Acknowledgements
The ability to complete this research could never have achieved without the encouragement and understanding of my family and specially Rayan my brother, who endured from did not back to home country for long time.
I wish to express my gratitude to my supervisors Carol Holder and Nasser Khan, who organised presentation of the answer of research question and their collaboration. As well as, one of the people who provided the greatest amount of help is Dr. Keith Salmon, for his help and support in whole period of my program.
I am also appreciative to my colleagues in Iinternational Medical Centre (IMC), a most sincere thank you is expressed to SamerAbughazaleh my former director for his contribution, his knowledge and expertise in the principles of teaching and learning and for loyalty and steadfastness during the writing of my research. RashaKhonjee who has provided that, phases of Joint Commission International (JCI) implementation in IMC and studies in the theory of International accreditation standards also FatemahRashed helped me to contact with executive staff of IMC. I am also grateful to MajdahShugdar for making many helpful suggestions of structural setting and clarified a significant of JCI. In addition, I would like to appreciate the staff at IMC, especially total quality management department for their cooperation during the interviews and questionnaires.
Finally, utmost gratitude is extended to Bassma and AmalAltoaimi for making specific suggestions that have entered into the revision. I owe a particular debt to some friends, who have had many unsolicited but welcome reactions from various readers. Their names are too many to mention but I owe a particular debt to most important persons for their careful reading of my research.
Abstract
Background
In recent times, the Joint Commission International (JCI) Accreditation Standards for Hospitals have considered a promising tool for recovering total quality management and patient safety. Nevertheless, the impact of JCI accreditation standards on healthcare services and on organisational behaviour has an inconsistent and fragmented record (Informaworld, 1991). Successful implementation of accreditation standards does not necessarily mean that quality has been embedded in the daily culture and practices of an organization. Improving and maintaining the quality of healthcare services takes more than just implementing standards.
Purpose
The purpose of this research is to investigate to what extent the Joint Commission International (JCI) Accreditation standards improve healthcare facilities. Additionally, to understand from Western literature the barriers and facilitators those are essential to embed quality in the organizational culture of Saudi Arabian healthcare organizations.
Scope
The scope of this dissertation comprises the total quality management development of healthcare facilities by Joint Commission International Accreditation Standards in hospitals of Kingdom of Saudi Arabia.
Methods
Two methods have been utilised in order to meet the objective of the study. Firstly, a literature review has been undertaken to observe existing literature on JCI accreditation standards for hospitals after compares and contrast with six-sigma. Secondly, telephone interviews and executive staff questionnaires have been conducted with staff members from the International Medical Centre in KSA, which has signed an agreement with JCI making it the first hospital in the Gulf area to involve the JCI in a project from its inception (International Medical Centre, 2000b).
Results of this research may lead to
- Avoidance of medical care errors.
- Warning of a wrong procedure or a patient surgical mistake.
- Prevention of uninterrupted medication errors.
- Regular dosages of anaesthesia to prevent errors.
- Promote infection through paying attention to hand hygiene.
Recommendation
Healthcare facilities organisations have recommended implementing Joint commission International compulsory accreditation standards in Kingdom of Saudi Arabia (KSA).
Conclusion
There is an absence of quality culture accreditation standards, which have been considered an effective tool to embed quality in Saudi Arabian hospitals. There are many factors, which may enhance or inhibit the embedding of quality, the main factors being belief in the impact of change, teamwork, leadership support, and a top down approach to management.
Introduction
According to Jovanovic (2008), healthcare organisations have been faced with challenges in the past few years. These challenges are in regards to the improvement of safety and quality healthcare services. The voices who determine quality improvements come from key stakeholder groups such as the government, the Ministry of Health, healthcare insurance fund, healthcare associations, health-care professionals, patients and their families, the public, etc. In addition, international agencies, World Health Organisation (WHO), and World Bank, promote the improvement and development of quality and safety of healthcare services. In order to achieve the desired improvements in healthcare services, investment and the additional resources are not always enough. Accreditation standard for hospitals illustrate an interesting methodology for significant improvements in regards to healthcare. In order to improve the quality of healthcare services and processes, ensure the safety of the environment, and prevent or reduce risk to patients and staff, achieving the accreditation standards is highly crucial. In addition, there is the benefit that it helps healthcare providers to identify the strengths and weaknesses of their own organisations (Jovanovic, 2008).
KSA healthcare is interested in healthcare accreditation standards. She has focused on self and external appraisals in order to evaluate their performance against that of set accreditation standards and work towards improving the healthcare sector by following recommended methods. On the other hand, accreditations not only for standards setting to the procedure but there is counselling, analytical and improvement measurements. Furthermore, measures such as reduction of medical errors, evidence medicine and quality assurances are used to gauge the healthcare organizations because they are important in the accreditation process. Thus, hospital accreditation is one major key in ensuring patient safety (Tabish, 2010).
Healthcare service and healthcare organizations are crucial in any organized society fit for human habitation and the healthcare sector takes a chunk of the resources found in any particular society. Due to the vital role that the healthcare organizations play in the society they ought to be safe for all the stakeholders that is patients , staff and general public (World News, 2011). The Quality of hospitals and healthcare services is also of great interest to many other bodies, including governments, NGOs targeting healthcare and social welfare, professional organisations representing doctors, patient organisations, shareholders of companies providing healthcare services, etc. How quality has-been maintained and improved in hospitals and healthcare services are the subject of much debate. Hospital surveying and accreditation are recognised means by which this has achieved (World News, 2011).
After compare and contrast some of hospitals standards with Joint Commission International (JCI), it is found that, JCI as a universal accreditation standard, which is stand-alone in the world, provides unique tools designed to provide quantifiable benchmarks for patient care quality and drive positive changes that have noticed by clinical staff, patients and management. In view of that, JCI remains competitive with the latest quality and safety information (Joint Commission International, 2011a).
World News (2011) clarified that, JCI are not just an issue of hospital quality. There are financial factors as well. For example, in the USA up until recently, the JCI exercised a de facto veto over whether or not USA hospitals and other health providers were able to participate; and therefore earn from the Medicare and Medicaid programs. “Medicare can be defined as a health insurance program for people age 65 or older. People under age 65 with certain disabilities, and people of all ages with end-stage renal disease (permanent kidney failure requiring dialysis or a kidney transplant), and Medicaid is a state administered program and each state gets its own guidelines regarding eligibility and services” (The Centres for Medicare & Medicaid Services, 2005a&b).
Many organisations are motivated to implement JCI accreditation standards for a range of reasons. Exceeding patient expectations might be the main motivator for these firms. However, the most important thing is how to understand JCI accreditation standards and how to employ the objectives, policies, standards and measurements with which to meet them. Therefore, the new direction now taken by the Saudi healthcare sector aims to follow this new philosophy in order to face deficiencies that exist in the public and private sectors that implementation has produced in privet hospitals(World News, 2011).
Research Question
To what extent does Joint Commission International Accreditation standards improves healthcare facilities?
Aims and objectives
The aims of this research are to evaluate and analyse the extent to which JCI’s international standards have been applied in Saudi Arabia, and to what degree they have followed through assessing the different factors involved in Total Quality management (TQM).
The objectives of this study are:
- To explore the introduction of TQM in Saudi hospitals,
- To understand how Saudi hospitals could implement TQM properly,
- To help healthcare policy makers, managers and health professionals to implement TQM correctly.
- To understand the significance of the purpose and goals of JCI in Healthcare sector.
- To assess the International Essentials for Health Care Quality and Patient Safety according to JCI accreditation standards.
- To assess the extent to which healthcare facilities have improved throughout the implementation of JCI medical care, patient rights, patient satisfaction.
- To analyse the consistent implementation of the mission of IMC in KSA following the international standards of JCI accreditation.
Limitations and Opportunities
In conducting this research, some limitations and opportunities may be encountered in both the primary and secondary research. Through the primary research, the limitations may arise in the performance of telephone interviews and subsequent analysis of the answers. Within the secondary research, the limitations may include the reliability of the information, and the confidentiality of some information. In addition, some information that is acquired may be outdating.
This research will be an opportunity for the Saudi and Non-Saudi public to understand if IMC has achieved its international accreditation standards in healthcare facilities with its vision “to pioneer a unique approach of healing the body, mind and soul and applying the best international healthcare standards and pursuing divine ethics”(International Medical Centre, 2008).
This research may also provide an opportunity for me to apply for a PHD degree in International Public Healthcare area to research the health economics and Services of Life in international public healthcare. Therefore, it would be very interesting for me to accumulate as much information as possible to answer my research question.
Literature Review
Introduction
The culture in Saudi Arabia has had a great influence on healthcare issues. The population of Saudi Arabia is a mixed society consisting of nomadic Bedouin tribes and other sedentary inhabitants (Al-rasheed and Robert, 2006). The nomadic Bedouin tribe constituted the majority of the Saudi Arabian society nearly 70 years ago. According to Al-Dabal (1999), the Arabian culture, which is largely influenced by the Islam religion, can be compared to that in the United States using the Hofstede’s cultural matrix. According to Hofstede (1980), Collectivism “is characterized by a tight social framework in which people distinguish between in-groups and out-groups, they expect their in-group to look after them, and in exchange for that they feel owe absolute loyalty to it” (p.45). Moreover, individualism refers to “a loosely knit social framework in which people are supposed to take care of themselves and of their immediate families only” (Hofstede, 1980, p.45).When collectivism and individualism are compared between the two countries, the level of individualism is higher in the US than in the Arab nations. Collectivism is considered the second major factor after Islam that has influenced the culture in Saudi Arabia (Al-Dabal, 1999).
Healthcare in Saudi Arabia also has been influenced by cultural factors such as consanguineous marriages; that can be defined as marriage between persons, who have the same family name (Fisher, 1996). People in Saudi Arabia prefer consanguineous marriages for many reasons that include strengthening of family ties and avoiding the dispersal of property and other assets to those outside the family (Bittles, 2001). According to Al-Abdulkareem and Ballal (1998), such consanguineous marriages are ascertained to be one of the major causes for the occurrence of certain inherited blood disorders among this population. In order to reduce the rate of such disorders, in 2003 the Saudi government, also introduced pre-marital testing for couples entering into matrimony. However, in a study carried out by Alsulaiman and Hewison (2006) on the general attitude of the people, to prenatal and pre-implantation testing revealed that nearly 50% of the couples that are at a genetic risk would not resort to such testing. This is suggestive of the fact that such testing procedures are still considered unacceptable among the population as they are against their cultural and value systems.
The present healthcare delivery and quality management system was non-existent in KSA until 1926 as they were provided only by individuals rather than the government (Middle East institute, 2009). However, since then the quality of healthcare and its delivery has become more organised and effective to reach its present day standards. With the immense development in the field of total quality management (TQM), many workers have taken up jobs in both the public and private healthcare sectors and have contributed to improved quality management.
Dale (1994) has argued that, the shifting of TQM from the manufacturing industry to the health sector has its share of difficulties for various reasons. For instance, the difference in the managerial environment compared to other sectors because of healthcare consumers differ from others as they use the service as patients. The above reason makes it harder for implementing the accreditation standards in TQM as well as consistently improving the quality of healthcare a challenging mission. Additionally, Dale (1994) has clarified that, there are many challenges faced by the healthcare staffs including those in the management department as well as physicians who strive to deliver optimum service to their patients in the most appropriate way possible.
According to Dale (1994), despite these efforts, several hospitals have not been able to maintain or improve their quality. Considering the many hospital deaths that could have avoided, and in many cases, people have died owing to improper medical treatment afforded to them.
It is vital for healthcare organisations to determine their inefficiencies in quality and cost containment. This would enable the quality of care and its cost to become more transparent. With the exposure of these problems, the stakeholder organizations could release more information about the standard of these hospitals. With the increasing availability of the Internet, the public can obtain data about the hospitals and then make a decision about their choice of care. There are many challenges to be conquered with regard to resource allocation, the service cost and efficiency and effective delivery of healthcare to the people (Kanji and Moura, 2003). In order to achieve all these objectives, the adoption of accreditation standards for delivering quality healthcare by improving performance and ensuring that all patients have equal access to care has been proposed.
This paper explains the JCI accreditation standards as the best health care method/program after compares and contrast with Six-Sigma method, which has been adopted to carry out the study. The second portion of this paper examines the existing literature on accreditation of hospitals, starting with the healthcare system in KSA prior to implementing the JCI concept. It also identifies the factors that prevent the implementation of quality in healthcare organizations from a different perspective.
Healthcare System and Ministry Of Health (MOH) in the KSA
Kingdom Of Saudi Arabia with its numerous humanitarian achievements nationally and internationally has been awarded its status as the “Kingdom of Humanity”, as decreed by The Custodian of the Two Holy Mosques. This has considered the national logo used by the government in relation to any humanitarian endeavour (Conjoined Twins, 2011).
The Kingdom of Humanity reaches out across geographical and cultural barriers to aid those in need regardless of race, colour or beliefs. These principles prevail under the leadership of The Custodian of the Two Holy Mosques, King Abdullah bin Abdul-Aziz Al Saud whose acts of benevolence clearly show his compassionate and generous nature (Ministry Of Health, 2010). This is evident by his sponsorship of numerous conjoined twins’ separation cases from all over the world. During the past fifteen years, 13 sets of conjoined twins have been successfully separated in the Kingdom of Humanity under the sponsorship of King Abdullah bin Abdul-Aziz Al Saud and the experienced Multidisciplinary team (Ministry Of Health, 2010).
The TQM program of the health department in KSA initially started in the Markkah region, which is under Prince Abdul Majeed. Latterly, it spread throughout Saudi Arabia that has recognised by the Central Board for Health care Institutions (CBAHI) (Hoskins, Abdul-alHamid, and Ghasib, 1994). The Ministry of Health (MOH) is the department responsible for the supervision of both public and private healthcare institutes. MOH came up with a five year plan to bring about changes in different areas such as healthcare in 1970.. Under the healthcare sector, the plan outlined the necessity to implement accreditations to develop healthcare organisations, improve facilities in clinics, pharmacies, laboratories services, primary care, and research centres (Jovanovic, 2005). It further included the hiring of expatriate staff to work in healthcare facilities and encourage the public to pursue a career in this field. The Ministry offers a universal healthcare coverage for all classes of people. There are different cases of healthcare delivery. Some of them have comprise a network of primary healthcare centres and clinics that provide preventive, prenatal and emergency mobile clinics and other basic services for the rural population, while the other cases have been coverage by hospitals and other specialised treatment centres that are primarily located in urban regions(Central Board for Accreditation of Healthcare Institutions, 2010).
Table 2 1: Health Resources Indicators (2009). Source: Ministry of Health Statistical Yearbook (2009).
Since the 1970s, the number of beds in the Saudi hospitals has risen dramatically to 220,400 beds, in 2009. Of these 173,800 beds are in government hospitals and 46,600 beds in private hospitals (Ministry of Health Statistical Yearbook, 2009). 62% of hospitals and 52 % of clinics fall under the ministry of health while the rest are run by governmental agencies us the defence ministry including the private sector. (See table 2.1).
MOH Mission and Vision
The Ministry of Health (2011) mission is to has as its mission the provision of comprehensive and integrated therapeutic, rehabilitative and supportive health care in accordance with the principles of Islam as well the ethics of healthcare delivery. MOH tries to fulfil its mission by catering to the need of the patients, their families and the community as a whole and by upgrading awareness about health and by implementing the right laws to provide better healthcare in both quality and quantity throughout the country (Ministry Of Health, 2011). In addition to taking care of the status of the employees, MOH also provides training; rehabilitation adequately rewards them in order to ensure best healthcare delivery. The vision of the MOH is to achieve the realisation that health is a comprehensive concept that needs to be dealt at the level of the individual, family as well as the community in order to maintain the quality and quantity of healthcare services and to help the elderly and others with special needs. The vision of the Ministry of Health is to realise health in its comprehensive concept at all individual, family and community levels. Maintaining health in both quantity and quality, also help the elderly and those of special needs by enabling them to accommodate with their health situations in health care providers at both private and public sectors (Ministry Of Health, 2011).
MOH Vision for 2020
According to Ministry Of Health (2011), the MOH vision for the 2010 aims to provide best and quality healthcare for the people of KSA with equal and satisfactory medical care afforded to all classes of people in order to help them manage the financial burden. It is also working to create a basic structure for formulating health policies, including health insurance services. Another mission of the MOH is to adopt a general national health strategy with focus on diseases including infectious diseases and also nutrition, effects of smoking, AIDS and other accidents and injuries. In addition, the MOH is also keen to develop an adequate and fair method for assessing the risks and advantages of the services provided (Ministry Of Health, 2011).
Healthcare Accreditations and Standard
Accreditation refers to a systematic assessment process that hospitals use to access their standards against the standards set by a particular authority. Accreditation was used only in hospitals at first but other sectors in the healthcare services adopted it for example laboratory services. The practice of accreditation has its genesis in the United States. It began in 1917, with the American College of Surgeons. The institute came up with standards to be used in defining hospitals that were appropriate for offering surgical training to medical students. Later, the standard programs evolved and into a multidisciplinary program and become the standardization platform. The program led to the establishment of the Joint Commission on Hospital accreditation in 1951. The commission changed its name and became the Joint Commission on Accreditation of Healthcare Organisations (JCAHO). Many other national programmes developed from JCAHO either directly or indirectly. Since, 1990 the number of programs has seen a twofold growth across the globe within every five years (Jovanoviæ, 2005). Europe has the most remarkable growth rate of programs in the world with eleven robust programmes. The programmes are scattered across Spain, France, Netherlands, Germany, Switzerland, Poland, Bulgaria, United Kingdom and Portugal. The United Kingdom and Switzerland have three and two programmes each respectively. In order to know the number of accreditation programmes in the world, World Health organization did a survey and identified 36 programmes (World Health Organisation, 2004).
The international community demands international standards for evaluation of healthcare facilities thus JCI accreditations are used because they have agreed upon by health professionals drawn from various countries in the world (Joint Commission International, 2003). Bodies that offer accreditations are independent, their main objective is to ensure that quality, and safety is upheld in services delivered to patients. The bodies also work to ensure that safety and quality is improved by healthcare organizations by following set standards, which they are required to observe in order to attain accreditations after an assessment by external peers (Jovanovic, 2005).
Healthcare organizations are able to meet the set standards by improving quality and safety. The organizations are encouraged to maintain a safe environment for both their patients and staff that minimizes ad eliminates risks for the staff and patients. The accreditation process is recognized worldwide as a valid tool for measurement of quality safety and management in hospitals and any other health facilities. The accreditation regulations set by the accreditation body are aimed at creating safe environments by encouraging a culture in healthcare settings. Moreover, healthcare organizations get motivation form the standards to maintain a safe culture through provision of quality care at all times for the sake of the patients (Joint Commission International, 2009a). Healthcare organizations that attain accreditation are required to prevent occurrences of medical error by taking specific steps the steps taken to avoid communication breakdown between caregivers and the staff, errors in identifying patients correctly and equipment problems (Joint Commission International, 2009b).
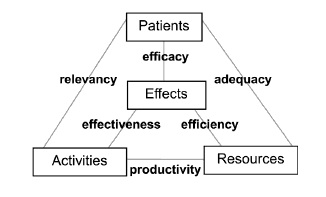
Quality management understanding involves the following components: effects, activities, resources and patients. The four components are categorized into detailed items: unfavourable health effects, financial, other resources and human among others. This research will only look at the initial four components of quality management for educational purposes. However is vital to differentiate between indicators that connect two entities at least and descriptors combining date that are issued from one entry only. (Boutat et al., 1992).. The combinations formed from the entities. These combinations rationally make six families of indicators together with four (Figure 2 1).
Flexibility of healthcare accreditation standards
For a healthcare organization to improve its quality management system it can implement various strategies although the aim of stating this is not to elevate one strategy over the others but to make it known that different strategies can be employed in healthcare quality management. It is also important to note that over relying on strategy can produce negative results and discourage healthcare workers from implementation of its recommendations. There is a high likelihood that cultural aspects determine choices made in the strategy to use but the drawbacks of each should be taken into consideration. The following examples illustrate the above point. The ISO 9001 model does not pay attention to aspects such as staff motivation or resource management although it is unwise to do so but the model can give excellent outcomes in some sectors in the healthcare processes. Moreover, a health facility that follows bureaucratic red tape may give an assurance to the staff for the respect of care standards and may motivate them highly. On the contrary, the high motivation of staff is not a guarantee that the patients views are taken into account or that the care they give would earn approval from health professionals practicing in other hospitals even if the healthcare organization is has been awarded accreditation. Eventually, illusions may be created in the total quality concept through the neglect of resource management that limitations do not exist (Bechel et al., 2000). Moreover, it is difficult to sell the idea to an institution from a few carriers of the idea as medical practitioners may take it just as a fad (Stern, 1997; Grol, 2000).
The above examples illustrate the dangers that can result from a unilateral approach. Evidence about the impact that each approach has is lacking (Grol, 2001). All the factors that lead to quality provision ought to be taken into consideration. Furthermore, it is paramount to consider the previous stages during the examination of a particular factor. For example, an external audit in a hospital would be of no value but a wasteful expense if there lacks documentation of the real situation or measure and the expectations or standards. Objectives must be defined before or a staff appreciation interview would only end up being a superficial task. More importantly, the guiding clinical principles must be created in accordance with the classification method utilized in the hospital’s information system to enable the observation of practice outlines. Lastly, it is recommended that managers in healthcare organizations come up with quality management process that fit their setting according to the planned structure to enable them sensitive to likely shortcomings.
A conceptual frameworks used in hospitals quality management
The proposed concepts of the total quality management proposed concepts of healthcare organizations could be as different acknowledged approaches. The four approaches decided by this research paper are:
- ISO 9001 standards (International Organization for Standardization, 2000);
- JCIASH (Joint Commission International Accreditation Standards for Hospitals, Joint Commission International, 2000);
- EFQM excellence model (EFQM, 1999);and
- Total quality management (TQM) doctrine (EGGLI & Halfon, 2003, p. 30)
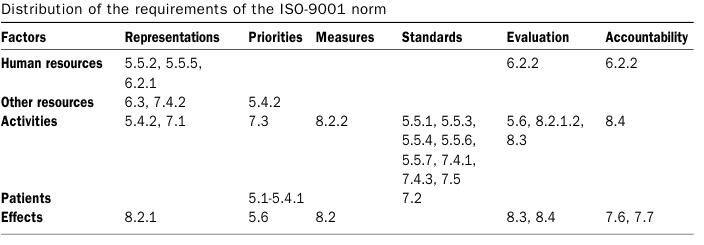
ISO 9001 has awarded over 230,000 certificates to organizations in over 130 countries across the globe. The ISO standards are mostly applied in laboratories and radiology. However, their implementation in clinical setting has not been successful. The majority of requirements in ISO standards focus on management activities that are correction and prevention of errors, document control, quality standards, product traceability and effects. The effects focus on customer satisfaction. The ISO framework main goal is the clients and aims to put them at ease by assuring them of receiving quality medical care. On the contrary, clients are not well versed in matters quality when it comes to picking healthcare providers and hence the ISO 9001 is not effective in a hospital context (Eggli & Halfon, 2003). Even in the U.S where their healthcare system is consumer driven a client survey puts information regarding quality in picking out health care service provider down in their list (Bailit, 1997). It is not s surprise that promotion of ISO 9001 model in hospital settings has been minimal.
The Joint Commission of Accreditation of Health Care Organizations (JCAHCO) has come up with specific sets of international standards that hospitals are required to follow and evaluated by Healthcare experts Heidemann, 1999). The requirements of the framework are on staff management. Staff management entails hiring, job description and crediting the staff for competence. Moreover, the requirements focus on “admission, discharge, transfer, and delivery of high risk services” (Eggli & Halfon, 2003, p. 31).
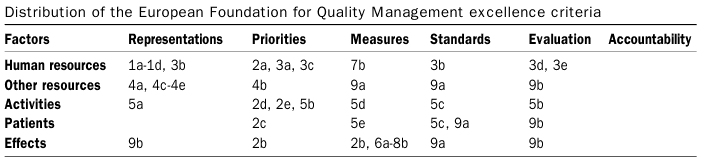
The European Foundation for Quality Management excellence model (EFQM) is popular and over 800 organizations across Europe have used the framework. EFQM has a subdivision called International EFQM Health Sector Group that shares experiences similar to EFQM. Table AIV (Appendix 1). The framework takes care of most aspects of quality management but does little on accountability because it is mainly focused on excellence. It also aims promote self-assessment.
Table 2 2
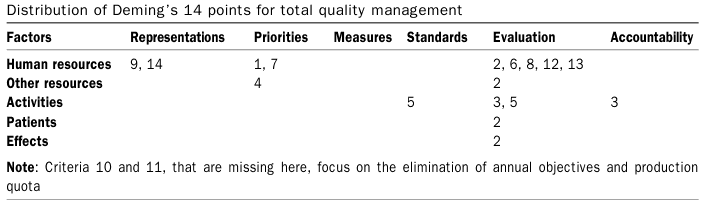
The total quality doctrine” (TQM) framework focuses on the client. It can be summarized using the slogan everything should be done to attract, satisfy and retain the trust of the client” (Eggli & Halfon, 2003, p. 31). In order to satisfy the clients and retain them the staff must be motivated. If the staff is motivated it can deliver better services to clients who will in turn be satisfied with eth services. Conversely, TQM does not stress upon all quality aspects, as accountability and management are not fundamental in quality assurance according to Deming (1986).
International Medical Centre has agreement with JCI
The International Medical Centre (IMC) entered into an agreement with the eminent authority body on healthcare JCI in 2000. IMC associated with JCI to acquire accreditation because JCI offers accreditation to healthcare organizations that illustrate exemplary standards in medical care. In order to understand why IMC chose JCI it is important to look at other standards that hospitals use. European Foundation for Quality Management, 1999 (EFQM) is another standard. The model has nine components. The other standard of ISO 9001 entail the following components -human, clients/patients, processes, products, measurement, analysis, management and ongoing improvement. The EFQM is the only model that has the concepts of policy and strategy and leadership. Both the ISO 9001 and EFQM do not provide a systematic quality management matrix. The ISO standard lacks a measurement system for comparing achievements in various levels while the EFQM model is very complex with its scoring tool called Results, Approach Deployment Assessment Review (RADAR). Moreover, the assessment criteria used for its results and processes components is not similar. The RADAR scoring tool has 138 items hence too much and hospital workers object its use due to time constraint (Eggli & Halfon, 2003).
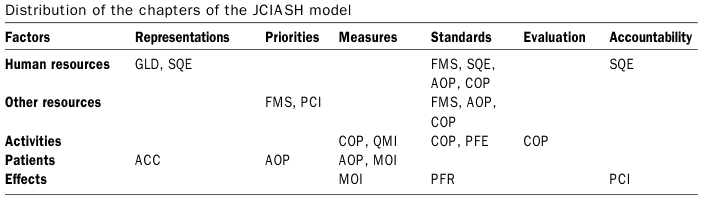
The other standard is the Joint Commission International Accreditation Standards for Hospitals (JCIASH), Joint Commission International, 2000. The commission has specific sets of international standards that hospitals are required to follow and evaluated by Healthcare experts. The requirements of the framework are on staff management. Staff management entails hiring, job description and crediting the staff for competence. Moreover, the requirements focus on “admission, discharge, transfer, and delivery of high risk services” (Eggli & Halfon, 2003, p. 31). The framework also pays particular attention to effects in terms of patient respect and adverse events. However, the framework is not well developed in financial and marketing aspects. It also lacks a good basis for evaluation of requirements EFQM is popular and over 800 organizations across Europe have used the framework. The framework takes care of most aspects of quality management but does little on accountability because it is mainly focused on excellence. It also aims promote self-assessment. The last one is total quality management (TQM) framework focuses on the client. In order to satisfy the clients and retain them the staff must be motivated. If the staff is motivated it can deliver better services to clients who will in turn be satisfied with eth services. Conversely, TQM does not stress upon all quality aspects as accountability and management are not fundamental in quality assurance.
All of the above standards contain shortcomings that the JCI standard helps to overcome thus IMC choose to it over the others. JCI aims help healthcare facilities become safe environments that provide quality care. The commission does so by providing education and consultations services to hospitals. IMC collaborated with JCI because its objectives are to provide exemplary services to the patients and the JCI standards will help the medical facility attain its objectives because it standards quality care and patient safety. Moreover, JCI standards that take cultural aspects into consideration is the best model for IMC to use so that it can uphold its Islamic standards and at the same time cater for all people regardless of their race, gender, disability or religion as outlined in their patient’s rights and responsibility guidelines. Thus, patients will feel respected when their cultural practices are out into consideration as they seek medical care. The JCI standards are world renowned and IMC getting JCI accreditation puts its raises its reputations as patients will feel confident seeking medical care from a facility that meets international standards in healthcare because the standards that JCI uses are created by international health experts from all over the world. Patients will feel secure with the services provided at IMC because the body requires hospital to engage in risk management hence reduce medical errors and risks. Following the JCI standards makes IMC a healthcare facility of international standards yet it able to cater for the local community in KSA. IMC will benefit from the education and consultations services offered by JCI and will be in a better position to address the challenges they encounter in their medical processes.
International Medical Centre (IMC) in KSA
The IMC is a multi specialty hospital with 300 beds, which is committed to deliver quality healthcare to the people. The centre attracts its customers through its new approach towards diagnosis and treatment and by providing the desired Islamic cultural atmosphere, which has expected to grow steadily from one generation to the next. In order to ascertain their commitment to accurate treatment, IMC is working in collaboration with the highly acclaimed JCI to establish an international standard of treatment. This multi specialty hospital encompasses six Centres of Excellence that includes sub specialties in which Board Certified Physicians of US and Canadian work together to deliver excellent medical care to their patients. The healthcare organization has various centres catering for different people and needs such as women’s health, plastic surgery, and diabetes among others. Both the construction and facilities offered at IMC were carried out under the guidance of JCI which collaborated right from the conception, design and setting up of the medical facilities of the centre. The IMC logo is represented by a tree, which is composed of five crescents that together symbolise the body, mind and soul (See figure 2.1). This symbolises the mission of the IMC, which is to achieve optimum health and the lower crescents beginning from the trunk and roots symbolise the international standards and ethics, which are vital elements for the success of any healthcare centre (International Medical Centre, 2011).

The centre has also entered into an affiliation with the Cleveland Clinic Foundation (CCF), which is the first American Institute that has entered into a partnership with the centre. The CCF owns stock, as an equity holder and with the partnership; it has agreed to work with the centre in several joint ventures such as promoting e-health, teleconferencing and continuous education programs. The JCI has reviewed the architectural plans of the IMC and has confirmed its compliance with the US construction standards for healthcare facilities. In order to aid in the design and operational planning processes and to ensure the required level of care and quality that is comparable with the US standards, the IMC entered into a multi stage contract with the JCI, which has finally led to international accreditation. The heads of the IMC medical team in Boston have also negotiated partnerships with other leading medical institutes, within the US for a long-term strategic alliance with the centre (International Medical Centre, 2000a).
According to Joint Commission International (2009b), IMC is going to follow JCI process of obtaining accreditation or certification, the IMC has implemented all the above 14 standards and the TQM department is involved in all the accreditation standards. This department is responsible for ensuring that all the standards are implemented in healthcare settings through regular inspection of all the concerned areas. Such an inspection is carried out twice a year with the entire hospital being covered during each session. The inspection by the TQM department includes members from their team, while the environmental rounds include a representative from every separate department such as hospitality, safety and laboratory. Each department representative inspects his or her specific area of expertise. Their findings sent to the TQM department who then forward the findings to the head of the inspection for necessary action to be taken based on the findings (See Figure 2.3).
Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
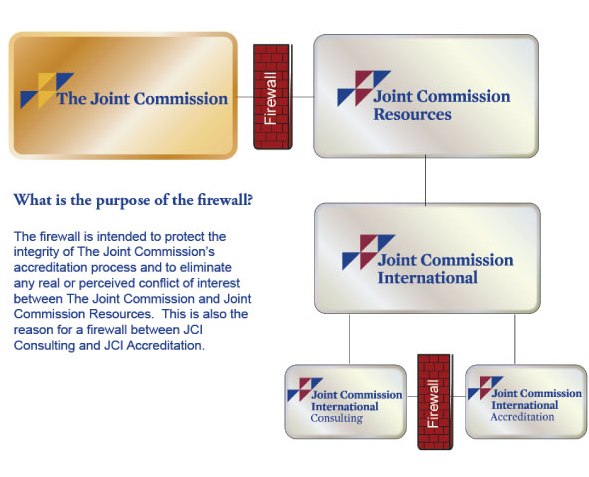
The Joint Commission on Accreditation of Healthcare Organization (JCAHO) has set specific standards for such organisations and issues accreditation certification for those, which meet the set standards (Joint Commission, 2010b). The JCAHO, which is an independent non-profit organisation, has accredited and certified more than 18,000 healthcare organisations in the US. Accreditation is a measure of quality in healthcare organizations and it is recognized worldwide and shows that an organization is committed to providing and observing the high standards in accordance to set standards. At present, all the accredited healthcare organisation are following the Joint Commission standards as a guidance to ensure proper care is provided to the patients and also to continuously improve their performance. Hence, the JCAHO is the only capable accrediting organisation as it has the capacity and experience to properly evaluate healthcare organisations across the world (Joint Commission, 2010a). As can be seen in figure 2, JCI has been defined as division of JCR Inc. that considered being part of The Joint Commission.
The Joint Commission International (JCI)
JCI has been working with several healthcare organisations, health ministries and other global organisations in more than 80 countries since 1997(Joint Commission, 2010b). The primary focus of the JCI is patient care, safety, and duly providing accreditation certification advisory and educational programs that would aid in implementing suitable solutions in these organisations. In the year 2000, the IMC at KSA entered into an agreement with the JCI thus becoming the first hospital in the region to collaborate with the JCI right from the inception of the project (Joint Commission, 2010b).
The JCI, which is a globally recognised authority for accreditation of healthcare organisations, accredits only those concerns that demonstrate a high standard of medical facilities and patient care. Hence, throughout the initial stages of formation of the IMC, the supervision and guidance of the JCI was sought to oversee the design and construction and other medical facilities and procedures offered by the organisation (International Medical Centre, 2000b). The JCI mission is to improve the quality and safety of healthcare being afforded by the medical community worldwide and the Commissions has been performing this dedicates service for the healthcare industry for more than 75 years. The JCI grants the accreditation based on the initiatives taken by the healthcare organisation, which are designed in a manner that would meet the growing demands in the field of medicine. The main purpose behind this is to provide a standard and objective based process for evaluating the international healthcare community (Joint Commission, 2010b). In addition, it also ensures that healthcare organisations demonstrate a continuous and sustained development by implementing the agreement standards, patient safety goals and indicator measurement support within their healthcare program. Thus based on the above motives the JCI has developed standards and accreditation programs for: Clinical Laboratories, The Care Continuum (home care, assisted living, long-term care, and hospital care), Medical Transport Organisations, and Ambulatory Care. In addition, it also certifies programs that provide Disease or Condition Specific Care such as those designed for stroke or cardiac care. Hence the JCI accreditation, though based on an international framework of standards, they also encompass the local needs of the patient population (Joint Commission International, 2009a).
Benefits of JCI accreditation and certification
The Joint Commission (2010b) has clarified benefits of JCI accreditation; one of the major benefits is the provision of education on good practices in the field of medicine as well as, to improve risk management that would result in a reduction in risks and errors. In addition, to strengthen the trust of the community on the quality and safety of care and services offered also, conducting on site evaluations by trained clinicians and advocates to assess patient safety. Moreover, to develop internationally recognised standards by healthcare experts from across the world, the provision of accreditation and certification is decided by an international committee of health care experts (Joint Commission, 2010a). Finally, guidance on patient care, an advisory council that is comprised of health care leaders from Europe, Middle East, and Asia Pacific provides safety and quality issues (Joint Commission, 2010b).
Improvements and effectiveness
The focus of the JCI is to improve the “safety of patient care through the provision of accreditation and certification services as well as through advisory and educational services aimed at helping organisations implement practical and sustainable solutions” (Joint Commission International, 2008). The standards of the JCI have been decided by international healthcare experts in order to achieve consistent and better expectations from healthcare organisations. According to National Guard Health Affairs (NGHA) (2010), through accreditation by the JCI, NGHA in KSA now has immediate access to a wide variety of resources ranging from the international system for measuring the quality of services to patients across the board. In addition, it has also set a benchmark for the guidelines under quality management in patient healthcare, patient risk reducing strategies, improved healthcare practices and quality control measures have to be undertaken in order to completely realise the services of the NGHA. By this certification, the NGHA has ensured that all its facilities meet the needs of the patients through increased safety measures and infection control, better medical and pharmaceutical facilities in compliance with the accreditation standards (National Guard Health Affairs, 2010).
The JCI has introduced many basic principles that provide guidance for healthcare organisations. Though many of these are routine and common principles now, they were new and revolutionary first when they were introduced.
Pasternak (2009) clarified that the following are some of the fundamental principles introduced by the Joint Commission, Medical Records; the necessity for medical records arose in year 1917 when they were viewed as unwanted by many. However, in today’s scenario the medical record is the most vital source used for storing information about the patient, their health problems and the treatment decisions, research, patient monitoring, the outcome of the treatment and even the patient bills. Moreover, according to Pasternak (2009), patient safety; this principle serves to identify medical errors, their causes and aids in developing safety measures in healthcare organisations. This intervention by the JCI in affording patient safety has indeed reduced the frequency of medical errors and other sentinel events.
Evaluation
The evaluation process includes a range of functions and systems that include preventing patient care hand over errors, wrong site or procedure surgical errors, preventing the continuation of medication based errors, high concentration drug errors and the promotion affective hand hygiene practices (Saad, 2011).
Limitations and Weakness
The JCI is a private entity that has designed a “mechanism to assure that accredited health care facilities meet certain basic standards” (Shi & Singh, 2008, p. 320), and on that basis, they determine whether the facility is eligible to receive Medicare/Medicaid reimbursement (Shi & Singh, 2008). The non-governmental status of the JCI that conducts the regulatory work has been challenged in the court by many healthcare organisations. As an example, in 1984, persons under the age of 21 can be offered Medicaid financed care if psychiatric hospitals have JCI accreditation standards. Other critics have pointed out that “through the use of the JC, the government has endorsed too narrow and monolithic a vision of health care” (Jost, 1994, p. 43).
In addition, another concern is that the JCI Inc. website has listed the available consulting services without clarifying the prices and its seminars that cost $650 per person, which has included references that could be used to prepare performance evaluation questionnaires of healthcare organisations (Joint Commission International, 2008). Despite these fears, a conflict still exists more so when an organisation’s access to obtain Medicare reimbursement is based on these factors. The final concern is the actual cost factor involved in the accreditation process. In the year 2008, the average cost for an accreditation questionnaire was $41000, this is in addition to the expenses required to prepare a facility for a survey, which could vary with respect to its size, location and the scope covered by the organisation (Joint Commission International, 2008). In accordance with the hospital size, the survey team will also vary in number, which will in turn affect the survey cost. Hence, this cost factor associated with the survey process places an additional burden on the institute and makes the accreditation process even more complicated (JTaylorBUProject, 2009).
Criticisms
The JCI has faced criticisms about its functioning in the past from the US, which has notified hospitals of these inspections that must strictly adhere to this. An article published in The Washington Post (2005) has stated that nearly 99% of the hospitals that were inspected were granted accreditation. However, during the process, serious problems with delivery and care are often being overlooked or neglected. Similar statements have been issued in other paper such as The Boston Globe(2007), which has stated that “The Joint Commission, whose governing board has long been dominated by representatives of the industries it inspects, has been the target of criticism about the validity of its evaluations”. The JCI has responded to these statements and criticisms and since January 2006, all the hospital surveys conducted in the US were carried out without any prior announcements by which the institutes would not have time to prepare ahead of the evaluation process this eliminating the possibility of inadequate standards being maintained in between the surveys. However, surveys done at international institutes by the JCI are still being done with prior notice and as a result, there is considerable preparation time given to the hospitals. Other means can be used to make the evaluations such as the Total Quality Management Doctrine. It deals with the business aspects of organizations and can be done through regular appraisals. The other method that can be used is the ISO standards in which healthcare organizations are awarded certificates for compliance with the set regulations. The other methods used to maintain standards at healthcare organizations have their own limitations that make JCI method the most suitable to use. JCI is specifically formulated to be applied in healthcare setting and hence caters for all aspects that regard quality of care and hence gives the staff and patients the best alternative to ensure proper environment and quality services (Harry &Schroedter, 2000). Lastly, JCI can make impromptu visits to the hospitals to ensure that the hospital complies with the regulations at all times and not only in readiness for inspection.
Conclusion
In conclusion, the JCI has specific healthcare accreditations and standards, which are required to be followed by all hospitals they enter into an agreement with. After much effort, and thorough analysis of limitations, weaknesses, and criticisms, it has been proved that IMC in Saudi Arabia has the required qualifications and standards. Therefore, it was the first hospital in the region to collaborate with the JCI.
Methodology
Introduction
Problems are bound to exist at academic institutions, workplace or any other situation in life. These could arise because of minor incidences or complex, integrated problems which affect the normal course of life. Hence, it has become necessary for academicians and managers within an organisation to attempt to understand the underlying problem and find suitable possible solutions to alleviate the problem using various investigative methods. Such an investigative approach to solve problems is referred to as research.
Many writers and other experts have defined the concept of research in several different ways and from a wide range of viewpoints. One such definition views research as an “organised, systematic, data based, critical, objective, scientific inquiry or investigation into a specific problem, undertaken with the purpose of finding answers or solutions to it” (Sekaran, 2003). Scientific enquiry or research involves a series of steps that begins with defining the problems through proper investigations using a scientific approach and devise methods to reach a suitable solution.
Experts have divided this process of scientific research under eight sub-divisions. The first characteristic is purpose, which implies that every researcher should have a specific purpose for undertaking the research. This is the initial step that would enable the researcher to find suitable answers and methods to solve the problem. The next important requirement is rigor by which researchers need to be attentive and scrupulous during the research process in order to avoid any errors or bias that may affect the end of results. The next requirement is testability by which a hypothesis should be subjected to proper testing processes after collection of the required data. Following the testing process the researcher should also ensure that the results obtained are replicable every time the research is conducted under similar conditions as this will ensure that the hypothesis is reproducible. The next requirement for any research is precision and confidence. Precision ensures that the results obtained from the research are relevant to the hypothesis made and the confidence levels reveal the extent to which the results are correct. In addition to the above factors, every researcher should be objective in their research by which any subjective or emotional bias should be eliminated and the study interpretation should be based on the data alone. Another important requirement is generalisation of the study by which the study could be applied to any setting. Finally, the study should also be simple to perform and understand rather than complex (Sekaran, 2003).
The following chapter begins with the definition of the research problem and then describes the purpose of this study, following which the study objectives are detailed and in turn, the study setting has described. The research methodology that includes the sampling methods is explained and the types of data to be used, data collection and analysis are then explored. The contribution of the study is described finally. The method employed in the study is telephonic interview and use of an electronic survey of executive staff with the IMC staff members. The IMC has entered into an agreement with the JCI, which has made it the first hospital in Gulf to be involved with the acclaimed organization right from the inception of a project.
Research problem
Following the implementation of the JCI standards within the TQM department, several manufacturing industries have shown marked improvement in quality in different sectors across the country. Given this increase in quality improvement, the service industry, especially the healthcare industry has shown interest in implementing this concept within its purview.
The Saudi health sector, both public and private, faces a variety of general challenges such as resource allocation and other challenges related to its nature such as the quality of services provided, cost containment and medical errors.
Considering the increased benefits that could be gained by implementing the TQM, several healthcare policy makers in Saudi Arabia have shown a willingness to adopt this approach within their healthcare system in order to improve the performance, quality and services of their organization and to improve health indicators. Despite the various benefits, the introduction of the JCI standards within the TQM is relatively a newer concept within Saudi Arabia, which could face some stiff challenges owing to factors that could have a negative impact on its implementation. Hence, the major question that remains to have addressed is the extent to which the JCI accreditation standards will improve the healthcare facilities?
Study purpose
The study purpose has aimed at answering the above question by exploring the implementation of the JCI standards by hospital in KSA. The Jeddah city was chosen for the study, it is located in the western part of Saudi Arabia.
Study objectives
The study objectives included assimilation of evidences observed in Saudi hospitals pertaining to healthcare management in order to aid these institutes to implement a better healthcare service strategy for its customers. Additionally, the study also focused on emphasizing the importance of quality change within an organisation as it is not merely associated with implementing a set of standards, rather it could be deemed as a cultural change and all the factors that could affect this change will have to be considered.
Qualitative and quantitative methodologies
The use of qualitative or quantitative method for a particular study entirely depends on the research question and its purpose. In case of some studies, both the techniques will have to be employed in order to attain the goal of that research (Ulin et al, 2005).
In case of the quantitative research technique, all the parameters covered under the research have converted to numbers, followed by quantifying the problem and then analysing and discussing the results obtained on a numerical basis (McQueen and Knussen, 2002).
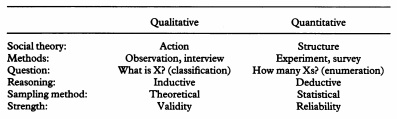
Berg (2007), in his article has stated that qualitative research is “the meanings, concepts, definitions, characteristics, metaphors, symbols and descriptions of things”. This research technique focuses on the quality of the data garnered from the study or in other words, the qualitative method is “attempting to explore and describe, explain and predict” (McQueen and Knussen, 2002). The technique relies on complete understanding of the research problem. As an example the method of data collection in a particular study, need to be done through interviews or observations. This method is being appropriately used for healthcare research. The doctors and other healthcare professionals are required to incorporate research reviews, patient observations, detailed telephonic interviews and electronic survey of executive staff. Qualitative research focuses on the development of research methodologies, which would facilitate the understanding TQM functionality that deals with emphasizing the meanings, experience and views of all the participants of the study. This would enable researchers to understand the reasons behind healthcare related issues such as why education against the practice of smoking among teenagers and young adults is not effectively followed in their day-to-day life. As can be seen in Table 3.1, these qualitative research studies are more concerned in dealing with queries such as ‘What is TQM and how does JCI standards practices vary under different circumstances, and why?” rather than “How many JCI standards are there?” (Mays and Pope, 1995).
In the implementation of the JCI standards, a qualitative method of research was chosen in order to identify the various factors that influence the implementation process. Hence, as the goal of the study was to identify the factors rather than measuring their frequency of occurrence or distribution, this method was preferred to the quantitative technique (Hudelson et al, 2008). This method can be employed to obtain information about various complex settings such as the interaction of patients with their clinicians and those present among different professional groups within the organization. The results obtained from such studies aid in identifying the value of people playing a specific role within the organization. The method allows the people to speak for themselves and do not impose terms or place them under specific categories during the research process. Through such a process, the people are encouraged to describe the events that they have encountered in their own way by which the researcher gains an understanding as to how the events are interpreted differently by various individuals (Sofaer, 1999). Hence, such qualitative processes are useful in the evaluation of healthcare services and to identify the factors that are associated with the delivery of these services to the patient community (Spencer et al., 2003).
The qualitative method is used in this research, which analyses the implementation of JCI standards within the TQM of hospital in Saudi Arabia. This method was also chosen owing to the insufficient information available in the implementation of the JCI standards in the healthcare sectors.
Collect data
The result of any scientific research depends on the data collected, which is generally classified into two different types’ namely primary and secondary data.
Primary data
Mcnabb (2008) as the initial or new information that is collected describes primary data. For example, this might include surveys that are conducted using an electronic survey, telephonic interviews of the concerned individuals, using content analysis or published documents or carrying out an experiment. From the primary data collected, the information is processed and interpreted, which is used to draw suitable conclusions on the study and to make relevant recommendations if required. In the present study, data from telephonic interviews and electronic surveys of executive staff was collected, analyzed and recorded as documents as excel sheets.
Crowther and Lancaster (2008) have analyzed the advantages of using the observational approach for collecting primary data, more particularly in the area of management and organisational research. These observational analyses, unlike those of interviews and surveys, these are based on first hand observation of the individuals (Bryman, 1989; Delbridge and Kirkpatrick, 1994). Another advantage of this technique is that the process can often yield new data and research findings, which are impossible to obtain by any other method. In other words, observational research can be useful in identifying smaller or hidden issues within an organization, as it is easier to shift one’s observation to even a small distracting behaviour, which is interesting (Graziano and Raulin, 2004). This form of research techniques allows for greater generation of detailed information compared to collecting primary or secondary data using surveys and telephonic interviews (Robson, 2002). Finally, observational research is particularly well suited to carry out research within one’s own organization as in the case of a consultancy type student research project (Saunders et al, 2009). Despite these many advantages, the technique also faces some disadvantages and limitations with regard to primary data collection, as the time taken is long as is the cost required for the collection process. Additionally it is also difficult to get the doctors and other heads of the department, the managers and directors in the TQM department to offer their cooperation for answering the surveys or even telephonic interviews and is difficult to organise the right time between London time and KSA local time. In addition, the researcher should be careful in choosing the right tools and methods for the analysis. In these processes, the researcher is bound to have a lesser degree of control over the data collection method. As the research is entirely dependent on the willingness of the respondents, there is a greater chance for the quality or scope of the information to be weaker in such processes. There could be several reason associated with an individual’s refusal or unwillingness to cooperate in the research such as lack of time or suitable rewards for their participation (Ghauri and Gronhaug, 2005).
In the present research, however, telephonic interviews and executive staff surveys were used as a primary data source.
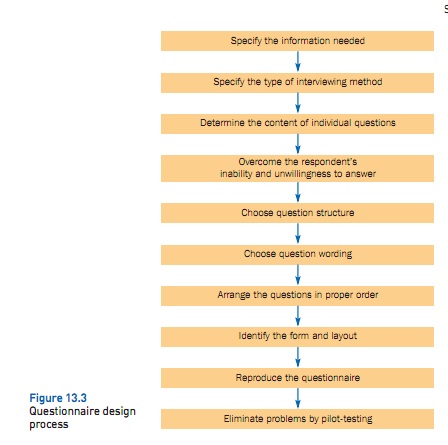
In order to completely understand the survey design, the process will be presented as a series of stages as shown in Figure 3.1
The first step in survey design is to specify necessary information, such as the effectiveness of the response of JCI accreditation standards, which is an effective tool used to implement the quality in the culture of Saudi hospitals. In addition, it is also the first step in the research design process (Malhotra and Birks, 2007).
JCI accreditation standards regarding healthcare facilities in Saudi hospitals have been clarified by telephonic interviews and executive staff surveys, which covered research needs. This is an effective tool used to implement the quality standards in Saudi hospitals.
According to Malhotra& Birks (2007), a better understanding of how influential the types of interviewing methods were may be obtained by considering how the survey was administrated under each method. In regards to telephone interviews, the respondent interacted with the interviewer without physically reading the questions, which limits the type of questions that can be asked to short and simplified ones. Electronic surveys are self administered via Google Docs Forms, which provides detailed instructions, and simplifies the process of creating a survey and inviting others to respond. All responses are gathered automatically into a Goggle Docs spreadsheet, which can be saved to computer as an Excel spreadsheet. The only requirement in order to do so is to have a free Gmail account (Teacherlink, 2010).
The required information was gathered from every question in the survey. However, some questions were not directly related to the needed information, but were asked anyway, because they can be crucial in regards to gaining confidence and cooperation of the respondents. These questions are called opening questions, and they are interesting, simple and non-threatening. In addition, as the surveys sample included executive staff, they like to express their opinions.
Secondary data
According to Mcnabb (2008), secondary data collection involves obtaining information related to the study from secondary sources such as those in published books or journals. This method has been used in the literature review section to detail the previous study results. The University of Hertfordshire’s library databases, e-journals, EBSCO, Google search engine, e-book, textbook, and IMC’s documents from its website were used to obtain the secondary information data. One, however, should be cautious while using published information, as a lot of care is required for using the material in a report.
Secondary data collection also has several advantages like that of the primary collection methods. Boslaugh (2007) has stated that one of the major advantages of secondary data is the cost effectiveness of the method as only a previously collected data is being reproduced and hence the researcher does not have to spend time or money on the data collection aspect of the JCI accreditation standards in KSA. Even purchasing secondary data would be cost effective compared to the cost involved for collecting a primary data set from individuals. In addition, time saving is also an important component of secondary data collection. As these data have been previously collected and stored in electronic format, the researchers on collecting specific requirements for the study instead of spending their working hours on framing a hypothesis and writing proposals for grants to carry out the research data collection and entry and supervising those involved in the project. Another advantage of secondary data collection is the large data that would be available for a given study and original electronic references. Though data conducted by individual researchers from a sample of the population would be relatively less, as it would not be possible for them to repeat the study every year or during every relevant period, the federal government however, conducts several surveys and collects data on specific issues regularly. The data collected on issues pertaining to the health related problems within a population are subjected to changes that include the health status and the health behaviour of the population. When such new data are collected annually or at regular intervals, it provides new insights to the researcher on the health status of the population over a period of time. The process of secondary data collection would, in some cases, involve the participation of experts and other related professionals that would not be possible while conducting small-scale research projects by individuals. For example, the federal health surveys included in this volume have used a complex sample design and weighting system, which has in turn aided in the computation of the population based on their health conditions and behaviours. Even though a small research project could possibly use similar techniques, it is always convenient to use samples that have been generalised among the specific population (Boslaugh, 2007).
However, collection of secondary data does suffer from some disadvantage and limitations as some the data might not pertain to the specific research question under study or certain necessary details may not be available in the secondary data collected in the previous studies. In other cases, the study might have not been conducted within a required geographic region or population of interest or during the years that might have been needed. In any case, can only work with data that exist, not what it wish had been collected. A related problem is that variables may have been defined or categorised differently thanit would have been chosen. For instance, a data set may have defined as only White/Other. A third difficulty is that, data may have been collected but are not available to the secondary researcher. For instance, address and phone number information for survey respondents may have been recorded by the original research team but will not be released to secondary researchers for confidentiality reasons. A secondary data set should be examined carefully to confirm that it includes the necessary data, and that the data are defined and coded in a manner that allowed accessing the data required (Sorensen et al, 1996).
According to Wernn et al (2007), accuracy of data collection is another major disadvantage of the secondary method. The initial problem lies with the source of the secondary data as to whether it has obtained from a primary or secondary source. The secondary data, if collected from a secondary source should be largely avoided. The next issue is about the organisation or agency that collected the data and the quality of the methodology followed by them, the data collection design and the credibility of the resources. The third issue is regarding the age of the data, as recent information garnered could be more useful compared to age old information whose usability to a present situation is often questionable. Another disadvantage associated with secondary data is the quality of the information gathered is often unknown as the reputation and the capacity of the agency or institute that had collected the information is vital while assessing the quality of the information collected. Additionally, if the collected data needs verification, the quality of information which includes details about the sampling plan, data collection method, the field procedures used, the training provided to the staff prior to data collection, the degree of non-responsiveness to the collection process and other possible sources of errors becomes a very vital requirement (Boslaugh, 2007).
The information regarding the JCI and its effect on the Saudi culture has not dealt with in many prior studies. In such cases, the accuracy of the secondary data source can also be a problem as the study deals with the stability of implementation of the JCI standards in hospital settings, which is a relatively new area of study. It is therefore necessary to evaluate the secondary data source along with other accredited data. Another problem with the study is the inability to obtain information by direct interviews with people at KSA as the complexity of the data collection process is usually costly and time consuming owing to the size of the sample (Bowling, 1997). However, the present study has managed to access the most current information about the JCI accreditation standards and its implementation in the quality management of healthcare facilities such as the KSA.
Limitation and opportunities
In order to conduct this research, some limitations and opportunities have faced. The limitations will rise within both the primary and secondary research. The limitations in the primary research are revealed in the performance, quality, and working time of the survey, and examining and analysing the answers. In regards to the secondary research, the limitations involve the reliability of the gathered information, data validity, and the confidentiality of the information. In addition, it must have ensured that the information is recent, and not outdated.
Sampling Techniques
Babbie (2011) also raised another concern about the use of the surveys in the data collection process regarding the source of participants. In order to conduct a meaningful survey, the individuals enrolled for collecting information should represent the population under study. In other words, the participants should be a subset of the population on whom the study is to be generalised.
According to Babbie (2010), there are two categories under, which the sampling process is classified: probability and non-probability sampling methods. In the present study, this method of sampling is more applicable thannon-probability method, which has used snowball sampling. The main characteristic of this research sampling that as a researcher in TQM area, it has identified some members of executive staff group or medical worker group in healthcare organisation, who first profile of TQM subject or JCI as a specific area wanted in this research as well as, who has interesting to present their opinions about this research. They have asked for their names, locations and positions. Through these referrals, research survey can be identified reasonably and effectively that is mostly useful when research survey subjects are difficult to locate. That has considered the main advantage of snowball sampling. In other hand, the main disadvantage is that it is non-random (Black, 2009). This research sample has included doctors, directors, head officers and managers with sampling size for six people.
Study contribution
The study has mainly aimed at the healthcare sector by aiding their policy-makers, management and other healthcare professionals in effectively implementing the JCI standards within the TQM department.
Conclusion
In conclusion, this chapter has dealt with the methodology that has followed for the entire study. Following the definition of a research problem, the purpose of the study has outlined in this chapters as well as objectives of the study and the study settings have explained. The types of research methodologies and the data types have explored in detail, survey design following which the sampling techniques and data collection and analysis process and the contribution of the study have then outlined.
Systematic Presentation of Data- Findings
Secondary Sources
This dissertation is based on both primary and secondary sources, which describe the impacts of JCI Accreditation on the work of healthcare facilities. First of all, literature review indicates that adoption of JCI standards can provide the following benefits: 1) improved risk management such as infection control; 2) better communication among members of the personnel, 3) better medication management and subsequent cost reduction; 4) better protection of patients’ rights (Joint Commission 2010b; Braun, Koss, & Loeb, 1999, p 283). The most important thing is that JCI standards emphasize the importance of continuous improvement of employees’ skills and competencies. JCI accreditation is not a single-time event; more likely, it should be regarded as regular efforts to enhance performance of a healthcare organization.
To some extent, academic sources demonstrate that implementation of JCI contribute to better performance of medical organizations. One should take into consideration that JCI standards are consistent with the principles of Total Quality Management (TQM). This framework emphasizes such principles as: 1) customer focus or patient-focus, 2) employee empowerment, 3) continuous process improvement (Al-Dabal, 1999). Existing academic literature suggests that these principles are quite applicable to the needs of healthcare institutions. Nevertheless, it should be noted the degree of implementation depends on culture, political system and those norms, which regulate the relationships among employees.
However, literature review has also pointed out several limitations of JCI accreditation, in particular, the cost of accreditation, which may not be affordable for healthcare organizations. Another drawback that has been identified is that JCI standards do not cover all aspects of healthcare (Jost, 1994). Furthermore, this validity of JCI accreditation is often criticized; namely, the inspection of JCI accredited hospitals revealed that many of these hospitals had many problems related to patient care and medication (Kowalczyk, 2007). Therefore, at this point one can say that literature review does not give a univocal answer about the effectiveness of JCI accreditation. Therefore, the adoption of JCI standards has expected to yield both qualitative and quantitative benefits, such as better workplace practices and reduction of costs incurred by medical institutions.
The government of Saudi Arabia actively promotes the adoption of JCI standards among healthcare organizations in this country. At this point, there are 33 accredited institutions: 31 hospitals, 1 ambulatory care organization and one clinical laboratory (Joint Commission International, 2011a, unpaged). These institutions are located in 13 cities of the country; the leading positions are occupied by such cities as Jeddah: Nine accredited institutions, Riyadh: seven accredited hospitals and Dammam: six accredited organizations (Joint Commission International, 2011a, unpaged). Some of these organisations have reported the effects of JCI accreditation. For example, JCI accredited Dr, SolimanFakeeh Hospital; the representatives of this institution claim that the new model brought the following improvements: 1) increased patient and staff satisfaction; 2) better compliance with governmental standards. Their findings can be summarized in the following chart.
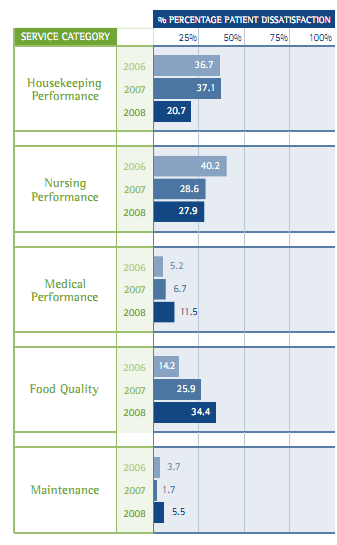
Additional, this medical institution pays close attention to such measurements as medication errors and safety procedures. This longitudinal chart indicates that after adoption of JCI standards, the number of workplace incidents dramatically decreased. Moreover, this statistical information is quite consistent with the initial hypothesis, advanced at the very beginning, in particular, the positive relations between JCI accreditation and patient safety.
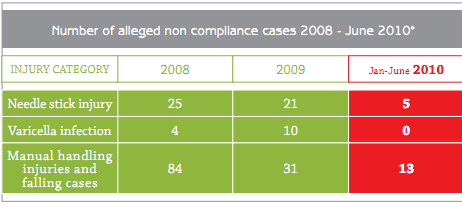
The main advantage of JCI implementation is that this model attaches great important to continuous assessment of quality and the use of different measurement tools. The adoption of these standards helped the hospital to uncover some problems, such as lack of safety precautions. The main requirement set by JCI is continuous reporting of incidents and defects and many Saudi Arabian hospitals like Dr. SolimanFakeeh Hospital benefited from it (Walton, Al-Omar, & Al-Maturi 2010, p 38). Based on these reports, the administration of a medical institution can better implement new policies and standards. Scholars argue that there are three factors, which affect patient safety: 1) management support; 2) adequate reporting systems; and 3) resource adequacy (Walton, Al-Omar, & Al-Maturi 2010, p 38). TQM approach addresses each of these factors. These quantitative and qualitative data shows that those Saudi Arabian Hospitals, which have implemented JCI standards were able to improve their performance especially in the long-term.
The Case of International Medical Centre (IMC)
At this point, it is necessary to discuss the experiences of a medical institution that has already adopted JCI standards and embraced the principles of total quality management; one of them is IMC (IMF, 2011, unpaged). IMC employs physicians from the United States and Canada. The administration of IMC is very keen insuring that every member of the staff is able to meet JCI standards.
This medical institution received JCI status ten years ago and since that time, its organizational structure underwent significant changes. JCI helped IMC provide training to the employees and design organizational processes within the hospital, so that it could meet the quality standards established in the United States. Later IMC entered into contract with many American medical institutions and this partnership enabled them to adopt the best practices used by healthcare organizations, for instance, teleconferencing, continuous education program, and more effective utilization of technologies, for example electronic health records (IMC, 2011, unpaged). Overall, these innovations have allowed them to make organization more oriented toward the needs of patients. In this case, one has to speak about the improved time management and less bureaucratic relations in the workplace.
In addition to that, the management of this medical institution emphasizes the importance of orientation programs for the new employees, regular training, and staff empowerment (IMC, 2011, unpaged). The innovations that were implemented by the management of International Centre are largely based on the principles of total quality management, especially, if one is speaking about regular training offered to the staff and orientation programs. Thus, over a period of 10 years IMC managed to improve its performance in a very dramatic way.
Primary sources
Several medical workers have been interviewed about the effects of JCI accreditation. The questions were related to the following issues: 1) the rationale for JCI accreditation; 2) the benefits of applying JCI standards; and 3) changes brought by this strategy. Six healthcare professionals were interviewed in the course of this research. Each of them has worked in those Saudi hospitals that have already implemented JCI standards and they agreed to tell us how TQM approach had affected these organizations. These are the questions that the respondent had to answer.
- The objectives for adopting JCI accreditation standards.
- The importance of JCI accreditation for the maintenance of healthcare facilities.
- The impact of JCI standards on the quality culture in a healthcare organization.
- The effects of JCI accreditation on leadership, teamwork, and beliefs about quality in Saudi hospitals?
- The indicators showing that Saudi hospitals have implemented JCI accreditation standards.
- The evolution of JCI standards in the future
This table summarizes the key responses of the interviewees.
Table 4 2: The key findings can be presented in table form.
This table is based on the responses given by those medical workers and executive staff who have already encountered with JCI accreditation. This people were asked to describe their perceptions of this innovation. Overall, this interview has enabled to gain better understanding of this process and these professionals has given us deep insights into the work of hospitals which implemented TQM approach.
Discussion and Analysis of Findings
Interpretation of findings
This study is largely based on the premise that it is possible to apply the principles of Total Quality Management to healthcare organizations. Despite the fact that this model was initially developed for the needs of manufacturing companies, it can be of great use to medical institutions (Bowling, 1997). The results of literature review and the survey that has been undertaken did not undermine the validity of this approach. More likely they have demonstrated that administrators should take into account the peculiarities of the organization, itself, and cultural environment in the region; otherwise such strategies TQM and JCI accreditation will not be successfully implemented. The growing number of healthcare organizations in the Kingdom of Saudi Arabia is willing to implement JCI standards. At the moment, there are more than thirty JCI-accredited hospitals in thirteen cities (JCI, 2011b, unpaged). To some degree this evidence indicates that, JCI standards and TQM approach are growing more and more popular in this country. However, one should take into account that the administration of a hospital should regard JCI accreditation only as the first step to continuous improvement; otherwise their attempts will be doomed to failure. On the whole, academic sources as well as the experiences of Saudi Arabian medical workers suggest JCI accreditation is conducive to better performance of medical institutions. Yet, one can say that implementation of JCI standards varies across countries and across hospitals. Furthermore, total quality management and JCI accreditation should not be perceived as interchangeable notions. In the following sections, this argument will be further elaborated.
The quantitative information provided by hospitals indicates that there is statistically significant relationship between the adoption JCI standards and patient safety. In particular, according to the report issued by Dr. SolimanFakeeh Hospital, the number of non-compliance cases was reduced by almost 75 per cent (Dr. SolimanFakeeh Hospital, 2010, p 52). Moreover, the same statement can be applied to the level of patient and staff satisfaction. It should be noted that the administration of Dr. SolimanFakeeh hospitals conducts surveys among patients and employees on a regular basis. This attentiveness toward the opinions of the staff and customers is an inherent part of total quality management. In part, these data partially supports the argument that adoption of JCI standards can improve workplace practices in a medical organization. It is worth mentioning that the administration of Dr. SolimanFakeeh Hospital referred primarily to JCI accreditation; they did not focus on total quality management. However, judging from their report, one can say that this institution actively embraced the principle of TQM, namely regular training offered to the staff, strong committeemen to the needs of the customers, and regular assessment of service quality. One should bear in mind that statistical data about Saudi Arabian hospitals is not sufficient for giving any definite answer about the effectiveness of JCI accreditation and total quality management. The thing is that Saudi Arabian hospitals began to adopt JCI standards only in 2001, while others did it in later years. This period is too short for in-depth analysis, and one has to take this limitation into account. Still, despite this limitation the statistical information that JCI-accredited hospitals have already made considerable progress, and they can enhance their performance even more in the year to come.
Apart from that, Saudi hospitals, which received JCI accreditation, were able to dramatically increase their revenues, but their total costs were increased (Dr. SolimanFakeeh Hospital, 2010, p 6). In part, this fact contradicts the principles of TQM which strived to reduce operational expenses of an organization. This is the difference between Saudi Arabian hospitals and Western medical institutions. Nonetheless, it is quite probable that the situation will change in the future because TQM cannot yield results immediately. The findings point to a very curious pattern; at the very beginning, JCI-accredited hospitals can record higher levels of injuries and other cases of non-compliance; such situation was observed in Dr. SolimanFakeeh Hospital, especially during the first two years after accreditation (Dr. SolimanFakeeh Hospital. 2008, p 22). However, in subsequent years the number of non-compliance cases declined. There are several ways of interpreting these data; one of them is that very often non-compliance cases such as medication errors or needle injuries are poorly reported. In turn, TQM approach is based on the premise that every deficiency has to be reported. Judging from this information, one can come to the conclusion that a hospitals, implementing TQM and JCI standards, should not look only for short-term gains. Such expectation overlooks the underlying principles of total quality management. These issues should be taken into consideration by administrators, who intend to change the policies and performance standards of Saudi healthcare organizations. These people must know what kind of pitfalls should be expected and how these pitfalls can be avoided.
It is also possible to argue both scholars and practitioners are not unanimous in their evaluation of the benefits, brought by JCI accreditation. Their key argument is that the outcomes of JCI implementation greatly depend on the goals, pursued by the administration of the hospital. For example, the critics of this accreditation believe that many hospitals implement JCI accreditation for marketing purposes; however, they do not apply the principles of total quality management and especially JCI accreditation standards (Kowalczyk, 2007, p 1). As a result, the quality of their work was improved significantly. This claim was supported by some of the respondents who were interviewed in the course of this study. Thus, one can argue JCI accreditation can yield the management of medical institution continuously assesses the results and promotes the adoption of best practices. Hence, the criticism of JCI accreditation can be explained by the fact that different hospitals approach this task, bearing different goals in mind. If the primary intention is to increase patient’s awareness about the clinic, the new policies are rather unlikely to bring significant quality improvement. Nonetheless, if administration genuinely intends to assure patient’s safety and promote employee education, they will genuinely benefit from adopting JCI standards and adopting TQM principles. This is probably the most important issue that has been identified in the course of this study.
Another pattern that becomes quite noticeable is that successful adoption of JCI standards is inevitably connected with deep organizational changes. Namely, one can speak about such changes to the shift toward patient-centered healthcare, elimination of formal barriers among the colleagues, willingness of the management to assist employees with their tasks, for example, by providing training to the staff. These changes are indispensible components of TQM philosophy, and they normally accompany JCI accreditation. Another very important issue, related to the introduction of JCI standards is that they are good tools for the evaluation of hospital’s performance. In this case, one has to speak about the scales which help to measure customer satisfaction or patient satisfaction. Furthermore, one should not overlook the important of such measurements as the number of non-compliance cases, like infection or injuries. Both Western and Saudi Arabian hospitals make full use of these assessment tools (Walston, Al-Omar, & Al-Mutari, 2010; Dr. SolimanFakeeh Hospital, 2010). These are the patterns, which are described in academic sources and which are supported by the empirical research. It has to be acknowledged that JCI accreditation still remains very costly, and many medical institutions in Saudi Arabia and in other countries cannot afford it. Therefore, the administration of medical institutions must make sure this investment is not spent in vain. By focusing only on marketing and short-term gains, they will overlook many benefits which total quality management can yield.
Difference between this research and findings of other people
At this stage, it is necessary to compare the results of the interview with the information provided by other researchers. Certainly, the scholars as well as our respondents expect JCI accreditation to improve the quality of patient care (Pasternak, 2009). Nonetheless, one should point out that in some cases, the expectations set for JCI model do not coincide. For instance, none of the respondents believed that cost-reduction was the main rationale of introducing TQM principles and JCI standards. As it has mentioned in the previous section, the advocates of TQM approach to medicine also emphasize the importance of cost reduction (Kanji &Moura, 2003). Those people, who have interviewed during this study, also expected the new model to contain costs. However, judging from their responses, the adoption of JCI standards enabled them to improve the quality of care, but it did not allow them to reduce their expenses. Thus, business administrators should determine why this goal has not attained. By doing it they manage to improve financial performance of Saudi Arabian hospitals in the future. Still, one should assume a very sceptical attitude toward JCI standards and total quality management. The outcomes of these innovations should been assessed from the long-term perspective. More importantly, the experts, who have surveyed, spoke about the necessity to enhance people’s trust in Saudi Arabian hospitals. Hence, it is possible to argue that failure to achieve cost reduction can be accounted by the difference in expectations. Another example that attracts attention is attitude toward patients’ rights. JCI strives to achieve better protection of patients’ rights (Joint Commission, 2010b). Those medical workers, who have interviewed, did not mention this task. To some degree, this difference can be explained by the fact that the respondents viewed protection of patients’ rights as something self-evident.
Currently, Saudi Arabian hospitals are willing to embrace TQM approach, which proved to be effective in other countries. Now, this country has the largest proportion of JCI accredited hospitals in the Middle East. Moreover, Saudi medical workers are fully aware of the improvements brought by this method. Apart from that, Saudi Arabian experience indicates that JCI can productively cooperate with governmental organizations, such as Central Board for Accreditation of HealthCare Institutions. This partnership ensures that medical institutions do try to reach the highest performance standards. Overall, it is possible to say that the differences in JCI implementation can be accounted by the fact Saudi hospitals have closely monitored by the state, while Western hospitals are more independent. These examples indicate that implementation of total quality management and JCI accreditation standards are strongly influenced by political culture of the country. Additionally, this case illustrates that assistance of governmental institutions can be quite beneficial for JCI.
The responses of the interviewees show that there is a significant relation between the JCI accreditation and improvement of patient care. Moreover, it is quite permissible for us to reject the null hypothesis. These improvements include better risk management and infection prevention, better organizational processes, and improved cooperation. Yet, researchers and business administrators stress the importance of employee empowerment (Al-Dabal, 1999, p 14). The healthcare professional, who participated in this study, did not pay the same attention to this issue. Thus, one can say that the expectations set for JCI accreditation often vary. These expectations may depend on social or cultural environment in the country. The thing is that in Saudi Arabian organizations, the power distance between employees is very long, and people are more likely to pay attention to the formal barriers existing between the top management and frontline personnel (Hofstede, 2011, unpaged). Furthermore, one should bear in mind that the level of uncertainty avoidance is much higher in Arab countries than in the Western world. This means that the employees of Saudi Arabian hospitals are less willing to take risks unlike their American or European counterparts (Hofstede, 2011, unpaged). Overall, the notions of power distance and uncertainty avoidance can help us understand why some of the TQM principles such as employee empowerment were not fully applicable to Saudi Arabian hospitals. Yet, it is necessary to emphasize the point that the exact outcomes of JCI accreditation has effectively measured only after a longer period. Erasure of formal barriers and democratization of the workplace cannot happen instantaneously. Many Saudi hospitals have been accredited by JCI only several years ago. It is quite probable that changes in managerial style will occur only in the future.
This information have used by those administrators who will try to implement TQM approach in Saudi Arabian hospitals. For instance, they should bear in mind that in many Saudi Arabian hospitals the establishment of JCI standards did not contribute to the cost reduction. Moreover, employee empowerment is an inseparable part of TQM, and this organizational change has not observed in Saudi Arabian hospitals. Overall, these results have made me firmly convinced that there is no universal pattern for the adoption of TQM principles. The management has to consider such issues as business culture, political system of the country, the values of employees and patients and so forth; otherwise, their efforts will not succeed.
The key conclusions
These findings can change several perceptions of JCI accreditation and Total Quality Management. First, these notions have not considered as something synonymous. In itself, JCI accreditation only indicates that at a certain point in time, a hospital is able to meet certain performance standards. Moreover, it shows that its employees possess certain skills and competences. However, as it has said many organisations adopt this approach mostly for marketing purposes, and in this case, one cannot speak about genuine shift to TQM approach. The second issue that have not overlooked is that one should not expect JCI and TQM implementation to bring immediate improvements. The thing is that at the beginning the adoption of TQM approach can only allow the hospitals to pinpoint the deficiencies in organizational design. Only through continuous training of the personnel and meticulous reporting, the administration will be able to eliminate these deficiencies. The third aspect is cultural differences, which can exist between countries. The business culture of Saudi Arabian organization is not similar to that one of Western medical institutions. In Saudi Arabia, formal relations among members of the staff play more important role, and these barriers cannot easily erased. Therefore, people should not perceive TQM and JCI accreditation as universal experiences, which are similar in different countries of the world. This discussion leads to the conclusion that JCI accreditation is only a part of TQM philosophy. Overall, the findings suggest that there is a positive relation between the adoption JCI standards and improvement of patient safety and customer satisfaction. It is possible to single out. Such perquisites for successful implementation of JCI standards and TQM principles: 1) willingness of the administration to improve quality of patient care, rather than intention to advertise the hospital; 2) skilful use of different measurement tools, which evaluate the degree of patient and employee satisfaction; 3) meticulous reporting of non-compliance cases such as, infections or needle injuries; 4) regular training provided to the employees; 5) patient-cantered healthcare. These conditions are indispensible for the success. The findings of this research has utilized by those Saudi hospitals, ambulatory services and medical laboratories, intending to apply the principles of total quality management.
Summary, Conclusions and Recommendations
Summary of main findings
At this point, it is necessary to summarize the major findings of this research.
- The adoption of JCI standards and TQM principle results in higher levels of patient satisfaction and reduced number of medical errors and improved infection control.
- Total quality management is associated with higher levels of staff satisfaction.
- The outcomes of JCI and TQM implementation are strongly dependent on the motives and goals set by the hospital administration.
- Successful JCI accreditation and TQM implementation inevitably entail such organizational changes as patient-cantered healthcare, continuous emphasis on the improvement of quality of care and less bureaucratic relations among members of the personnel.
- Hospitals, which adopted the principles of total quality management, pay more attention to the measurement of performance. These organizations conduct surveys among patients and employers; moreover, they continuously record every case of non-compliance, such as needle injuries or medication errors. These methods enable them to pinpoint drawbacks in their everyday practices and subsequently evaluate them.
- JCI can successfully cooperate with governmental organizations such as the Ministry of Health. This cooperation is particularly important when we are speaking about the dissemination of best practices to other medical institutions of the country.
- In addition to that, JCI accreditation enables the hospital to establish partnership with foreign medical institutions. The most eloquent example is IMC in the Kingdom of Saudi Arabia. This healthcare organization cooperates with several hospitals in the United States such as Cleveland Clinic. This partnership enabled them to better adopt the best practices used by leading U.S. hospitals. It seems that other healthcare institutions should use this approach. These are the major patterns, which have identified in the course of the study. Overall, they confirm the initial hypothesis of this research, namely the assumption that JCI accreditation and total quality management results in the improvement of patient safety and quality of care. However, these findings do not refute several criticism of JCI. One of them is the cost of JCI accreditation; for many hospitals in Saudi Arabia, these expenses are hardly affordable.
One should consider some other issues. First, JCI accreditation and total quality management should be regarded two synonymous concepts. If a hospital receives JCI status, it does not necessarily mean that this institution will adhere to the principles of total quality management, such as continuous improvement of business processes, personnel empowerment, and orientation toward long-term objectives. Secondly, the implementation of TQM principles is not a universal experience; it has affected by social and cultural environment of the country. Moreover, it depends on the work experience of the staff. For example, power distance and attitude toward risks in Saudi Arabian organizations differ from Western medical institutions, and hospital administrator needs to consider these differences. Additionally, hospitals administrators need to determine whether the employees have any prior experience of TQM principles. Those medical workers, who are new to this managerial philosophy, are less likely to benefit from it.
It is has admitted that this study has several limitations. First, the number of interviewees should have increased. This would have allowed me to collect data that are more reliable. Still, this study has both theoretical and practical value. First, it describes the organizational changes in hospitals, which attempt to implement the principles of total quality management. Secondly, on its basis one can develop a set of guidelines for healthcare administrators. These people must know how to involve the staff into this process and how to evaluate the performance of these employees. More importantly, administrators need to know what kind of difficulties they may face when introducing JCI standards and how these difficulties can overcome.
Conclusions and directions for further research
This dissertation can give rise to further research. In particular, it is necessary to determine how cultural distinctions affect the implementation of TQM model. For this purpose, one has to compare the organizations changes, which occur in Saudi Arabian hospitals with those ones, which take place Western medical institutions. Moreover, there is no universal pattern for the implementation of total quality management and business administrators can employ different strategies. Hence, one should compare and evaluate these strategies and identify the most effective ones. The results of this assessment can greatly benefit hospital administrators. Another question, which is also of great interest, is the economic benefits of JCI. The hospitals that have received JCI status have said to reduce their operational expenses. However, statistical data provided by some Saudi Arabian hospitals indicates that this objective has not achieved. Therefore, the researchers should analyze their financial reports and determine whether the adoption of JCI standards and TQM principles leads to cost reduction. In order to gain a better understanding of this question, one should take those healthcare organizations that have accredited by JCI at least five years ago. The analysis of longitudinal data will enable to determine the long-term economic effects of introducing JCI standards and TQM principles. Another very interesting task for the researchers is to determine what kind of factors affect the implementation of TQM models in medical organizations. One can certainly assume that they include employee involvement, the turnover rate, job security, or employee satisfaction, but this is just an assumption that has to be tested. Overall, these directions for the research are directly relevant to the needs of medical institutions in Saudi Arabia. Provided that, one manages to give accurate answers to these questions, these findings can be of great help to hospital administrators. Currently no one denies the importance of total quality management for the needs, but the questions, which have been identified in this section, still require further research.
Recommendations
Because of these findings, one can propose several recommendations to the management of healthcare organizations. First of all, they should perceive JCI accreditation only as a marketing tool. JCI status does not mean that the hospital has eliminated every drawback or deficiency. Without continuous focus on improvement, personnel involvement, and assessment of employees’ performance, JCI accreditation will not bring expected results. Furthermore, the second recommendation is to apply a set of measurement tools in order to evaluate the progress of the organization. Special attention should paid to such criteria as patient and staff satisfaction, the number of non-compliance cases (medication errors, injuries, and infections), the operational expenses, the number of patient re-admissions, etc. These measurement tools will ensure that quality problems have identified as quickly as possible. Moreover, the third step that should been taken is to eliminate the barriers between various departments of the hospitals. The work of the employees should focus on the needs of the patients, and bureaucracy must not come between them. This requirement is an essential element of total quality management. In addition, apart from that, the administration should offer training to the employees every three years. This strategy will ensure that the skills of the staff have kept up-to-date. Also, the previous strategies have fully adopted only if members of the staff work together for a long time. Those hospitals, which have high turnover rate, may fail to do it because they have to spend both time and money on the recruitment of skilled employees. Thus, the administration must reduce turnover rate by offering adequate compensation to the personnel and improving their work conditions. Ultimately, the management of hospitals also has to ensure that the members of the staff are aware about TQM; in some cases, it might be necessary to hold seminars or even lectures for them so that they could understand the expectations, which they need to meet.
These recommendations are consistent with the principles of TQM and JCI accreditation standards. By following them, the management of healthcare organizations will improve both patient care and reduce operating costs. It has noted that these recommendations have intended not only to those hospitals, which plan to receive accreditation from JCI. These strategies can be equally useful for those clinics, which are willing to improve the quality of their service but cannot afford to work with JCI. As it has been for total quality management, it has regarded mostly as a set of principles, which govern healthcare institutions. They have not necessarily connected with JCI or any other accreditation organization.
Reflection
Prior to starting work on this dissertation, I spend some time on the development of my research schedule. The thing is that a student, who is writing such a paper, has to plan his/her activities very meticulously. In particular, this person needs to know how much time each stage of the research is going to take and how to stay within the timelines, set by the scientific advisor. Overall, this schedule has been of great help to me since I was more aware of how this dissertation was progressing. According to David Kolb’s model, my learning style has characterised as assimilator, which means that I tend to rely more on reflective observation and abstract conceptualization (Kolb, 1984). On the one hand, it helps me to see the regular patterns when I analyze information. Yet, at the same time, I find it more difficult to apply theoretical concepts to real life situations. This ability was particularly important for me when I was developing recommendations for hospital administrators. At that point, I needed to adjust the theoretical principles of TQM to the needs of healthcare organizations, and this turned to be a very challenging task for me.
My dissertation consists of several chapters. While writing the introductory section, I wanted to learn as much as possible about this topic and pose those research questions, which had not fully answered. At this stage, I learn about the basis principle of TQM and JCI accreditation standards. At this part, I needed to understand how the performance of clinic has measured, since without this knowledge I would not have been able to formulate the key hypothesis. Having written the introductory section, I began to collect evidence related to JCI accreditation and the use of TQM models in hospitals. This information had to be included in the Literature Review Section. This was by far the most consuming part of the research. I needed to find those books and articles, which give adequate assessment of JCI accreditation and its benefits for medical institutions. At this stage, students should avoid attempts to fit the facts to the initial hypothesis. It would have been a great mistake of me to mention only those sources, which discuss the benefits of JCI accreditation. Such an approach undermines the validity of the research. This is why I tried to understand why JCI has criticised and determine whether this criticism has substantiated. While looking for the information about the effects of JCI implementation, I had to find reliable statistical data. I was particularly interested in the numerical information about patient safety or the level of satisfaction. This information enabled me to determine whether my initial hypothesis was right. It has noted that while I was searching for the information, I came across several the reports of several hospitals. They emphasized the importance of total quality management and had JCI status, but they did not provide any examples that would illustrate the benefits of these two models. They seemed to be two unsubstantiated and this is why I decided not to include them. Overall, this assignment has demonstrated to me that a researcher must be able to assess academic sources in terms of their relevance and reliability. Furthermore, while doing this research, I learned more about different search engines and especially Google. Such free service as Google questionnaire was of great help to me. Internet technologies helped me to contact several people, who had not contacted in person or by phone.
The third chapter of this dissertation was Methodology. At that point, I had to select the most appropriate methods of collecting primary data. I decided to choose such method as unstructured interview since it allows the interviewee to express his/her thought more freely. Overall, conversations with medical workers enabled me to understand the peculiarities of TQM adoption and JCI accreditation. In this stage, I can say that it was necessary to broaden the range of questions. Some of them have presented in Likert scale format, since in the way one can better quantify the data. More importantly, enlarged sampling would have increased the validity of my findings. Moreover, if I had had more time, I would have interviewed a large number of people from different hospitals. These activities allowed me to learn more about the advantages and disadvantages of different research methods. In the future, I will be better able to design the research.
The fourth chapter is Presentation of Findings. At that stage, I needed to distinguish the most significant findings that derived from my own research and from academic sources. This was probably the most challenging task. This activity taught me to better assess information and systematize it. This skill was of great use for me when I was analyzing the main results. I needed to understand whether there is significant relation between the adoption of JCI standards and improvements in the work of medical institutions. It must be acknowledge that I should have analyzed larger samples of data. The last chapter of my dissertation proved to be much easier, since I had already done the major part of the research. In this section, I tried to distinguish the key findings of the study as well as their theoretical and practical implications. The main problem for me was to translate my findings into recommendations for managers.
I encountered several difficulties, while doing this research. First, I have no time to go to Kingdome of Saudi Arabia and visit International Medical Centre in Jeddah. It was not easy for me to find those people, who have prior experience of TQM implementation. Because of working relationship, I have help from my director in previous job. I have to admit that this person has helped me with the selection of subjects for the interview. This research made me even more interested in JCI standards. When I was working in International Medical Centre (IMC) from begging time as a representative of patient affairs department for 4 years also I moved to Project management department, I became convinced that cooperation with JCI could greatly improve the work of medical organisations. IMC cooperated with JCI while developing its healthcare facilities.
Overall, this experience has taught me a great deal about the peculiarities of dissertation process and research. In my opinion, the topic that has examined in this study definitely merits more attention. Total Quality Management and accreditation has believed to produce positive effects on medical organizations. However, the methods of implementation differ significantly from one another. Thus, one needs to determine which approach is the most appropriate one. This knowledge can greatly improve the work of medical institutions in Saudi Arabia and in other countries as well. This research increased my knowledge about the development of healthcare system in Saudi Arabia that motivated me more to doing PHD research in International public health strategy via this knowledge I can cover these five areas according to PHD area; “public private partnerships and marketisation, globalization and health, clinical trials, regulation, and intellectual property, and comparative health systems”.
References
Al-Dabal, J. (1999) Is total quality management enough for competitive advantage? Realities of implementing change initiative in organizations: with examples from the United States and the developing world. Thesis (Master). ISBN1581121261.University of Hull.
Al-Abdulkareem, A. Seifeddin, G., &Bellal, M. (1998) ‘Consanguineous marriage in an urban area of Saudi Arabia: Rotes and adverse health effects on offspring’. Journal of community health. Vol. 23, pp. 75-83.
Alsulaiman, A. and Hewison, J. (2006) ‘Attitudes to parental and pre-implantation diagnosis in Saudi parents at genetic risk’ prenatal diagnosis. Vol. 26, pp. 1010-1014.
Babbie, E. (2010) The Practice of Social Research. 12th edn. USA: WADSWORTH CENGAGE LEARNING.
Babbie, E. (2011) The Basics of Social Research. 5th edn. USA: Wadsworth Cengage Learning.
Berg, B. (2007) Qualitative research methods for the social sciences. 6th ed. Boston: Pearson education, Inc.
Black, K (2009) Business Statistics: Contemporary Decision Making. 6thedn. USA: John Wiley & sons, Inc.
Boslaugh, S. (2007) Secondary Data Sources for Public Health. United Kingdom: Cambridge University Press. Web.
Bowling, A. (1997) Measuring health – a review of quality of life measurement scales, 2nd edn. Buckingham: Open University press.
Braun, B. Koss, R. & Loeb, J. (1999) “Integrating Performance Measure Data into the Joint Commission Accreditation Process.” Evaluation and the Health Professions22(3): 283-97.
Bryman, A. (1989) Research Methods and Organisation Studies. London: Routledge.
Bittles, A. (2001) ‘Consanguinity and its relevance to clinical genetics’. Clinical Genetics. Vol. 60. 2001. pp. 89-98.
Central Board for Accreditation of Healthcare Institutions (2010) Hospital Accreditation Guide. Web.
Conjoined Twins (2011) Kingdom of humanity.Web.
Crowther, D. and Lancaster, G. (2008) Research methods: a concise introduction to research in management and business consultancy. 2nd edn. UK: Elsevier Butterworth- Heinemann.
Dale, B. (1994) Managing quality. 2nd ed. Hertfordshire: Prentice hall.
Delbridge, R. and Kirkpatrick, I. (1994) ‘theory and practice of participant observation’ in P. Wass and P. Wells (eds) Principles and practice in Business and Management Research, Aldershot: Dartmouth, pp. 35-62.
Dr.SolimanFakeeh Hospital (2008) Hope for the Future: Corporate Responsibility Report.Web.
Dr.SolimanFakeeh Hospital (2010) Corporate responsibility report. Web.
Eggli, Y & Halfon, P. (2003). A conceptual frame work for hospital quality management. International Journal of Health Care Quality Assurance, 16(1), pp. 29-36.
Fisher, N (1996) Cultural and ethnic diversity: a guide for genetics professionals. USA: Acid free paper, The Johns Hopkins University Press.
Graziano, A. And Raulin, M (2004) Research Methods: a process of inquiry. 5thedn. Boston: Person.
Ghauri, N. and Gronhaug, K. (2005) Research methods in business studies: a practical guide. 3rdedn. London: Financial Times Prentice Hall.
Hofstede, G (1980) Culture’s consequences International differences in work-related values. Beverly Hills, CA: Sage.
Hofstede. Geert. (2011) Arab World: Cultural Dimensions. Web.
Hudelson, P., Cléopas, A., Kolly, V., Chopard, P., &Perneger, T. (2008)What is quality and how is it achieved? Practitioners’ views versus quality models.Quality and Safety in Health Care, 17 p.31-36.
International Medical Centre (2000a) About IMC: History. Web.
International Medical Centre (2000b) About IMC: JCI Accreditation. Web.
International Medical Centre (2008) Home: Overview of IMC. Web.
International Medical Centre (2011) Home: Overview of IMC. Web.
Joint Commission (2010a) Home: About Us. Web.
Joint Commission (2010b) Home: Topic Details: Facts About Joint Commission International. Web.
Joint Commission International (2008)Common Questions and Answers Regarding JCI Accreditation, Hospital Accreditation, and These Standards. Web.
Joint Commission International (2009a) Home: About Joint Commission International. Web.
Joint Commission International (2009b) Home: Accreditation Certification Process: Why become accredited?: JCI Accreditation process timeline. Web.
Joint Commission International (2011a) Joint Commission International Accreditation Standards for Hospitals: Standards Lists Version. 4th edn. USA: the Joint Commission on Accreditation of healthcare organizations.
Joint Commission International (2011b) “Regional Focus: Kingdom of Saudi Arabia”. Web.
Joint Commission Resource (2010) Home: The Joint Commission Organisation. Web.
Jovanovic, B. (2005) ‘Hospital accreditation as method for assessing quality in healthcare’. International Journal for Quality in Health Care. 13(3-4): 156-7.
Jost, T.(1994)‘Medicare and the Joint Commission on Accreditation of Health Care Organizations: A healthy relationship?’.Law & Contemporary Problems, 57(4), 15-45.
JTaylorBUProject (2009) Academic Work : Health Care System. Web.
Kanji, K. and Moura, P. (2003) ‘Sustaining health care excellence through performance measurement’ J total quality management. Vol. 14, No. 3, pp. 269-289.
Kolb. D. (1984)Experiential learning: experience as the source of learning and development. New York: Prentice-Hall.
Kowalczyk. L.(2007) “Surprise check faults MGH quality of care”. The Boston Globe. Web.
Mathotra, N. and Birks, D. (2007) Marketing Research an applied approach. 3ed edn. England: Prentice Hall Inc. Web.
Mays, N. and Pope, C. (1995) ‘Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research’. National Center for Biotechnology Information. 311(6996) pp. 42-45. Web.
McNabb, D. (2008) Research methods in public administration and nonprofit management.2nd edn. USA: M.E. Sharpe, Inc.
McQueen, R. and Knussen, C. (2002) Research methods for social science. Essex: Pearson Education Ltd.
Ministry of Health (2009) Statistics Department- Years Book 2009. Web.
Ministry of Health (2010) Conjoined Twins. Web.
Ministry of Health (2011) Main: Vision and Mission. Web.
Middle East institute(2009) Viewpoints Special Edition, The Kingdom of Saudi Arabia, 1979-2009: Evolution of a Pivotal State. Web.
National Guard Health Affairs (2010) Home: Media Center: News: JCI Re-accreditation. Web.
Pasternak, D. (2009) Hospital Accreditation A Framework for the Systematic Improvement of Patient Car. Web.
Robson, C. (2002) Real world research: a resource for social scientists and practitioner-Researchers. 2nd edn. UK: Blackwell Publishing Ltd.
Saad, M. (2011) Joint Commission International Meeting All the Standards of Health Care and Safety. Web.
Saunders, M., Lewis, P., &Thornhill, A. (2009) Research Methods for Business Students.5th edn. England: Person Education Limited.
SeKaran, U. (2003) Research methods for business. 4th ed. New York: John Wiley & sons.
Sorensen, H., Sabroe, S., & Olsen, J. (1996) ‘ A Framework for Evaluation of Secondary Data Sources for Epidemiological Research’. International Journal of Epidemiology.Vol. 25. No. 2. Web.
Sofaer, S. (1999). Qualitative Methods: What Are They and Why Use Them? HSR Health Services Research, 34 (5) Part II p. 1101-1118.
Spencer, L. Ritchie, J. Lewis, J. & Dillon, L. (2003). Quality in Qualitative Evaluation: A framework for assessing research evidence. National Centre for Social Research.Government Chief Social Researcher’s Office.
Shi, L., & Singh, D. (2008). Delivering health care in America: A systems approach. 3rd edn. Boston: Jones and Bartlett Publishers.
Tabish, S. (2010) ‘Assessment Methods in Medical Education’. International Journal of Health Sciences.Vol 2, No 2(2). Web.
Teacher link (2010) Teacher Resource. Web.
The Washington Post (2005) National News.Accreditors Blamed for Overlooking Problems. Web.
The Boston (2007) News: Local. Surprise check faults MGH quality of care. Web.
Ulin, p., Robinson, E., &Tolley, E. (2005) Qualitative Methods in Public Health: a field guide for applied research. USA: Jossey-Bass.
Walston, S. Al-Omar B, Al-Mutari F, (2010) “Factors affecting the climate of hospital patient safety: A study of hospitals in Saudi Arabia”, International Journal of Health Care Quality Assurance, Vol. 23 Iss: 1, pp.35 – 50.
World News (2011) Hospital Accreditation. Web.
Wrenn, B., Stevens, R., & Loudon, D. (2007) Marketing research: text and cases. 2nd edn. USA: The Haworth Press, Inc. Web.
Student Health Center, New Mexico State University, Las Cruces 88003. Web.
Evaluatingaccreditation(editorial).InternationalJournalforQualityinHealthCare2003;15(6): 455-6.
Shaw D. C. Toolkit for Accreditation Programs: Some issues in the design and redesign of exter- nal health care assessment and improvement systems. International Society for Quality in Health Care,Australia;2004.
Quality andaccreditation in Health Care services. A globalreview. Geneva: World Health Organization;2003.
Joint CommissionInternational accreditation Standards for Hospitals. Joint Commission International,USA,2003.
Alriyadh (2009) Local News: Board of Directors, International Medical Center in Jeddah, acknowledges its expansion. Web.
AlKhenizana, A and Shaw, C. (2010) Assessment of the accreditation standards of the Central Board for Accreditation of Healthcare Institutions in Saudi Arabia against the principles of the International Society for Quality in Health Care (ISQua). Public Medical Centre Journal list Quarterly [Online]. 30(5) pp. 386–389. Web.
Bate, P. (1995) Strategies for Cultural Change. Butterworth-Heinemann, Oxford.
Bowling, A. (1997).Research methods in health, investigating health and health services. 2nd edition. Open University Press, Buckingham.
Burnes B. (2000). Managing Change: A Strategic Approach to Organizational Dynamics. 3rd ed. Harlow, Essex, England: PearsonEducation.
Buse, K., Mays, N. and Walt, G. (2005). Making Health Policy. Berkshire: Open University Press.
Bhuian, S., Abdulmuhmin, A., and Kim, D. (2001).Business education and its influence on attitudes to business, consumerism, and government Saudi Arabia.Journal of Education for Business, 76(4) p.226-230.
Coulter, A. (2002) After Bristol: putting patient at the centre. British Medical Journal, 324 p. 646-651.
Chen J, Rathore SS, Radford MJ et al. (2003) JCAHO accreditation and quality of care for acute myocardial infarction.Health Aff, 22 p.243–54.
Chin, R., & Benne, K. D. (1969). General strategies for effecting changes in human systems.In W. G. Bennis, K. D. Benne, & R. Chin (Eds.), The planning of change (pp. 32–59). New York: Holt, Rinehart & Winston.
Cumming, T.G. and Worley, C.G. (2001). Organizational development and change.7th edition, Cincinatti, South-Western College Publishing.
Davidson, D. (2005). The organizational development cycle: putting the approaches into a process. In Peck, E. (Ed.), Organizational Development in Healthcare (pp.63-75).Radcliffe Publishing Ltd, UK.
Helen Ziegler & Associates (2011) The Health Care System in Saudi Arabia.
HCIA/JCAHO (1993).Comparing Quality and Financial Performance of Accredited Hospitals. Oakbrook Terrace: JCAHO. Joint Commission International(JCI), (2010).Six Construct will build the Cleveland Clinic in Abu Dhabi. Web.
Joss, R. and Kogan, M. (1995) Advancing quality total quality management in thenational health care services. Bukingham: Open university press.
Koch, H. (1993) Total quality management in health care. Essex: Longman.
Kotler, P. (1994). Marketing management, analysis, planning, implementation andcontrol. Chapter 3&18, pp. 130-145. New Jersey: Prentice Hall.
Munro-Faure, L. and Munro-Faure, M. (1992) Implementing total quality management.London: Pitman publishing.
Oakland, J. (1993) Total quality management. 2nd ed. Oxford: butterworth-HeinemannLtd.
Rahman, S. (2004) the future of TQM in past. Can TQM be resurrected?.J Total qualitymanagement. Vol. 15, No. 4, pp. 411-422.
Shortell, S.M., O’Brien, J.L., Carman, J.M., Foster, R.W., Hughes, E.F.X., Boerstler, H., O’Connor, E.J. (1995). Assessing the Impact of Continuous Quality Improvement/Total Quality Management: Concept versus Implementation. Health Services Research, 30(2) p.377-401.
Thiagarajan, T. and Zairi, M. (1997). A review of total quality management in practice: understanding the fundamental through example of best practice applications- Part 1, The TQM Magazine. 9(4) p.270-286.
Vanisina, Leopold S. (1990) Total Quality Control: An Overall OrganizationalImprovement Strategy. National Productivity Review, pp 57-74.
Walshe, K (2003). Regulating Healthcare, A prescription For Improvement.Open University Press. England.
Weiner, B.J., Alexander, J.A., Shortell, S.M., Baker, L.C., Becker, M., and Geppert, J.J., (2006). Quality Improvement Implementation and Hospital Performance on Quality Indicators. HSR: Health Services Research 41 (2), p.307-334.
Wojner AW. (2001). Outcomes Management: Applications to Clinical Practice. St Louis, Mo: Mosby.
World Health Organization (2003) Quality and Accreditation in Health Care. Geneva: WHO.
Weiner, B. Shortell, S.M. and Alexander, J. (1997). Promoting Clinical Involvement in Hospital Quality Improvement Efforts: The Effects of Top Management, Board, and Physician Leadership. Health Services Research, 32 (4) p.491:510.
Appendices
Appendix 1: Proposal Research
Joint Commission International (JCI) Accreditation standards for healthcare facilities development. The case of International Medical Centre(IMC).


Background
The World Health Organization, which has known more universally by its acronym, “WHO” consideredthe main organisation in the healthcare sector. WHO has authority to coordinate health within the United Nation Systems. In addition, it is able to provide leadership on international health issues, rules standards, health research processes, and policies and procedures (WHO, 2010). Moreover, in 2005 it identified cooperation centres for Patient Safety Solution, which are the Joint Commission and Joint Commission International “JCI” (Collaborating Centre for Patient Safety Solutions, 2010). Since 1990s, JCI evaluated the performance of healthcare facilities outside of the United States, which do not including profit organisations. JCI’s mission extends the Joint Commission via assisting international healthcare organisations, healthcare ministries, public healthcare agencies, and others to advance the performance quality and safety of global patient care for approximately more than 200 hospitals in 80 countries such as, International Medical Center (IMC) in Saudi Arabia (The joint commission: 2010, joint commission international: 2010).
The Joint Commission International’s mission is: “To continuously improve the safety and quality of care in the international community through the provision of education and consultation services and international accreditation and certification”. JCI authority of healthcare facilities, which is responsible for implementing high standards of medical affairs. The IMC’s development was done through the JCI’s supervision that wielded within IMC’s conception, construction and design as well as overseeing medical procedures and facilities. The IMC logo is considered to be a tree, which has been made up of five crescents, it symbolizes the body, mind and soul. It will be cared for in order to achieve optimum health, but the lower crescents; which start from the trunk and roots, symbolize international standards and holy ethics, which are essential for the survival of the tree (IMC,2010).
Research Question
To what extent the Joint Commission International (JCI) Accreditation standards improves healthcare facilities?
Aims
The aims of this research are to evaluate and analyze the extent to which JCI’s international standards are applied in Saudi Arabia, and to what degree they are followed through assessing the different factors involved in Total Quality management (TQM),
Objectives
- To understand significance purpose and goals of Joint Commission International in Healthcare sector.
- To assess the International Essentials for Health Care Quality and Patient Safety according to JCI accreditation standards.
- To assess the extent to which healthcare facilities have improved throughout the implementation of JCI; medical care, patient rights, patient satisfaction.
- To analyse the consistent implementation of the mission of International Medical Centre in KSA following the international standards of JCI accreditation.
Literature Review
This section has intended to explain goals of this research. IMC goals achieved JCI accreditation standards. Some purposes will be considered to clarify the impact of JCI accreditation standards to develop healthcare facilities.
World Health Organisation Collaborating (WHO) Centre for Patient Safety Solutions
Since 2005, both the Joint commission and Joint commission International have designated as the WHO bodies for patient safety solutions. WHO has established international network to clarify performance, and evaluate patient safety solutions. It recognises present solutions, which have a potential applicability to a vast variety of countries. It has established linkages with main organisations and individuals, which have expertise in-patient care safety (The joint commission, 2010).
High 5s Project
The Collaborating Centre in 2007 established High 5s Project to implement the standards protocol for patient safety solutions for more than five years. There are five solutions areas, which have been defined as the concentration of the High 5s project:
- Avoidance of medical care errors.
- Warning of a wrong procedure or wrong patient surgical mistake.
- Prevention of uninterrupted medication errors.
- Regular dosages of anaesthesia to prevent errors.
- Promotion of effective infection control and focus on hand hygiene practices.
International Accreditation and Certification
International experts have developed the standards to achieve expectations for structures, processes and outcomes for healthcare facilities. International patients’ safety objectives concentrate on a variety of areas in healthcare, evidence and solution to these problems. The standards adapt to the religious and local cultures (The Joint Commission, 2010).
International Consulting
In 1994, Joint Commission International Consulting provided technical assistance services and education for healthcare organizations, ministries of healthcare and other countries outside of the United States. Through the previous 15 years, JCI created a record of supporting healthcare facilities for organizations and governmental agencies. JCI assisted with the development of clinical services by issuing practical solutions, advancing the patient care quality, supplementing patient safety and achieving global standards and other goals. JCI consulting recommends the following services:
Improving operations, progressing a national or regional quality estimate system, education and networking services, evaluating performance and advancing a quality program to improve and support standards compliance (The joint commission, 2010).
JCI Standards
Joint Commission International has about 300-accreditation standards, which healthcare facilities and hospitals must meet as well as 1200 measurable factors (Medical Tourism Magazine, 2010). International Medical Centre has implemented JCI Accreditation standards; Patient Centred standards and Organization Standard:
- Patient-Centred Standards (PCS). Primary care centre should define the type of services, which has implemented to the community and patients. In addition, these services could be provided from birth to death of the patients, which needs to connect to their health care needs. It is recommended that Healthcare organisation must clarify specific services to be provided and interface between the care they provide and other services of healthcare system. On the other hand, how to effectively provide healthcare services to support patient care and patient rights, ensure the perfect assessment of the patients needs, and also it will be through care and patient education. In all these activities, the patient will be the goal of every aspect of the healthcare organisation (Joint Commission International, 2010). Some PCS standards, which have been implemented in IMC:
- ACC- Access to Care and Continuity of Care
- PER- Patient and Family Rights
- AOP- Assessment Of Patients
- COP-Care of Patients.
- PFE- Patient and Family Education.
- Organization Delivery Standards (ODS).Primary care centre effort to be effective, which will be through obtaining a clear management structure with visible coordination of the healthcare process, which has included the delivery of services using teams. Successful Teamwork could be when they have the information they need from an organisation and a whole patient’s record, which can be in a safe environment with minimized risks for both staff and patients. Staff should have the qualification and talent to supply the healthcare expectations and opportunities to improve as professionals. These conditions create primary care centres where healthcare is optimized with staff support and safety (Joint Commission International, 2010). These are some ODS which have been implemented in IMC:
- QIPS- Quality Improvement and Patient Safety.
- PCI- Prevention and Control of Infections.
- GLD- Governance, Leadership and Direction
- FMS- Facility Management and safety.
- SQE- Safety Qualifications and Education
- MOI- Management of Information
Methodology
The purpose of this section is to clarify and understand how the information and data have collected for this research. To answer the research question, primary and secondary research will be compulsory. Primary research will be obtained via International Medical Centre directors and considering the fact that my practical experience since the establishment of the International Medical Centre in KSA as patients’ affairs representative and as a statistical analyst would be an advantage. In addition, surveys and interviews have been need to show the monthly and yearly evaluation performance of healthcare affairs. It will be passed to samples of patients and IMC members or general members in healthcare public and private sectors. The purpose of patient surveys is to evaluate the performance of general services, medical staff, medical services, interactions with patients and overall evaluation. On the other hand, staff surveys will include information on how to implement the policies and procedures in IMC, and whether or not staffs understand the meaning of the IMC logo. Secondary research will be conducted to obtain information about WHO responsibilities and JCI Accreditation, which has included “patient and family rights (PFR), Assessment of Patients (AOP), Access to care and continuity of care (ACC), Quality Improvement and Patient Safety (QPS), Prevention and Control of Infections (PCI) and Governance, Leadership, and Direction (GLD)”. In addition, acquire the five risk areas, which have been decided as “High 5s Project” and find out benefits of improving quality by JCI and this will be done through secondary research through original websites, journal, textbooks, Medical magazines, and articles.
Limitations and Opportunities
To conduct this research some limitations and opportunities will be encountered. These limitations will be found out within both the primary and secondary research. Through the primary research, the limitations will be in the performance and quality of survey, working time of survey and analysing the answers. Within the secondary research, the limitations would involve the reliability of the information, and the confidentiality of some information. Also, some information, which is acquired, might be outdated.
This research will be an opportunity for SA and non-SA public to understand that International Medical Centre has achieved its international accreditation standards in healthcare facilities with its vision “to pioneer a unique approach of healing the body, mind and soul and applying the best international healthcare standards and pursuing divine ethics”. According to that, IMC has the opportunity to improve its performance and quality.
This research will be an opportunity for me to apply for a PHD degree in Healthcare management program. Therefore, it would be very interesting for me to accumulate as enough information to answer my research question.
Gantt chart
References
Collaborating Centre for Patient Safety Solutions (2010) About US. Web.
Healthbase (2010) jci unveils international essentials of health care quality and patient safety. Web.
International Medical Center (2010) About IMC. Web.
Joint Commission (2010) Facts about Joint Commission International. Web.
Joint Commission International (2010). Web.
Joint Commission International (2010) About JCI . Web.
Joint Commission International (2010) Joint Commission International accreditation standards for primary care centre. Web.
Medical tourism magazine (2010) JCI CORNER The Value of Accreditation. Web.
World Health Organisation (2010). Web.
Appendix 2- Ethics Form
Please complete this form by ‘tabbing’ your way through each answer box using a word processor. Save a copy of the completed form entitled as follows – ‘Family Name, Ethics’. Return the completed form as per instructions
- For official use only
- Protocol Number
- Date emailed to student
University of Hertfordshire
Business School
Application for Ethics Approval for Research – tick as appropriate:
Section A. This Section Should Be Completed by All Appicants.
A1 Details:
- Name of Applicant: JAWAHIR MOHAMMED EID BOGIS
- Student Number (if appropriate): 08189239
- UH Email address: [email protected]
- Programme (if appropriate): Msc International Business
- Name of Academic Supervisor: Carol Holder
- Proposed research title: Joint Commission International (JCI) Accreditation standards for healthcare facilities development
- Reasons for research I would like to do PHD in healthcare Management as well as I have work experience in healthcare sector.
- If other please explain.
A2 Primary or Secondary Research?
- Primary research involves gathering new information from interviews, observation or questionnaires. This includes research done face-to-face, by telephone or email.
- Secondary research involves using publicly available information that has already been collected by other people, organisations or academics.
Is your research to be based solely on secondary information? NO
If the answer to A3 above is YES, proceed to SECTION C. and certify the declaration. If the answer is NO, complete the rest of the application, and then certify the declaration.
Note: If you are a student on the DMan programme, intend doing action research or research that involves participant observation then Ethics Form B should be completed. This can be obtained from Ruth Grillo in the administration office ([email protected]).
Section B: Only Complete This Section If You Are Conducting Primaryresearch
- B1 Description of Study: Briefly describe the study: The World Health Organization, which has known more universally by its acronym, “WHO” is considered to be the mother organisation in the healthcare sector. WHO has authority to coordinate health within the united nation systems. In addition, it is in control to be able to provide leadership on international health issues, rules standards, health research processes, and policies and procedures (WHO, 2010). Moreover, in 2005 it identified cooperation centres for Patient Safety Solution, which is the Joint Commission and Joint Commission International “JCI” (Collaborating Centre for Patient Safety Solutions, 2010). Since the1990s, JCI has evaluated the quality performance (excluding financial performance) of healthcare facilities outside of the United States,. JCI’s missionextends the Joint Commission via assisting international healthcare organisations, healthcare ministries, public healthcare agencies, and others to advance the performance quality and safety of global patient care for approximately more than 200 hospitals in 80 countries such as, International Medical Centre (IMC) in the Kingdom of Saudi Arabia (KSA). (The joint commission: 2010, joint commission international: 2010).
The Joint Commission International’s mission is “To continuously improve the safety and quality of care in the international community through the provision of education and consultation services and international accreditation and certification”. JCI authority of healthcare facilities, which is responsible for implementing high standards of medical affairs. The IMC’s development was done through the JCI’s supervision that wielded within IMC’s conception, construction and design as well as overseeing medical procedures and facilities. IMC logo is considered to be a tree, which has been made up of five crescents, it symbolizes the body, mind and soul. It will be cared for in order to achieve optimum health, but the lower crescents; which start from the trunk and roots, symbolize international standards and holy ethics, which are essential for the survival of the tree (IMC,2010). - B2 Informed Consent: This is a process whereby a participant voluntarily agrees to willingly participate in a piece of research once they have been fully informed of what it entails and its purpose. The Applicants should give details of the purpose of the research and how long an interview/ questionnaire will take. Further, the participant should be assured of anonymity and informed that they can withdraw at any time. These details can be given by letter. In the case of questionnaires, telephone interviews or focus groups a verbal explanation can be given, but MUST be supported by written information about the project that is offered to participants. Written information must be available for participants in research via the internet. Additional Guidelines for Ethics includes a specimen letter that should be used. Hard copy may be used or an electronic attachment in the case of email questionnaire s.
B2 (I) Applicants Declaration:
I confirm that I have read and understand the instructions above on informed consent. YES
I agree that written information will be available for all participants and that verbal or written consent will be obtained from all participants. YES
Please note that this written permission MUST BE included in the final copy of your report
- B3 Participants: Selection and Approach: B3 (i) Complete the table
Please note that you are not required to use all of these methodological approaches – you need to discuss with your supervisor and select that approach/s which will be most appropriate to your research. Think carefully here about such issues as: how many questionnaires constitute viable research? How easy will it be to identify informants? How will you obtain email addresses/telephone numbers? Do not assume that people or organisations will hand over customer lists or be willing to see you at your convenience!
B3 (ii)How will your respondent be selected?
B3 (iii)Where will your research take place?
Please note that sections B3(ii) and B3(iii) should reflect section B3(i) – if you have selected more than one methodology then it should be clear how informants will be selected in each case, and where the research will take place.
- B4 Research in Organisations:
B4 (i) Do you intend conducting research in: private firms, public sector organisations, charities or NGOs? Yes
If yes, you MUST complete B4(ii)
If NO, proceed to B5
B4 (ii) If known, give the name of the organisation(s) in which you will be conducting your research.
B4 (iii) If the organisation(s) in which you will be conducting your research is not yet known please explain how you will find and select your sample.
Be careful about research that involves assessing individual’s work within an organisation: this can present problems, as they can worry that results can be fed back to their employers or that it may affect their standing.
Applicants Declarations
B4 (iv) I agree to get written permission from an appropriate senior manager if I intend collecting data from employees in any organisation. YES
Written permission MUST be obtained even if the owner/manager/director of the company is a friend or relative and this written permission must be included as an appendix in your final report.
B4 (v)I agree that it will be made clear to employees in an organisation that their participation is voluntary. YES
- B5 Minors and Vulnerable Groups:
You are advised not to include minors (under 18 years) and/or members of other vulnerable groups in your research. A clear definition of vulnerable groups is difficult: minors are an obvious example, but in some cases groups are vulnerable because of their situation, not because they are vulnerable per se. So, for example, migrant workers, not in their home countries, would be vulnerable; workers who are possibly in a country illegally would be vulnerable; people living in one country, who are encouraged to express political or social views at odds with their home government, could be vulnerable.
There may also be a problem with possible coercion. So, for example, if one of your family members runs an organisation, including their employees in the research must be very carefully handled as they may perceive that they are being coerced or pressured to take part, and will then provide answers which they think the researcher/manager wants to hear.
ANYTHING TO DO WITHE STRESSS OR THE HEALTH SERVICE IS IFFY!!!!
We appreciate that some of the sensitivities we have outlined may be less important in other countries, and that different ethical standards and codes of behaviour apply. Nonetheless, you are carrying out research as a student of the University of Hertfordshire and, as such, your research must abide by the ethical guidelines set out by the University.
Do you intend including minors and/or member of other vulnerable groups? NO
Please be aware that if the answer is YES you will be required to present a justification report to the Ethics Committee. Your supervisor may be asked to attend for that item of business.
- B6 Anonymity:
The anonymity of Respondents anonymity must be preserved. This involves not only withholding their names and addresses, but also other information provided by or about them which could in practice identify them (for example, their company and job title) must be safeguarded.
Do you agree to preserve the anonymity of participants both individuals and organisations? YES
Even if informants appear happy for their identity to be known, you should still ensure confidentiality.
If the answer is NO, discuss with your supervisor and detail reasons:
- B7 Access to Data:
I agree that access to the data gathered and final report will only be made available to the University, participants, participating organisation(s) or client(s). YES
I understand that information gathered or the final report should only be used for academic purposes and should not be used for commercial purposes without the express permission of the client or your academic supervisor. YES
- B8 Confidentiality:
Your research will be confidential in exceptional circumstances. Some firms or organisations may make this a precondition of allowing access. Research that is confidential will contain sensitive information, which will mean that there can be only limited access to the results. This must be discussed with your supervisor.
Confidentiality should not be confused with anonymity.
The rights of facilitators or sponsors to be consulted before publication should be respected. However, researchers should not accept contractual conditions that are contingent upon a particular outcome from a proposed inquiry.
Can you confirm that your research will not be considered confidential as defined above? YES
If NO, please detail the reasons. This MUST be discussed in detail with your supervisor and may delay allocation of an Ethics number
- B9 Studies Undertaken without an Approved Protocol: UPR AS/A12 states that;
‘Any employee of the University who acts in contravention of these regulations will normally be subject to the University’s disciplinary procedures. Any student acting in contravention of these regulations may be penalised by having his or her programmes of study declared invalid and may not be permitted to graduate or may have his or her award revoked’.
I have read the UPR above and understand the implications of undertaking studies without approved protocol. YES
Date: August 27, 2010
Amended: 10th January 2011
Section C. Signatures and Declarations (This Section Should Be Completed by All Applicants)
- C1 Applicant’s Declarations:
I understand that my research should not proceed until my application has been approved and a protocol number received YES
Date: August 27, 2010
I undertake to inform my supervisor at every stage of the research and to gain approval for each part of the research process (introductory letter/ questionnaire /interview design) and that I have read and will abide by the ethical guidelines of the University of Hertfordshire.
YES Date: August 27, 2010
I understand that Ethics protocol is given for a specific research project and methodology as detailed in this Ethics Form and that if I want to change my project or methodology then a reapplication for Ethics protocol must be made. YES Date: August 27, 2010
Amended: 10th January 2011
Students or employees failing to get new approval may be subject to the procedures in UPR AS/A12 (see B9).
- C2 Host Organisation Supervisor’s Declaration (Mainly Applicable for Placement Students):
- Name of host organisation supervisor:
- Position:
- Signature (or attach an email):
NOW RETURN THE FORM AS PER INSTRUCTIONS.
- C3 Ethics Committee Decision (Please Circle):
- Accepted
- Accepted with conditions (see below)
- Referred (see below)
- Signed on behalf of the Ethics Committee:
- Date:
C3 (i) ETHICS COMMITTEE COMMENTS
C3 (ii) The applicant has read and accepted the conditions as laid out above:
Signature: Date:
PLEASE NOTE: The Ethics Committee are only concerned with ensuring that your proposed research meets university-required ethical standards. This approval does NOT imply that your methodology is appropriate or suitable for the proposed research.
Appendix 3- Activity Schedule
Key sections in the dissertation:
- Abstract
- Introduction (approx. 10%).
- Literature review (approx. 25%).
- Methodology (approx. 15% -20%).
- Findings and results (approx. 10% -15%).
- Analysis & Discussion (approx. 15% -20%).
- Conclusions& Recommendations (approx. 10% -15).
Appendix 4– Approval letter
Business School
Dear participant,
I am a postgraduate student in the Business School at the University ofHertfordshire. As a part of accomplishing my MSc degree in International Business, I am required to write a dissertation. Therefore, I am conducting an exploratory study on the implementation of Joint Commission International (IMC) in Saudi hospitals. I am intending to follow the qualitative research and to use structured telephonic interviews in the data collection. The interview duration will be from 15 to 20 minutes.
Therefore, will you be able to participate in this study? Your effort will appreciate.
Please reply whether you would like to take place in this study or not. The questions below are the interview question. Please read through to familiarise yourself with them in case you decided to respond. I am looking forward to hear from you as soon as possible.
Sincerely yours,
Note did have written in this letter: Telephonic interviews and research questionnaire have the same questions.
Appendix 5- Questionnaire
- Q1. What are your objectives for adopting JCI accreditation standards?
- Q3: TQM has a wide image; its issue have related to inspection, audit and punishment. Do you think that JCI accreditation standards can be effective tool to implement the quality in the culture of Saudi hospitals? Why?
- Q4: What is the effect of leadership, teamwork, and beliefs of the benefits of the change on quality in Saudi hospitals?
- Q5: Are there any indicators, which show that Saudi hospitals have implemented JCI accreditation standards? If so, what are they?
- Q6: From your experience, do you expect the implementation of JCI to remain stable in the present? Why?
Appendix 5 – Health Resources Indicators
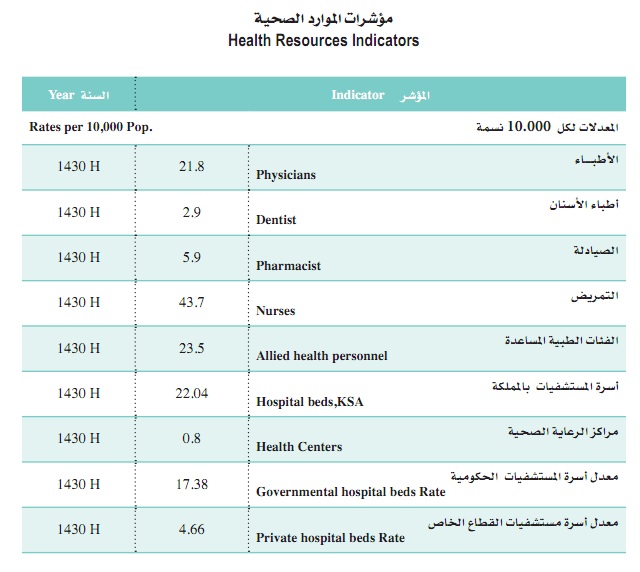
Appendix 6- Joint Commission Organisation