurses’ shifts, and observations will be conducted from outside of the wards, thus preventing distractions and disruptions. Additionally, measures to protect data privacy and confidentiality will be applied. In accordance with the EUI (2019) guidelines, personal information about the participants will be stored safely on a password-protected device and destroyed after one year by deleting electronic documents and shredding paper documentation. Identifying information, including names and e-mail addresses, will be replaced with identification numbers during data collection and analysis. No contact with patients will be made throughout the project, so no harm to them will be caused.
IRB approval to conduct the project will also be received, which means that the project will be done on a voluntary basis, and nurses will participate based on their motivation. The documentation supplied with the informed consent form will provide all relevant information about the project, including the ethical measures taken to protect the participants, their work, and data. No potential conflicts of interest were identified at this stage since the investigator is not connected to the hospitals or nurses who will participate in the project. Since this project may be published in scholarly journals, precautions will be taken to protect subjects’ privacy and confidentiality at the publication stage. The documents shown to third parties will be checked to ensure the absence of identifying information, and the publication will only reveal the findings and will not contain any identification numbers.
Limitations
While the project has been carefully designed to provide high-quality information on the problem and avoid bias, there are still two limitations related to its methodology. Firstly, the sample size of the study is smaller than in other quantitative studies in nursing (Cronin et al., 2014). New Jersey was chosen as the site of the project because of the need to conduct observations, and thus moving the project to another state would not be feasible. Additionally, the focus is on a coronary care unit, limiting the number of nurses in the sample. Enhancing the scope of the project would not help to achieve project goals because most other groups have a lower frequency of cardiac arrest and would thus provide incomplete data.
Hence, the chosen sample size is the best option given the geographic location of the project. Another limitation is that qualitative designs allow evaluating subjective knowledge only. While nurses’ perceived learning and their confidence in themselves to correctly perform and adapt to applying capnography in the clinical setting, this may not always be the case. This is because a quantitative correlational design would not allow considering qualitative information, such as the subjects’ attitudes and perceptions (Curtis et al., 2016).
This is a minor limitation to the project because nurses’ hesitance to use capnography may not only come from the lack of subjective knowledge but from perceived inadequacy of experience or skills. Nevertheless, this limitation can be prevented given the clinical questions, the selected design of the project, and the project potential to fulfill its purpose to identify knowledge deficits and correct them through educational means.
Summary
The purpose of this qualitative as well as quantitative correlational project is to explore the relationship between nurses’ knowledge of capnography and the use of this tool in coronary care units.
Although qualitative methodologies would be used to obtain necessary information into nurses’ perception of themselves with regards to capnography use; quantitative methodology is the best fit for the project’s purpose because it will provide objective data needed to establish the relationship between the variables (Barnham, 2015; Cronin et al., 2014). Additionally, the correlational design of the study is tailored to the needs of the project because it focuses on establishing the correlation between the two variables and its strength (Curtis et al., 2016). The data collection procedures that involve conducting quantitative observations and testing of nurses’ knowledge about the appropriate use of capnography through NKCT will provide adequate measurements of the variables presented (Kiekkas et al., 2016).
Descriptive statistics, scattergrams, correlation analyses, and regression analyses will also be applied to draw conclusions from the data sources provided as well (Pierce et al., 2017). The sequence of procedures chosen for the project will help to respond to clinical questions and fulfill the purpose of the project in evaluating and improving clinical practices.
Summary, Conclusions, and Recommendations
The project aimed at raising nurses’ awareness and competence regarding capnography during resuscitation of patients in coronary care unit have shown that training of nurses organized based on Kolb cycle method and within the concept of the diffusion of innovations has a potential to become a kind of standardized tool for the introduction of medical staff training on various technologies and processes in medical care.
During the implementation of project, training on capnography use in cases of cardiac arrest and coronary artery bypass surgery was conducted, with simultaneous application of the knowledge on practice. In the end of training process, randomized study with participation of the patients of coronary unit was conducted. The study showed high efficiency and accuracy of capnography as a method of monitoring respiratory function, thus contributing to the available data and discussion on the use of capnography as a method of monitoring.
Due to small amount of the sample of both nurses and patients, further studies are recommended with broader attraction of participants and in the units of different profiles.
References
Ali, Z., & Bhaskar, S. B. (2016). Basic statistical tools in research and data analysis. Indian Journal of Anaesthesia, 60(9), 662-669.
Aminiahidashti, H., Shafiee, S., & Sazgar, M. (2018). Applications of end-tidal carbon dioxide (ETCO2) monitoring in emergency department: A narrative review. Emergency, 6(1), e5.
Aramendi, E., Lu, Y., Chang, M., Elola, A., Irusta, U., Owens, P., & Idris, A. (2018). A novel technique to assess the quality of ventilation during pre-hospital cardiopulmonary resuscitation. Resuscitation, 132, 41-46. Web.
Austin, Z., & Sutton, J. (2014). Qualitative research: Getting started. The Canadian Journal of Hospital Pharmacy, 67(6), 436-440.
Barlow, J. (2016). Managing innovation in healthcare. London, UK: WSPC.
Barnham, C. (2015). Quantitative and qualitative research: Perceptual foundations. International Journal of Market Research, 57(6), 837-854.
Bullock, A., Dodington, J. M., Donoghue, A. J., & Langhan, M. L. (2017). Capnography use during intubation and cardiopulmonary resuscitation in the pediatric emergency department. Pediatric Emergency Care, 33(7), 457-461. Web.
Bureau of EMS, Trauma, & Preparedness. (2017). Procedures: End-tidal carbon dioxide monitoring. Web.
Campbell, C. M. (2017). An inside view: The utility of quantitative observation in understanding college educational experiences. Journal of College Student Development, 58(2), 290-299.
Carlisle, H. (2015). Promoting the use of capnography in acute care settings: An evidence-based practice project. Journal of Perianesthesia Nursing, 30(3), 201-208. Web.
Center for Innovation in Research and Teaching. (2020a). Quantitative approaches. Web.
Center for Innovation in Research and Teaching. (2020b). When to use quantitative methods. Web.
Cereceda-Sánchez, F. J., & Molina-Mula, J. (2017). Capnography as a tool to detect metabolic changes in patients cared for in the emergency setting. Revista Latino-Americana de Enfermagem, 25, 1-10. Web.
Chhajed, P. N., Gehrer, S., Pandey, K. V., Vaidya, P. J., Leuppi, J. D., Tamm, M., & Strobel, W. (2016). Utility of transcutaneous capnography for optimization of non-invasive ventilation pressures. Journal of Clinical & Diagnostic Research, 10(9), OC06-OC09. Web.
Chicote, B., Aramendi, E., Irusta, U., Owens, P., Daya, M., & Idris, A. (2019). Value of capnography to predict defibrillation success in out-of-hospital cardiac arrest. Resuscitation, 138, 74-81. Web.
Clark, V. L., & Ivankova, N. V. (2015). Mixed methods research: A guide to the field. New York, NY: SAGE Publications.
Conway, A., Collins, P., Chang, K., Mafeld, S., Sutherland, J., & Fingleton, J. (2019). Sequence analysis of capnography waveform abnormalities during nurse-administered procedural sedation and analgesia in the cardiac catheterization laboratory. Scientific Reports, 9(1). Web.
Cook, T., & Harrop-Griffiths, W. (2019). Capnography prevents avoidable deaths. BMJ, l439, 1-9. Web.
Cronin, P., Coughlan, M., & Smith, V. (2014). Understanding nursing and healthcare research. Thousand Oaks, CA: Sage.
Curtis, E. A., Comiskey, C., & Dempsey, O. (2016). Importance and use of correlational research. Nurse Researcher, 23(6), 20-25.
Darocha, T., Kosiński, S., Jarosz, A., Podsiadło, P., Ziętkiewicz, M., Sanak, T.,… Drwiła, R. (2017). Should capnography be used as a guide for choosing a ventilation strategy in circulatory shock caused by severe hypothermia? Observational case-series study. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 25(1), 15. Web.
de Caen, A., & Maconochie, I. (2018). EtCO2 measurement during pediatric cardiac arrest: Does the Emperor have no clothes? Resuscitation, 133, A1-A2. Web.
Dioso, R. P. (2014). Compression-only cardiopulmonary resuscitation as an assessment tool for nursing students – An evaluative literature review. Malaysian Journal of Nursing, 5(2), 44-49.
Duckworth, R. L. (2017). How to read and interpret end-tidal capnography waveforms. Journal of Emergency Medical Services, 42(8). Web.
Edelson, D. P., Yuen, T. C., Mancini, M. E., Davis, D. P., Hunt, E. A., Miller, J. A., & Abella, B. S. (2014). Hospital cardiac arrest resuscitation practice in the United States: A nationally representative survey. Journal of Hospital Medicine, 9(6), 353-357.
European University Institute. (2019). Guide on good data protection practice in research. Web.
Fawcett, J., & Ellenbecker, C. H. (2015). A proposed conceptual model of nursing and population health. Nursing Outlook, 63(3), 288-298.
Ferreira, M.S., Mendes R. T., Marson, F., Zambon, M. P., Antonio, M., Paschoal, I., … Ribeiro, J. (2017). Spirometry and volumetric capnography in lung function assessment of obese and normal-weight individuals without asthma. Journal de Pediatria, 93(4), 398-405.
Flanagan, S. M., Greenfield, S., Coad, J., & Neilson, S. (2015). An exploration of the data collection methods utilised with children, teenagers and young people (CTYPs). BMC Research Notes, 8(1), 61. Web.
Gong, Y., Lu, Y., Zhang, L., Zhang, H., Li, Y. (2015). Predict defibrillation outcome using stepping increment of poincare plot for out-of-hospital ventricular fibrillation cardiac arrest. Biomed Research International, 2015, 493472.
Gunnell, M. (2016). Research methodologies: A comparison of quantitative, qualitative and mixed methods. Web.
Guo, H., Kurokawa, T., Takahata, M., Hong, W., Katsuyama, Y., Luo, F.,… Gong, J. P. (2016). Quantitative observation of electric potential distribution of brittle polyelectrolyte hydrogels using microelectrode technique. Macromolecules, 49(8), 3100-3108.
Gutiérrez, J., Leturiondo, M., Ruiz de Gauna, S., Ruiz, J., Leturiondo, L., González-Otero, D., Zive, D.,… Daya, M. (2018). Enhancing ventilation detection during cardiopulmonary resuscitation by filtering chest compression artifact from the capnography waveform. PLOS ONE, 13(8), e0201565. Web.
Hamrick, J. T., Hamrick, J. L., Bhalala, U., Armstrong, J. S., Lee, J. H., Kulikowicz, E.,… Shaffner, D. H. (2017). End-tidal CO2–guided chest compression delivery improves survival in a neonatal asphyxial cardiac arrest model. Pediatric Critical Care Medicine, 18(11), 575-584. Web.
Harper, C. (2005). Capnography: Clinical aspects. Journal of the Royal Society Of Medicine, 98(4), 184.
Hartmann, S. M., Farris, R. W., Di Gennaro, J. L., Roberts, J. S. (2015). Systematic review and meta-analysis of end-tidal carbon dioxide values associated with return of spontaneous circulation during cardiopulmonary resuscitation. Journal of Intensive Care, 30, 426–35.
Hassankhani, H., Aghdam, A. M., Rahmani, A., & Mohammadpoorfard, Z. (2015). The relationship between learning motivation and self efficacy among nursing students. Research and Development in Medical Education, 4(1), 97-101. Web.
Heale, R., & Twycross, A. (2015). Validity and reliability in quantitative studies. Evidence-Based Nursing, 18(3), 66-67.
Heradstveit, B. E., & Heltne, J. K. (2014). PQRST–A unique aide-memoire for capnography interpretation during cardiac arrest. Resuscitation, 85(11), 1619-1620.
Hoff, I. L., Hoiseth, L., Kirkeboen, K. A., & Landsverk, S. A. (2019). Volumetric and end-tidal capnography for the detection of cardiac output changes in mechanically ventilated patients early after open heart surgery. Critical Care Research and Practice, Article 6393649. Web.
Ingham-Broomfield, R. (2014). A nurses’ guide to quantitative research. The Australian Journal of Advanced Nursing, 32(2), 32-38.
Israel, C. W. (2014). Mechanisms of sudden cardiac death. Indian Heart Journal, 66(1), 10-17.
Izrailtyan, I., Qiu, J., Overdyk, F. J., Ersion, M., Gan, T. J. (2018). Risk factors for cardiopulmonary and respiratory arrest in medical and surgical hospital patients on opioid analgesics and sedatives. PLoS One, 13, e0194553.
Jaffe, M. B. (2017). Using the features of the time and volumetric capnogram for classification and prediction. Journal of Clinical Monitoring and Computing, 31(1), 19-41. Web.
Jooste, R., Roberts, F., Mndolo, S., Mabedi, D., Chikumbanje, S., Whitaker, D., & O’Sullivan, E. (2018). Global capnography project (GCAP): Implementation of capnography in Malawi – an international anaesthesia quality improvement project. Anesthesia, 74(2), 158-166. Web.
Kalenda, Z. (1978). The capnogram as a guide to the efficacy of cardiac massage. Resuscitation, 6(4), 259-263. Web.
Kalmar, A. F., Allaert, S., Pletinckx, P., Maes, J. W., Heerman, J., Vos, J. J.,… Scheeren, T. W. L. (2018). Phenylephrine increases cardiac output by raising cardiac preload in patients with anesthesia induced hypotension. Journal of Clinical Monitoring and Computing, 1(1), 1-8. Web.
Katz-Buonincontro, J., & Anderson, R. (2018). How do we get from good to great? The need for better observation studies of creativity in education (Opinion article). Frontiers in Psychology, 9, 2342. Web.
Kerslake, I., & Kelly, F. (2017). Uses of capnography in the critical care unit. BJA Education, 17(5), 178-183. Web.
Kiekkas, P., Stefanopoulos, N., Konstantinou, E., Bakalis, N., & Aretha, D. (2016). Development and psychometric evaluation of an instrument for the assessment of nurses’ knowledge on capnography. Collegian, 23(1), 39-46. Web.
Kodali, B. S., & Urman, R. D. (2014). Capnography during cardiopulmonary resuscitation: Current evidence and future directions. Journal of Emergencies, Trauma, and Shock, 7(4), 332-340. Web.
Kolb, D. (1983). Experiential learning: Experience as the source of learning and development. Upper Saddle River, NJ.: Prentice Hall.
Kuisma, M., Salo, A., Puolakka, J., Nurmi, J., Kirves, H., Väyrynen, T., & Boyd, J. (2017). Delayed return of spontaneous circulation (the Lazarus phenomenon) after cessation of out-of-hospital cardiopulmonary resuscitation. Resuscitation, 118, 107-111. Web.
Lampe, J. (2017). Improved ventilation monitoring during CPR. Resuscitation, 110, A3-A4. Web.
Langham, M. L., Li, F. Y., Lichtor, J. L. (2016). Respiratory depression detected by capnography among children in the postanesthesia care unit: A cross-sectional study. Pediatric Anaesthesia, 10, 1010-1017.
Langham, M. L., Li, F. Y., Lichtor, J. L. (2017). The impact of capnography monitoring among children and adolescents in the postanesthesia care unit: A randomized controlled trial. Pediatric Anaesthsia, 27, 385-393.
Langhan, M. L., Shabanova, V., Li, F. Y., Bernstein, S. L., & Shapiro, E. D. (2015). A randomized controlled trial of capnography during sedation in a pediatric emergency setting. The American Journal of Emergency Medicine, 33(1), 25-30. Web.
Leppink, J., O’Sullivan, P., & Winston, K. (2016). On variation and uncertainty. Perspectives on Medical Education, 5(4), 231-234.
Leturiondo, M., Ruiz de Gauna, S., Julio Gutiérrez, J., M. González-Otero, D., M. Ruiz, J., A. Leturiondo, L., & Saiz, P. (2019). Waveform capnography for monitoring ventilation during cardiopulmonary resuscitation: The problem of chest compression artifact. Cardiac Diseases in 21St Century. Web.
Leturiondo, M., Ruiz de Gauna, S., Ruiz, J. M., Julio Gutiérrez, J., Leturiondo, L. A., González-Otero, D. M., … Daya, M. (2018). Influence of chest compression artefact on capnogram-based ventilation detection during out-of-hospital cardiopulmonary resuscitation. Resuscitation, 124, 63–68. Web.
Lin, T. Y., Fang, Y. F., Huang, S. H., Wang, T. Y., Kuo, C. H., Wu, H. T.,… Lo, Y. L. (2017). Capnography monitoring the hypoventilation during the induction of bronchoscopic sedation: A randomized controlled trial. Scientific Reports, 7(1), 8685-8687.
Lin, Y., Guerguerian, A., Laussen, P., & Trbovich, P. (2015). Heuristic evaluation of data integration and visualization software used for continuous monitoring to support intensive care: A bedside nurses perspective. Journal of Nursing Care, 4(300), 2167-1168. Web.
Link, M. S., Berkow, L. C., Kudenchuk, P. J., Halperin, H. R., Hess, E. P., Moitra, V. K., Neumar, R. W.,… Donnino, M. W. (2015). Adult advanced cardiovascular life support. Circulation, 132, 444-64.
Long, B., Koyfman, A., Vivirito, M. A. (2017). Capnography in the emergency department: A review of uses, waveforms, and limitations. Journal of Emergency Medicine, 53, 829-842.
Lui, C. T., Poon, K. M., & Tsui, K. L. (2016). Abrupt rise of end tidal carbon dioxide level was a specific but non-sensitive marker of return of spontaneous circulation in patient with out-of-hospital cardiac arrest. Resuscitation, 104, 53-58. Web.
Mader, T. J., Coute, R. A., Kellogg, A. R., & Harris, J. L. (2014). Coronary perfusion pressure response to high-dose intraosseous versus standard-dose intravenous epinephrine administration after prolonged cardiac arrest. Open Journal of Emergency Medicine, 2(1), 1-7. Web.
Martínez-Mesa, J., González-Chica, D. A., Bastos, J. L., Bonamigo, R. R., & Duquia, R. P. (2014). Sample size: How many participants do I need in my research? Anais Brasileiros de Dermatologia, 89(4), 609-615.
Merckx, P., Lambert, Y., Cantineau, J., & Duvaidestin, P. (1992). Effect of capnography on resuscitation efforts during CPR. Resuscitation, 24(2), 189. Web.
Monge García, M. I., Cano, A. G., Romero, M. G., Pintado, R. M., Madueno, V.P., & Monrove, J. (2012). Non-invasive assessment of fluid responsiveness by changes in partial end-tidal CO2 pressure during a passive leg-raising maneuver. Annals of Intensive Care, 2(1), 9-14.
Monnet, X.A., Bataille, E., Magalhaes, Barrois, J., Le Corre, M., Gosset, C., …, Teboul, J. L. (2013). End-tidal carbon dioxide is better than arterial pressure for predicting volume responsiveness by the passive leg raising test. Intensive Care Medicine, 39(1), 93-100.
Morse, J. M. (2017). Analyzing and conceptualizing the theoretical foundations of nursing. New York, NY: Springer.
Nassar, B. S., & Schmidt, G. A. (2016). Capnography during critical illness. Chest, 149(2), 576-585.
Nassar, B., & Kerber, R. (2017). Improving CPR performance. Chest, 152(5), 1061-1069. Web.
Nelson, D. (2018). Quantitative observation: definition and examples. Web.
Novais, P. M., & Moreira, M. M. (2015). Capnography: A feasible tool in clinical and experimental settings. Respiratory Care, 60(11), 1711-1713. Web.
Pantazopoulos, C., Xanthos, T., Pantazopoulos, I., Papalois, A., Kouskouni, E., & Iacovidou, N. (2015). A review of carbon dioxide monitoring during adult cardiopulmonary resuscitation. Heart, Lung and Circulation, 24(11), 1053-1061. Web.
Poth, C. (2018). Innovation in mixed methods research: A practical guide to integrative thinking with complexity. New York, NY: SAGE Publications.
Price, P. C., Jhangiani, R. S., Chiang, I. A., Leighton, D., & Cuttler, C. (2017). Research methods in psychology (3rd ed.). Web.
Ristagno, G., Mauri, T., Cesana, G., Finzi, A., Fumagalli, F., Rossi, G., Grieco, N.,… Azienda Regionale Emergenza Urgenza Research Group. (2015). Amplitude spectrum area to guide defibrillation: A validation on 1617 patients with ventricular fibrillation. Circulation, 131(5), 478–87.
Rogers, E. M. (1995). Diffusion of innovations. Glencoe, IL: Free Press.
Rowley, J. (2014). Designing and using research questionnaires. Management Research Review, 37(3), 308-330.
Ruiz de Gauna, S., Leturiondo, M., Gutiérrez, J., Ruiz, J., González-Otero, D., Russell, J., & Daya, M. (2018). Enhancement of capnogram waveform in the presence of chest compression artefact during cardiopulmonary resuscitation. Resuscitation, 133, 53-58. Web.
Sahyoun, C., Siliciano, C., & Kessler, D. (2018). Use of capnography and cardiopulmonary resuscitation feedback devices among prehospital advanced life support providers. Pediatric Emergency Care, 1-8. Web.
Sanjari, M., Bahramnezhad, F., Fomani, F. K., Shoghi, M., & Cheraghi, M. A. (2014). Ethical challenges of researchers in qualitative studies: The necessity to develop a specific guideline. Journal of Medical Ethics and History of Medicine, 7, 14. Web.
Saunders, R., Struya, M., Pollock, R., Mestek, M., Lightdale, J. (2017). Patient safety during procedural sedation using capnography monitoring: A systemic review and meta-analysis. BMJ Open, 7, e013402.
Sheak, K. R., Wiebe, D. J., Leary, M., Babaeizadeh, S., Yuen, T. C., Zive, D.,… Abella, B. S. (2015). Quantitative relationship between end-tidal carbon dioxide and CPR quality during both in-hospital and out-of-hospital cardiac arrest. Resuscitation, 89, 149-154. Web.
Sipmann, F., Bohm, S., & Tusman, G. (2014). Volumetric capnography: The time has come. Current opinion in critical care, 20(3), 333-339.
Smith, M. J., & Liehr, P. (Eds.). (2018). Middle range theory for nursing (4th ed.). New York, NY: Springer Publishing Company.
Soar, J., Nolan, J. P., Bottiger, B. W., Perkins, G. D., Lott, C., Carli, P., Pellis, T.,… , Deakin, C. D. (2015). Adult advanced life support. Resuscitation, 95, 100-147.
Stites, M., Surprise, J., McNiel, J., Northrop, D., & De Ruyter, M. (2017). Continuous capnography reduces the incidence of opioid-induced respiratory rescue by hospital rapid resuscitation team. Journal of Patient Safety, 1-10.
Subramani, Y., Singh, M., Wong, J., Kushida, C., Mahotra, A., Chung, F. (2017). Understanding phenotypes of obstructive sleep apnea: applications in anesthesia, surgery and perioperative medicine. Anesthesia Analgesia, 124, 179-191.
Tobi, K. U., & Amadasun, F. E. (2015). Cardio-pulmonary resuscitation in the intensive care unit: An experience from a tertiary hospital in Sub-Saharan Africa. Nigerian Medical Journal: Journal of the Nigeria Medical Association, 56(2), 132-137. Web.
Turle, S., Sherren, P., Nicholson, S., Callaghan, T., & Shepherd, S. (2015). Availability and use of capnography for in-hospital cardiac arrests in the United Kingdom. Resuscitation, 94, 80-84. Web.
Urman, R., & Kodali, B. (2014). Capnography during cardiopulmonary resuscitation: Current evidence and future directions. Journal of Emergencies, Trauma, And Shock, 7(4), 332. Web.
Venkatesh, H., & Keating, E. (2017). BET 1: Can the value of end tidal CO2 prognosticate ROSC in patients coming into emergency department with an out-of-hospital cardiac arrest (OOHCA)? Emergency Medicine Journal, 34(3), 187-189. Web.
Watson, R. (2015). Quantitative research. Nursing Standard, 29(31), 44-48. Web.
Whitaker, D., & Benson, J. (2016). Capnography standards for outside the operating room. Current Opinion in Anaesthesiology, 29(4), 485-492. Web.
Wright, S. (2017). The case for procedural capnography. Web.
Yang, Y., Huang, G., Tang, R., Chen, Q., Hui, X., Li, Y., Yu, Q., … Qiu, H. (2014). Optimization of Positive End-Expiratory Pressure by Volumetric Capnography Variables in Lavage-Induced Acute Lung Injury. Respiration, 87, 75-83.
Yen, P. Y., Kelley, M., Lopetegui, M., Rosado, A. L., Migliore, E. M., Chipps, E. M., & Buck, J. (2016). Understanding and visualizing multitasking and task switching activities: A time motion study to capture nursing workflow. In AMIA Annual Symposium Proceedings (pp. 1264-1273). Bethesda, MD: American Medical Informatics Association.
Zyphur, M. J., & Pierides, D. C. (2017). Is quantitative research ethical? Tools for ethically practicing, evaluating, and using quantitative research. Journal of Business Ethics, 143(1), 1-16.