Population and Sampling
Veterans of military service, especially those with a history of deployment in combat-intensive areas of operations, are considered a vulnerable population in a variety of ways. Failure to readjust back into civil society, memories of violence and death-related experiences, survivor’s guilt, and various other psychological stressors often lead to the development of depression and other mental disorders that negatively affect their lives. In the US, the veteran population amounts to 20.4 million people, constituting 10% of the entire adult population, making it a significant population subgroup (Bialik, 2017). At the same time, the periods during which veterans are considered most vulnerable are considered unknown. The variables affecting the likelihood and severity of depression of veterans about their service also remain relatively understudied. The purpose of this research is to analyze the incidence of mental disease in veterans in correlation to their deployment and discharge patterns.
The research will use a stratified sampling method within the target population subgroup. According to Chow, Shao, Wang, and Lokhnygina (2017), this technique is useful to ensure equal representation of each subdivision of the target population group, which is required to answer the research questions and investigate the hypotheses proposed in the scope of the study. It improves accuracy, representativeness, and reduces bias, which helps ensure the validity and reliability of the results. Inclusion and exclusion criteria for participation are as follows:
- The participant must be a military veteran;
- The participant must have served during the last 20 years;
- The participant must have been deployed in a combat role in areas of active military conflict (Iraq, Afghanistan, etc.);
- The participant must agree to take part in the research.
Any individual that does not meet all 4 criteria would not be eligible for participation in this study.
To screen the population for potential participants, it would be possible to enlist the assistance of local veteran populations and healthcare/social care centers, to encourage individuals to approach. These organizations may also provide the researchers with information on how to contact potential candidates eligible for the study. The participants will be briefed two times: the first time during the signing of the consent form, and the second time during the test process. The research does not need a particular setting, as the tests would be filled by the participants in the comforts of their homes and delivered to the researchers as physical or online correspondence. The patient’s privacy and anonymity will be protected through the use of anonymous questionnaires. Preliminary data and all hardware containing it would be physically destroyed after the results are disseminated.
Instrumentation
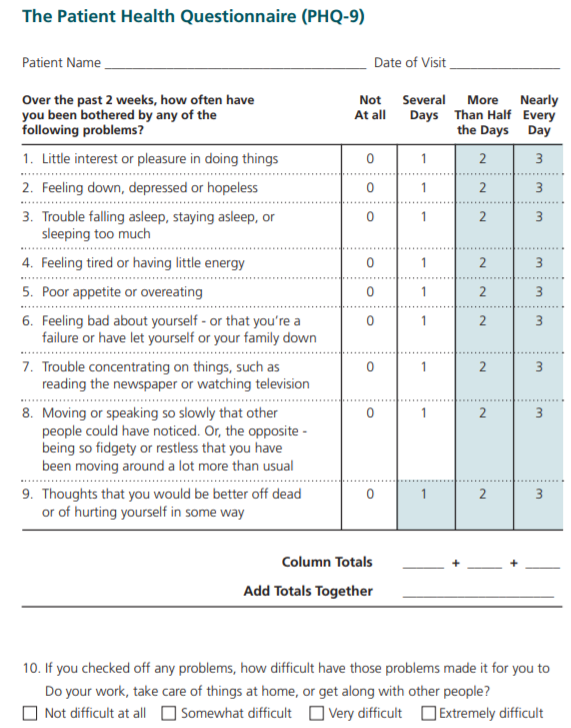
The primary assessment instrument to be used in this study would be the Patient Health Questionnaire Form 9 (PHQ-9). It is a multipurpose instrument for screening, diagnosing, and evaluating the severity of depression in a patient (Zhang et al., 2013). The instrument is free to use and adheres to DSM-IV criteria for major depressive disorders, meaning that there is no need to request permission for its implementation in the proposed study (Zhang et al., 2013). The reliability of this instrument was determined using a test-retest method. The instrument has content validity, construct validity, and discriminative validity well-established for itself. The test-retest reliability values for PHQ-9 are at 0.873, which is good, whereas the validity scores show the average sensitivity of 0.77 and specificity of 0.94 (Zhang et al., 2013).
PHQ-9 is fully supported by a large body of literature and is widely popular in depression-related studies. Zhang et al. (2013) state that PHQ-9 is a useful tool to be implemented in populations where the probability of developing depression-related disorders is high. It is quick, easy to use, and not difficult to understand by the patients, reducing the chances of wrongful implementation or misinterpretation on the part of the participants (Zhang et al., 2013). There is a potential to improve the clinical utility of the existing PHQ-9 questionnaire by increasing the severity score from 4 to 10 or higher, to represent the variance between populations more accurately. Some of the sample questions are as follows (See Fig. 1):
Over the past two weeks, have you been bothered by one or more of the following problems?
- Little interest or pleasure in doing things.
- Feeling down, depressed, or hopeless.
- Trouble falling asleep, staying asleep, or sleeping too much.
The instrument provides ordinal data and is consistent with the operational definition of the variable under investigation, which is the presence and severity of depression, as it was specifically created to measure this variable in patients.
Procedures
This research will follow a descriptive design, which would assess the current status of a variable or phenomenon. This type of approach does not start with a research hypothesis but develops one during data collection and assessment. However, it is possible to create a potential hypothesis by reviewing and analyzing the literature on the subject. Alexander et al. (2016) utilized the same design to evaluate the prevalence of sleeping disorders in veterans with a history of deployment between 2000 and 2010. As it is a descriptive study, no treatment protocols are included. The main dependent variable for the study would be the severity of depression, measured by the PHQ-9 tool, while the independent variables would constitute gender, place of deployment, length of deployment, and time passed since discharge from the armed forces.
The control group will include a randomized sample of military veterans who were not deployed in combat roles and did not serve in active theaters of war. These controls would improve the external validity of the study by providing a point of comparison for the results. The data would be collected during the 3 months between August and October 2019. It should be enough time to contact all of the associated organizations, recruit their help, reach out to potential participants, and receive their feedback on the subject.
Analysis
The data will be collected by distributing questionnaires in paper or online to all interested participants of the test group and the control group. Aside from the PHQ-9 tool, which would be used to collect depression-related ordinal data, the questionnaire would also include the date of enlistment, location, role, duration of service, and the date of discharge. The participants would not be requested to provide their names to preserve their anonymity. Ratios will be generated by converting and disseminating ordinal data received from the questionnaire and aligning it against other variables, to determine the relationship between these items and the severity of depression among the participants.
Statistical data will be generated using the Student’s T-test, which is one of the most popular tools in inferential statistical analysis. It would enable comparing the difference between the test group and the control group as well as the results between different clusters within the test group. The results of the analysis will show whether there is a correlation between the length of deployment, the intensity of deployment, and time passed since discharge, and the severity of depression. The prevalence of depression among the two groups will also be tested. Based on the results of the analysis, it would be possible to generate a working hypothesis. The initial hypothesis for this study could be based on the available data on the prevalence of depression among veterans.
Recent research shows that depression and its severity are more likely to be increased in individuals with lengthy periods of operational deployment as well as in recently-discharged veterans (Thomas et al., 2015). Prolonged combat fatigue and stress may result in greater chances of developing depression, whereas the inability to quickly transition from military to civilian life also poses a significant risk for the veteran population. Therefore, the initial hypothesis is as follows:
- The length and circumstances of combat deployment and the time passed since discharge are the primary factors to affect the likelihood and severity of depression.
- Null hypothesis: The length and circumstances of combat deployment and the time passed since discharge do not affect the likelihood and severity of depression.
Based on the results of the data collection process, this hypothesis may be changed to correctly reflect and represent the findings. The reviewed version would then be proven or disproven using the statistical analysis of the retrieved data.
References
- Alexander, M., Ray, M. A., Hébert, J. R., Youngstedt, S. D., Zhang, H., Steck, S. E.,
- … & Burch, J. B. (2016). The national veteran sleep disorder study: Descriptive epidemiology and secular trends, 2000–2010. Sleep, 39(7), 1399-1410.
- Bialik, K. (2017). The changing face of American veteran population. Web.
- Chow, S. C., Shao, J., Wang, H., & Lokhnygina, Y. (2017). Sample size calculations in clinical research (3rd ed.). Boca Raton, FL: Chapman and Hall/CRC.
- The patient health questionnaire (PHQ-9) – Overview. (1999). Web.
- Thomas, K. H., Turner, L. W., Kaufman, E. M., Paschal, A., Knowlden, A. P., Birch,
- D. A., & Leeper, J. D. (2015). Predictors of depression diagnoses and symptoms in veterans: Results from a national survey. Military Behavioral Health, 3(4), 255-265.
- Zhang, Y. L., Liang, W., Chen, Z. M., Zhang, H. M., Zhang, J. H., Weng, X. Q.,… &
- Zhang, Y. L. (2013). Validity and reliability of Patient Health Questionnaire‐9 and Patient Health Questionnaire‐2 to screen for depression among college students in China. Asia‐Pacific Psychiatry, 5(4), 268-275.
Appendix A