Introduction
Cancer is often a fatal disease if not detected early. The word has such a sinister or terrifying connotation that it has been extensively used as metaphorically to describe negative aspects of any kind. One comes across such clichés as ‘violence is a cancer in our society’ quite often. Huge advancement in research and technology has to a certain extent been successful in treating cancer to a large extent. But even now, the basic cause and a full cure of all types of cancers are still to be discovered. The reaction of a person when he comes to know that he or she has cancer is usually one of profound shock even if the attending physician assures that the disease can be cured. There have been countless instances where people have been able to get rid of the abnormality though proper treatment and care. This paper is a study of the changes in cancer survival, prognostic ability, monitoring, impact of treatment strategies and the latest advances in this area. The period of study is limited to the last thirty years. A brief review about the history of the disease and early treatment methods will also be done.
History of cancer
Archaeological finds indicate the cancer was in existence even during the Neolithic period. An instance is the drawings from the period found in Malta. The drawings of human beings have abnormal protrusion or swelling of the abdomen and groin areas. (Micozzi, p.29).
The book also gives another instance, this time of figurines found in Greece and Yugoslavia, having similar deformities. More compelling evidence of the existence of cancer was found in Egyptian papyrus scrolls now referred to as the Edwin Smith papyrus, Ebers papyrus and the Kahun papyrus. All these date back to a period around year 1800 BC and were thought to be either a medical, surgical or even gynaecological texts (because the explanations indicated breast cancer). The ancient medical texts of India’s Ayurveda also mentions about treatment and prevention of cancer. (Complementary and Alternative Therapies for Cancer Patients). The disease was also described by Hippocrates who is said to have coined the name cancer which is Greek for crab. “Hippocrates used the terms carcinos and carcinoma to describe non-ulcer forming and ulcer-forming tumours. In Greek these words refer to a crab, most likely applied to the disease because the finger-like spreading projections from a cancer called to mind the shape of a crab.” (The History of Cancer: Origin of the Word Cancer).
Cancer and modern medicine – A timeline of treatments
It was during the 19th and 20th centuries that rapid strides in the treatment of cancer began. The first initial operations done to remove tumour was by Bilroth and Handley from Germany and England respectively. Soon radical mastectomy was developed by the 19th century surgeon William Stewart Halsted. Other treatments include oophorectomy developed by Thomas Beatson (late 19th century), radiation (fag end of 19th century), Hyperthermia, Boron neutron capture therapy, Liposomal therapy, Monoclonal antibodies, etc. The above information was sourced from the website of the American Cancer Society mentioned in the earlier section. Chemotherapy was first performed using nitrogen mustard gas in 1946.
Cancer Survival
As mentioned earlier cancer may not turn out to be fatal if diagnosed and treated in its early stages. Review of the latest advancement in allopathic treatment of cancer is given at the end of this paper before the conclusion. Apart from advances in medicine and technology, some of the factors that are shown to decrease mortality are proper exercise, diet, adequate intake of nutrients and even exposure to sunlight to obtain Vitamin D. “A recent study conducted by researchers from the Swedish Medical University Karolinska Institutet (SMUKI) suggests that men who exercise regularly may less likely to die from cancer compared to sedentary ones.” (Exercise May Increase Cancer Survival Rates in Men). According to the British Journal of Cancer, oral treatment using “Seocalcitol (EB1089), a vitamin D analogue, can inhibit growth, induce differentiation and induce apoptosis of cancer cell lines in vitro and can also inhibit growth of pancreatic cancer xenografts in vivo.” (Evans et al, 680-685). With regard to nutrition, a study using Alpha-Tocopherol and Beta-Carotene had shown a reduction of 41% in mortality in patients with prostate cancer. (Nutrition in Cancer Care). With all the advancements in medicine, cancer research and the above mentioned factors cancer survival rates are increasing, especially in more developed economies like the UK, USA, Australia and many parts of Europe. There are reports from recognized organizations and news sources from all these countries which agree with the above statement. Analyzing proper cancer rate survival is quite difficult and impractical because of the sheer variety of the disease and the widely different mortality rates associated with each type of cancer. A few examples are cited here from the study conducted by L K Smith et al of the Department of Epidemiology and Public Health, UK gives five and ten year survival rates for different types of cancers. The study included a cohort as well as a period study of cancer patients in the country. The “Period analyses are defined by a recent time interval in which patients’ survival experience is observed. It excludes short-term survival of patients diagnosed before the start of the period but includes their long-term survival within the period.” (Materials and Methods). A few of the results are discussed below to illustrate the vast differences in survival rates among different types of cancers and also to see whether the ten and five year studies have any similarities for each type of cancer. For the ten year cohort study, the lowest survival rates were found in cancers of the pancreas (2.7%), liver (3.1%), oesophagus (6.2%) and multiple myeloma (8.0%). Better survival rates were found in cancers of the rectum (32.3%), and colon (34.8%). The highest survival rates were found in cancer of the testis (87.7%) followed by uterus cancer (68.6%), thyroid cancer (66.5%) and Melanoma of the skin (65.4%). (Smith, Lambert and Jones). This proves that different types of cancers have different (sometimes very high) mortality rates. The five year survival rates for the above mentioned cancers (cohort group) are also given below. Pancreas has a survival rate of 3.1%, liver cancer has a survival rate of 3.6%, cancer of the oesophagus has a survival rate of 7.3% and multiple myeloma has a survival rate of 20%. In the case of cancers which had a better chance of survival the figures is cancer of the rectum which has a survival rate of 38.7%, and colon cancer has a survival rate of 40.3%. For those types of cancers which had the highest rate of survival, the five year study figures are testis cancer (90.6%), uterus cancer (71.2%), thyroid cancer (72.4%) and melanoma of the skin 77.3%. The full table is given below for a more detailed reference.
The figures observed are not very encouraging because the survival rates for the ten years shown a decline in the life expectancy of the patients even though it is only marginal. This indicates that mortality rates increase when the period of study is increased. Once diagnosed, the chances of survival declines as time go by. This is quite beyond doubt since the time when the disease was diagnosed is uniform among both groups. According to the study, the period of diagnosis for the cohort and period group for the five year study was 1986 to 1990 and the period of diagnosis for the year study (for both groups) was 1981 to 1985. The highest mortality in the intervening period of five years following the five year study was for the following types of cancers. The figures given in brackets are the survival rates for the five year study followed by the survival rates in the ten year study. The figures are for multiple myeloma (8% and 20%), cancer of the breast (50.6% and 67.1%) and cancer of the brain (9.5% and 15.4%).
Cancer Trends in the UK
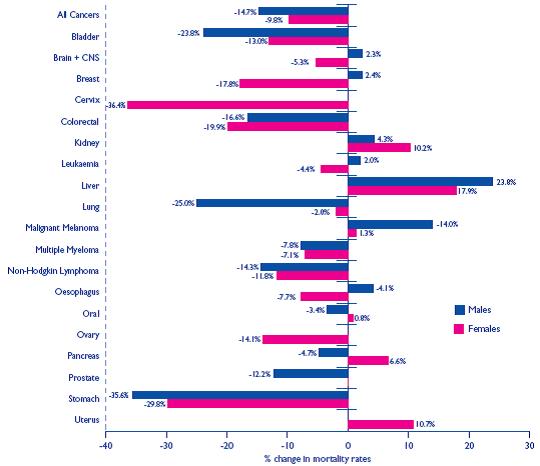
Studies have shown that survival rates of almost all types of cancers have increased over the last decade or so. “Mortality rates have fallen for most types of cancer over the past 10 years. The largest falls have been for stomach and cervical cancer. Rates have increased for cancers of the liver and uterus, for malignant melanoma and non-Hodgkin lymphoma.” (Source: Cancer Stats: Mortality UK, p.2). A chart showing the figures are given below.
While this trend is welcome, the number incidence of cancer has been increasing which is quite alarming. According to Cancer Research UK the “Overall, cancer mortality is decreasing, despite the increasing incidence of the disease. Over the past 10 years (1996-2005) the age standardized mortality rates for all malignant neoplasms fell by 12%: around 15% for men and 10% for women.” (Mortality Trends, p.1). There is also a difference in the type of cancer prevalent among men and women. The different types of cancers that cause death among men and women (respectfully) are given below. The figures are applicable to the year 2005.
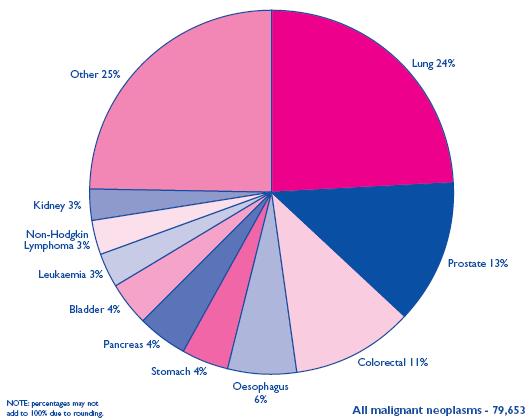
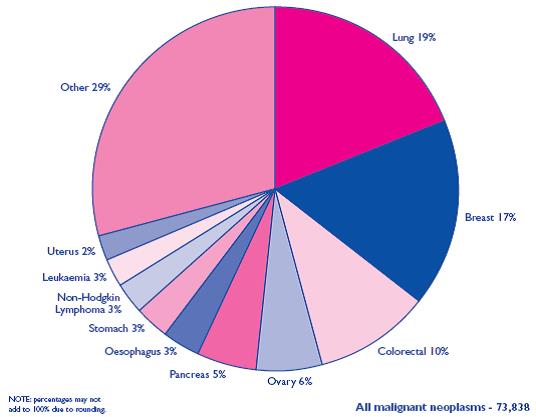
Lung cancer is the biggest killer of all types for both men and women. The next highest causality is caused by prostrate cancer for men and breast cancer for women. It appears to be a coincidence that both these types of cancer are sex specific. Mortality is also higher among the elderly population above 65 years of age. The mortality rate for this age group is nearly 76%. The age wise distribution of cancer deaths in the country is given as a chart below.
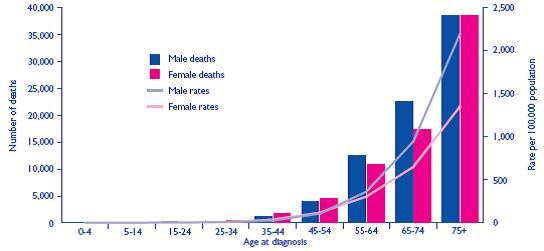
It can be seen that while there is no or negligible deaths from the disease up to age 44, the mortality rate begins to climb rather steeply after that period. There is also a significant difference among mortality rates in men and women. Under the 65 year age group, 47% of women succumbed to the disease while the rate for men was considerably lower and stood at 31%. Studies on this area point out to a positive correlation between body mass index and incidence of this disease. “Although it is widely accepted that body mass index (BMI) is positively associated with cancers of the colon, endometrium, and kidney, adenocarcinoma of the oesophagus, and postmenopausal breast cancer, the magnitudes of such effects and the role of BMI in the development of other, rarer, cancers are less certain.” (Reeves, et al, p.1134). This statement is from an article published in the British Medical Journal which was based on a comprehensive and large-scale study involving nearly 1.3 million women in the UK (age group between 50 and 64 years). The purpose of the study was to see whether there is a positive correlation between incidence and body mass index for other types of cancers as well. The body mass index was classified in the following manner namely 22.5, 22.5-24.9, 25.0-27.4, 27.5-29.9, and 30 and above. A body mass index between 25.0 and 30.0 was considered as overweight and the body mass index above this range was considered to be obese. The period of study was 5.4 years. The findings of the study were as follows. “High body mass index in women may increase the risk of multiple myeloma, leukaemia, pancreatic cancer, non-Hodgkin’s lymphoma, and ovarian cancer Menopausal status seems to affect the relation between body mass index and risk of breast cancer, endometrial cancer, and colorectal cancer Among postmenopausal women in the UK, 5% of all cancers (about 6000 annually) are attributable to women being overweight or obese Around half of all cases of endometrial cancer and adenocarcinoma of the oesophagus in postmenopausal UK women are attributable to women being overweight or obese.” (Reeves, et al, p.1138). In the case of men, prostate cancer is the most common among all cancers and the incidence of the disease is on the rise. According to an online article published by Cancer Research UK, prostate cancer incidence has risen rapidly over the years, even though mortality rates have remained more or less constant. This indicates that survival rates from this form of cancer have increased due to better and more advanced treatments.
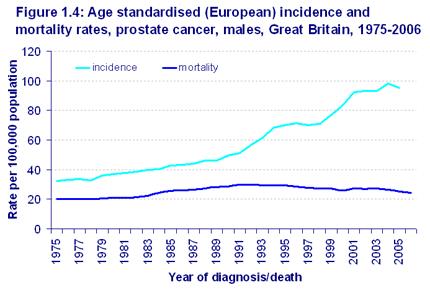
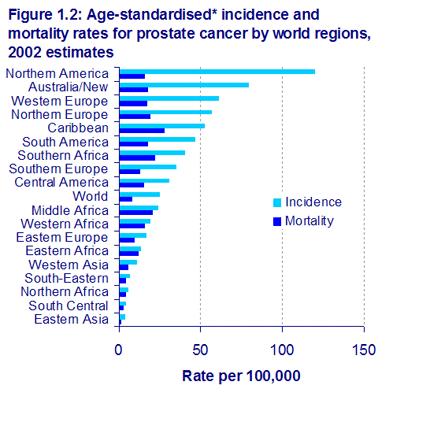
No particular reason was attributed to this increase. Prostate cancer risk is high in men above sixty years of age and increases drastically once they are past seventy years or older. Some of the factors apart from age that are attributable to the incidence of prostate cancer are given below. African Americans are more at risk of incidence than whites though the prevalence of this disease is very low in Asian countries. Family history of prostate cancer also seems to be a contributing factor. An area wise breakup of incidence and mortality is given below to illustrate the huge variance rates from different regions of the world.
Latest advances in cancer treatment
So much of research is going on in this area that it is difficult to provide a comprehensive review and hence only a random overview will be provided. New an improved advancement of the molecular biology of cancer has introduced new treatments in the cancer treatment. Some of the cancer treatment methods that are currently being tested in clinics include using matrix metalloproteinase inhibitors, gene therapy, immunotherapy etc. Using the matrix metalloproteinase inhibitors, the patients of advanced gastric, pancreatic and ovarian cancer are treated. It may also be found effective in hormonal treatments and also in adjuvant therapy for patients who are suffering from high risk of disseminated diseases. Gene therapy will change the disorders between the misaligned and the normal cells, whereas immunotherapy will modify the tumour cells so that it improves immune detection and in turn will enhance the cancer control and its treatment. (Tattersall and Thomas, p.445-448).
There are many latest advances made in the field of cancer treatment. One of the major advancement is Adjuvant therapy, which make use of chemotherapy subsequent to the surgical procedure so as to bring down the risk of cancer recurrence and to increase the cure rates. This method is developed especially for the people who are suffering from the early stages of breast, lung and colon cancers. Then there are targeted therapies which are targeted to a wide range of cancers like breast, colon, lung, kidney, head, and neck cancer. It also prevents the reoccurrence especially for lung and colorectal cancer. Bevacizumab (Avastin) also reduces the risk of re-occurrence of the colorectal cancer since it was found that by mixing bevacizumab with chemotherapy enclosing the drug oxaliplatin will considerably increase the survival rate among the cancer patients. New vaccines were introduced in order to prevent the infection caused by Human Papilloma Virus (HPV), which is a virus linked to the cause of cervical cancer. These vaccines were really effective in preventing 90 percent infections caused due to HPV. Another major theme in latest cancer advances is survivorship. In the cancer survivor ship, the degree and rigorousness of the long term health problems faced by numerous childhood cancer survivors are easily recognized and cured. The other major advances include the introduction of Trastuzumab (Herceptin). Studies have proved that by adding the Trastuzumab to standard chemotherapy in the early stages of breast cancer will reduce the risk of re-occurrence of HER-2-positive early stage breast cancer to half. It also reduces the risk of death to one third of those cancer patients whose early stages of breast cancer includes extreme amounts of the HER-2-protein when compared to standard chemotherapy. A new treatment with a newly introduced drug called Lenalidomide (RevLimid) was used for the treatment of myelodysplastic syndrome (MDS), which is a disorder in the blood forming cells and will cause leukaemia. The use of lenalidomide will reduce the genetic irregularity and also lessens the want for blood transfusion. An effective drug was introduced for the treatment of brain tumour, called temozolomide, which will help the glioblastoma patients to survive for a longer period. (Top Advances in Cancer Treatment for 2005 Chosen by Oncologists).
An external beam radiation therapy is effective for the treatment of vaginal brachytherapy. It will diminish the effect of re-occurrence of endometrial cancer with fewer side effects. Gemcitabine (Gemzar) is another effective medicine which was recently introduced increases the endurance of those patients who have undergone surgery for pancreatic cancer. This is a significant advancement since only few medicines were available for the treatment of pancreatic cancer. Another advancement is in the treatment of kidney cancer patients. With the introduction of a new advanced therapy called everolimus (RAD001, Cetican) will increase the survival of those patients whose cancer has been progressed after many other treatments. (Advances in Cancer Treatment and Quality of Life).
Alternative and complementary therapies
Due to the inherent danger and the longevity of the treatment involved, many people now look at alternative and complementary treatments in order to find relief and cure. Alternative systems of treatment indicate that people who opt for it stop conventional allopathic treatments and completely switch over to a single or combination of such therapies. Complimentary therapy is a more cautious approach where patients will continue with conventional treatment, but will in addition take recourse to other non-conventional therapies as well. The main problem with both the above forms is that very little clinical evidence is available for allopathic medical practitioners to advice people to go in for such alternative or complementary courses of action. In most cases it is the patients themselves who will opt for this based upon the advice of friends, families and other well-wishers. Complimentary and alternative medicine referred to as CAM “may include dietary supplements, megadose vitamins, herbal preparations, special teas, acupuncture, massage therapy, magnet therapy, spiritual healing, and meditation.” (Complementary and Alternative Medicine). The American Cancer Society provides useful information to patients and their families regarding these forms of treatments. While they do not claim that none of these are effective for a complete cure, an advice is provided for patients to consult with their medical team before starting complementary therapy. “The American Cancer Society urges patients who are thinking about using any complementary or non-mainstream treatments to discuss this with their health care team.” (Complementary and Alternative Methods for Cancer Management: Complementary Therapy). Most governments have problems in control of alternative and complementary therapies since such treatments do not come under the prerogative of their health related statutes. The American Cancer Society warns that such a situation will provide an opportunity for quacks and fraudsters to make money by cheating ill informed patients and their families. The Society gives an additional warning that not all such therapies that come under the classification of CAM are free from side effects as most people erroneously think. In this instance, only the existence of such therapies can be mentioned for the sake of information and no recommendations as to opting for any CAM therapies are done. But many therapies like nutrition supplements and meditation can be used to relieve many of the side effects of cancer treatment that are common in the allopathic treatment of cancer. They include managing stress, and recovery of health damaged though radiation and chemotherapy.
Conclusion
Thirty years of cancer research has brought considerable advances in the treatment and management of this dreaded disease. But concerns still exist mainly due to the higher incidence of cancer among the population. Living conditions, pollution, stress poor eating habits, lack of proper nutrition and exercise etc are some of the factors attributable to this phenomenon. The chart that showed changes in mortality rates over the past ten years still show no dramatic improvements. The ten year period have only brought about a maximum 36% reduction of cervical cancer deaths and a 35% reduction in stomach cancer deaths (both are male statistics). Reduction in mortality of other types of cancers range from a high of 25% in the case of lung cancer to a low of 3% in the case of oral cancer. The higher mortality rate for women is also another area of concern. This holds good for most types of cancers. For example, the reduction in mortality rates for men in the case of lung cancer is nearly 25% whereas in the case of women patients the figure is as low as 2%. Prostate and breast cancer incidence is also rising for men and women respectfully. Increase in incidence of other types of cancers is also there. This is despite the fact that governments in most advanced economies are bringing out public policies that are aimed at awareness and prevention of the disease. The disease is still a killer of men and women and it will take more time, effort, research and a lot of care until this quirk of nature can be defeated.
Works Cited
- Advances in Cancer Treatment and Quality of Life. ASCO: American Society of Clinical Oncology.
- Cancer Stats: Mortality UK. Cancer Research. 2007.
- Complementary and Alternative Medicine. National Cancer Institute. Web.
- Complementary and Alternative Methods for Cancer Management: Complementary Therapy. American Cancer Society. 2008. Web.
- Complementary and Alternative Therapies for Cancer Patients. University of California. Web.
- Evans, T. R. J., et al. A Phase II Trial of the Vitamin D Analogue Seocalcitol (EB1089) in patients with Inoperable Pancreatic Cancer. BJC: British Journal of Cancer. (2002). Web.
- Exercise May Increase Cancer Survival Rates in Men. Free Press Release.
- Materials and Methods. British Journal of Cancer. 2003. Web.
- Micozzi, Mark S. Documentary Evidence for Cancer in Antiquity. Complementary and Integrative Medicine in Cancer Care and Prevention. 2006. Web.
- Mortality Trends. Cancer Research. 2007.
- Nutrition in Cancer Care. National Cancer Institute. 2008. Web.
- Prostate Cancer: Geographic Variation in Prostate Cancer Incidence. Cancer Research UK. 2008. Web.
- Prostate Cancer: Trends in Prostate Cancer Incidence. Cancer Research UK. 2008.
- Reeves, Gillian K., et al. Cancer Incidence in Mortality in Relation to Body Mass Index in the Million Women to Study: Introduction. BNJ. 2008. 335.
- Reeves, Gillian K., et al. Cancer Incidence in Mortality in Relation to Body Mass Index in the Million Women to Study: What this Study Adds. BNJ. 2008. 335.
- Smith, L. K., Lambert. P.C., and Jones. D. R. Up to Date Estimates of Long Term Cancer Survival in England and Wales. BJC: British Journal of Cancer. 2008.
- Smith, L. K., Lambert. P.C., and Jones. D. R. Long Term Cancer Survival Estimates. BJC: British Journal of Cancer. 2008. Web.
- Tattersall, Martin H L., and Thomas Hilary. Recent Advances: Oncology. BMJ. 318. 1999. Web.
- The History of Cancer: Origin of the Word Cancer. American Cancer Society. 2008. Web.
- Top Advances in Cancer Treatment for 2005 Chosen by Oncologists. Senior Journal: Today’s News and Information for Senior Citizens and Baby Boomers. 2005.