History of the Governance Crises at Mid Staffs NHS Trust
The governance crises at Mid Staffs started as early as 2004. It started when HCC embarked on the first enquiry. The enquiry revealed that intractable and longstanding problems were very evident at Mid Staffs. The new senior management team at the organisation, comprising of the chair and chief executive, was introduced in 2004 and 2005, respectively. The new team held the position that Mid Staffs was in a state of chaos (Francis 2013).
In 2004, Mid Staffs Trust lost the star rating it had held for a long time. The rating resulted from a review by the Commission for Health Improvement [CHI] (Francis 2013). The Trust went from a three star to a two star. The drop in rating was brought about by a number of factors. According to Francis (2013), reasons behind loss of rating are usually adverse. The factors, for instance, include failure to meet the set targets. Others include increased outpatient and cancer waiting times. Other issues entailed poor financial performance and elective surgery in the organisation.
The first report of an enquiry to the activities of the firm was published in 2010. It contained negative criticism with regards to the care and other services offered by the Trust (Francis 2013). For instance, the report revealed that various departments and wards in the Trust lacked to provide proper basic care. In addition, there was a culture that was not conducive for the provision of good health care. There was also the issue of the failure to foster and create an enabling working environment in the Trust.
According to Francis (2013), the environment of the Trust instilled fear among care seekers. The fear was instilled in relation to negative repercussions associated with the services offered at the Trust. A lot of priority was also accorded to the achievement of tasks. To this end, the consultant body disassociated itself from the management. The employees at Mid Staffs lacked morale in their work. As a result, poor standards in the Trust were not openly accepted. Ultimately, internal and external transparency lacked in Mid Staffs Trust. The transparency was associated with the problems that existed in the organisation.
Issues Surrounding Governance and Leadership at Mid Staffs NHS Trust
The problems in Mid Staffs NHS Trust were founded on the shortcomings in relation to governance and leadership within and outside the Trust. Apparently, the various stakeholders had in one way or another neglected their duties, roles, and mandates. As a result, the quality and level of care provided in Mid Staffs NHS Trust went from better to worse. According to Francis (2013), the basis of the poor performance in Mid Staffs NHS Trust included negative culture in the organisation. The other problems included professional disengagement, poor governance, and failure to listen to the clients, including the patients. In addition, there was lack of focus in relation to service standards on the part of the firm. Other problems included inadequate risk assessment relating to reduction of members of staff, wrong priorities, and poor nursing standards (Francis 2013).
Poor governance formed one of the key basis upon which the problems in Mid Staffs NHS Trust were founded. According to Francis (2013), the board of the Trust failed in managing accountability as well as the governance structure during the period of the shortcomings. Apparently, the incoming leadership of the organisation, especially the chair and chief executive failed to address the shortcomings in the operations of the Trust their commencement of their tenure. The executives joined the organisation in 2004 and 2005, respectively (Francis 2013).
According to Francis (2013), the importance as well as acceptance of clinical governance in Stafford failed to permeate effectively. Consequently, the Trust did not have an effectively functioning system by 2014. The description of the governance of the clinic ended up being described as vestigial during the period of the enquiry. The state of clinical governance hence meant that the leadership of the Trust exhibited apparent blindness to the various concerns which lead to an investigation.
Foster and Jonker (2005) view leadership as the incremental influence above and over the mechanical compliance on which the regular and routine direction of an organisation is based. The governance of Mid Staffs NHS Trust failed repeatedly in their leadership role. Apparently, leadership can be viewed together with organisational change. However, in spite of the introduction of the new clinical governance team, the operations and conditions in the Trust continued to deteriorate.
The stakeholder theory essentially conceptualises the firm as consisting of series of groups, exhibiting differing respective relationships in relation to the organisation (Magness 2008). Stakeholders thus consist of the internal organisational members, consisting of employees, board members managers, and external members. The external members include for instance customers, owners, competitors, and suppliers. Hybrid members such as those engaging in inter-organisational cooperatives activities with the organisation also constitute stakeholders (Savitz & Weber 2006).
The primary focus of the stakeholder theory entails the ethical principles guiding the management (Foster & Jonker 2005). However, Rowley and Berman (2000) argue that normative concerns are also very necessary, but insufficient as a criteria for addressing the interests of the stakeholders. Stakeholders, such as those of Mid Staffs NHS Trust, have the potential of either influencing or affecting an organisation. Consequently, their influence on the organisation through deeds or words, through covert signals or overt protests has the ability to hurt or help the ability of the firm in creating value (Phillips 2003).
According to Francis (2013), some of the key issues in the leadership and governance of Mid Staffs HNS Trust was the prevailing negative culture. Apparently, there were significant warning signs with regard to the shortcomings in the organisation. However, the wider system failed to react to them, which can be attributed to poor governance and leadership. Information was available especially in terms of complaints from those receiving care, a factor which should have raised much concern (Tashman & Raelin 2013).
The clinical governance had the most close and clear responsibility for ensuring that the patients were provided with good and safe standard of care. The responsibility essentially fell onto the closest internal stakeholders, namely the board and the other leaders of the Trust. The leadership however failed in appreciating the enormity of the happenings in the organisation (Francis 2013). In addition, whenever they reacted, they did it very slowly, if at all they reacted. Consequently, the significance of some of the matters raised led to their being downplayed.
Francis (2013) attributes this failure in the part of Mid Staffs NHS Trust leadership as emanating from a culture of tolerating poor standards which persisted in the organisation. The leadership and governance apparently focused on financial targets. Consequently, the most important aspect or requirement of the main stakeholders (patients) which is quality service was neglected. The culture of the Trust is actually described as that of self promotion, as opposed to openness and critical analysis (Francis 2013). Reinforcement to these claims is provided in the manner with which the Trust applied for foundation trust (FT). The Trust also sought after Hospital Standardised Mortality Ratios (HSMRs), as well as inaccurately self declared its own performance. The Trust not only sought assurance from false good news, but also tolerated, or explained away any bad news (Francis 2013).
The propagation of the negative culture in Mid Staffs NHS Trust could not have persisted for so long without the direct participation, or indirect involvement of the governance. According to Harrison and Wicks (2013), in keeping with the theory of leadership, the stakeholders’ model of organisational leadership uses the leader effectiveness. The effectiveness of the leaders is as applied as the dependent variable (Phillips, Freeman & Wicks 2003; Schneider 2002). The effectiveness of leaders is defined as entailing the collective sense of the efficacy of the management team. It is based on the perceptions of the multiple stakeholders.
MacGillivray, Begley and Zadek (2007) argue that it is difficult for leaders to garner reputational effectiveness from multiple constituents concurrently. Consequently, using the criterion as a test of the leaders’ effectiveness proves to be critical. Effectiveness reflects on the stakeholders’ broad assessment of the complete leaders’ performance from the various quarters. The leaders of Mid Staffs NHS can however having lacked in effectiveness, based on the duration over which poor performance persisted in the organisation. Ingley and Walt (2004) postulate that the relationship leaders have with others in the organisation immensely influences the level of their effectiveness. The relationship between Mid Staffs HNS employees and the internal stakeholders essentially indicates complacency and ineffectiveness.
Francis (2013) advances that the leadership and governance of Mid Staffs HNS Trust had the shortcoming of not listening to patients. The management of Mid Staffs HNS lacked in development of a culture as well as structures and processes for dealing with patient complaints, and untoward behaviour (Goffee & Jones 2001). Apart from lacking in awareness regarding the nature of care accorded to patients, patient and staff surveys indicated increasing dissatisfaction with regard to running of the Trust (Francis 2013). The Trust’s management also lacked in following up on cases which were brought to their attention.
The failure of Mid Staffs HNS Trust to respond to the various warnings regarding poor care could be attributed to various factors. The management for instance must have been inattentive, or otherwise dismissed the sources of this information as not important. The lack of action can also be attributed to sheer irresponsibility. According to Maak (2007), truly responsible leadership should incorporate strategic use of corporate social responsibility, as well as leaders’ leverage in instrumentally benefitting the stakeholders. On their part, Harrison and Wicks (2013) postulate that responsible leadership has to involve multiple stakeholder groups, in making decisions so as to support long-term sustainability of the organisation. Despite of the two differing perspectives of responsible leadership, Mid Staff HNS Trust failed in both aspects. The Trust’s leadership failed in involving key stakeholders during decision making, and leveraging their actions with CSR for the long-term sustainability of the firm. If the leadership of the Trust had considered these aspects of responsible leadership, the persisting poor performance could have been avoided (Gilbert & Rasche 2007).
The other leadership and governance issues affecting Mid Staffs HNS Trust was professional disengagement (Francis 2013). Apparently, the consultants of the Trust were in the forefront in advocating and facilitating change. The findings of the enquiries carried on the Trust showed that the clinicians were indifferent in matters of change management, a critical role among their various functions. According to Francis (2013), the management was passive when it came to matters of handling personnel issues. Such an approach does not auger well with the management of sensitive matters affecting the patients. A collective responsibility approach in handling patients at all levels of the organisations was lacking.
According to Doh and Stumpf (2005), leadership in organisations exists due to the changing environmental conditions which affect the institution. In addition, leadership also stems from the incompleteness of organisational designs. Barney (2011) echoes this fact by stating that leadership is needed not only to respond to the changing environmental needs, but also to fill the gaps resulting from collapse of the organisational structure. The Trust essentially suffered from a collapse structure, considering that the governance had not responded to shortcomings of the institution such as poor service delivery for such a long time.
Responsible leaders have the ability to influence multiple level analyses within and around the organisations they lead. According to Kaufmann, Kraay, and Mastruzzi (2006), a responsible leadership approach which exhibits more inclusivity in relation to the diverse stakeholder groups has higher likelihood of psychologically resonating at the individual level. Consequently, the approach results in higher engagement levels, at the various levels of the organisation. Responsible leadership has a more stakeholder oriented approach, which is more effective particularly in motivating as well as influencing employees psychologically (Hausman & McPherson 2006; Kaptein & Tulder 2003).
The leadership in Mid Staffs HNS Trust not only lacks in being inclusive in relation to all stakeholder needs, but also does not empower the employees. Gilbert and Rasche (2007) define empowering leadership as a management style that is inclusive and encouraging to the various stakeholder needs. Consequently, responsible leadership can be envisioned as meaningfully trying to engage the various stakeholders within and outside the organisation. An example by Goffee and Jones (2001) is whereby empowering leadership establishes conditions that foster employee’s engagement with their work. The engagement is perhaps as a result of delineating job significance, providing decision-making autonomy, expression of confidence in employee’s capabilities, hence removing performance barriers (Doh & Stumpf 2005; Cragg 2002).
The leadership and governance in Mid Staffs HNS Trust lacked in these factors, hence the various shortcomings. Perhaps the organisation requires such a form of approach, which can create an environment that is conducive for psychological respect and trust. Upon such a foundation, the leadership of the Trust can as well have easily identified and responded to the concerns of the various stakeholders promptly and effectively.
Poor nursing standards and lack of focus on the appropriate standards of services facilitated poor leadership and governance in Mid Staffs HNS Trust. Francis (2013) advances that poor leadership coupled with staffing policies led to the substandard services offered by the nurses in the Trust. Poor leadership, recruitment and staffing led to the inadequate levels of staffing the Trust, leading to the ultimate poor services offered therein. Lack of professionalism and tolerance to poor standards led to the nurses’ failure in reporting the various irregular incidents, and low morale in how they conducted their duties. Poor governance however facilitated the continuity or persistence of the unprofessional behaviour by some of the clinicians working in the Trust (Francis 2013).
The various issues affecting the leadership and governance in Mid Staff NHS Trust not only reflect a management structure which is collapsing, but also lack of stakeholder salience. Bitektine (2011) provides a working conceptualisation of stakeholder’s salience. Bitektine (2011) regards it as the extent to which the management must identify and manage stakeholders’ claims. The governance and leadership of Mid Staffs NHS Trust had failed in all aspects. In line with the concept of stakeholders’ salience, the managers and the other stakeholders codetermine a number of factors. They include views on legality, authority, and importance of claims at the various levels of the organisation (Brown & Trevino 2006). Cameron, Quinn, Degraff, and Thakor (2006) argue that the welfare of prominent stakeholders is associated with the contracts signed with them.
The managers thus have the duty of not only carrying their core functions or planning, organising, directing and control, but also offering leadership. The management has the responsibility of identifying essential stakeholders’ interests to the organisation and prioritising them. The prioritising is done in a specific manner. It should address the interests identified in the contract (Asher, Mahoney & Mahoney 2005; Tashman & Raelin 2013). This should have been so in Mid Staffs NHS Trust, however the poor leadership and governance therein prevented the same. Through stakeholder identification and prioritisation, the managers can prioritise the set of values across the nexus of contracts entered with, especially considering these are patients who need good and safe care.
Recommendations for Development of Governance and Leadership in Mid Staffs HNS Trust
According to Doh and Quigley (2014), the construct of responsible governance and leadership is gaining considerable traction in the scholarship of contemporary management. The case study reveals that persistence of poor standards of service in Mid Staffs NHS stem from ineffective leadership and governance. The proposed solution in the Trust is development of a responsible governance and leadership structure. Responsible leadership provides a very attractive, as well as potentially useful approach of addressing stakeholders’ concerns in all forms of organisations (Ancona et al. 2007; Fehr & Gachter 2000; Freeman, Wicks & Parmar 2004). The approach effectively integrates social responsibility, stakeholders’ empowerment and research in leadership to address governance and leadership.
Figure 1 below provides a model of responsible leadership, pathways, as well as outcomes from the proposed approach to issues in Mid Staffs HNS Trust:
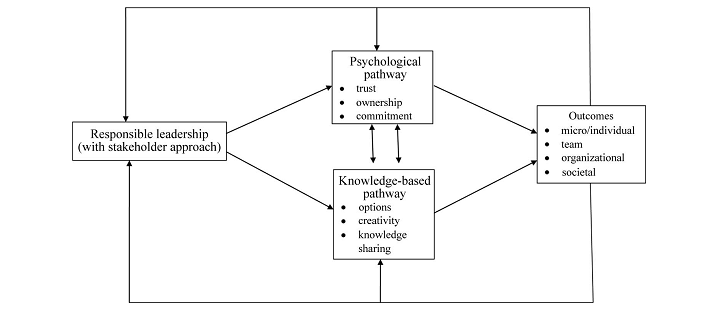
The proposed model integrates both responsible leadership and a stakeholder orientation to governing of organisations. According to Hendry (2001), the model’s capability is made apparent at four distinct levels of the organisation. The levels include the micro/individual, organisational, team and societal. At the individual level, responsible leaders consider their followers as very essential stakeholders. Consequently, they are able to leverage their unique perspective in generating both creativity and motivation (Bosse, Phillips & Harrison 2009; Hillman & Klein 2001).
At the level of a team, responsible leaders consider, as well as encourage various perspectives in their approach to stakeholders. Consequently, this has the capability of leading to team-level psychological learning and safety, both of which are linked to performance in teams (Fehr & Gachter 2000).In addition, these factors are also linked to accuracy and improved decision making (Bosse et al. 2009). At the organisational level, the leaders applying stakeholders’ approach might help in creating and building open, diverse and inclusive internal culture (Ancona et al. 2007). They are attained through sharing as well as dissemination of knowledge while facilitating strong links with the external stakeholders. All these have the capacity of leading to growth of an organisation, innovation, and ultimately performance (Asher et al. 2005). At the level of the society, responsible leaders consistently apply the stakeholder’s approach in bettering management throughout the various cultural boundaries (Doh & Stumpf 2005). In addition, they are able to identify, as well as anticipate the environmental changes, societal issues and problems, hence responding to them in the most appropriate manner.
Conclusion
The governance and leadership issues affecting Mid Staffs NHS Trust can be attributed to the poor management of the organisation. The poor management has essentially led to deterioration not only in terms of quality service, but also with regard to the staff competence. The proposed model for addressing these issues combines both the stakeholders’ theory and responsible leadership.
The model can help address the various issues in the organisation since pragmatically, the proposed approaches cut across all aspects of the organisation. For instance, the model does not only propose changes in the organisational culture, but also empowers the various stakeholders therein. The model also offers various pathways through changes in the leadership and governance of this organisation can be attained.
References
Ancona, D, Malone, D, Orlikowski, W & Senge, P 2007, ‘In praise of the incomplete leader’, Harvard Business Review, vol. 85 no. 2, pp. 92-100.
Asher, C, Mahoney, J & Mahoney, T 2005, ‘Towards a property rights foundation for a stakeholder theory of the firm’, Journal of Management and Governance, vol. 9 no. 1, pp. 5-32.
Barney, J 2011, Gaining and sustaining competitive advantage, 4th edn, Pearson Education, Inc: Upper Saddle River, NJ.
Bitektine, A 2011, ‘Towards a theory of social judgments of organisations: the case of legitimacy, reputation, and status’, Academic Journal of Management Review, vol. 36 no. 1, pp. 151-179.
Bosse, D, Phillips, R & Harrison, J 2009, ‘Stakeholders, reciprocity and firm performance’, Strategic Management Journal, vol. 30 no. 1, pp. 447-456.
Brown, M & Trevino, L 2006, ‘Ethical leadership: a review and future directions’, Leadership Quarterly, vol. 17 no. 1, pp. 595-616.
Cameron, K, Quinn, R, Degraff, J & Thakor, A 2006, Competing values leadership, Edward Elgar, Northampton, MA.
Cragg, W 2002, ‘Business ethics and stakeholder theory’, Business Ethics Quarterly, vol. 12, no. 2, pp. 113-142.
Doh, J & Quigley, N 2014, ‘Responsible leadership and stakeholder management: influence pathways and organisational outcomes’, The Academy of Management Perspectives, vol. 28 no. 3, pp. 255-274.
Doh, J & Stumpf, A 2005, Handbook on responsible leadership and governance in global business, Edward Elgar, Northampton, MA.
Fehr, E & Gachter, S 2000, ‘Fairness and retaliation: the economics of reciprocity’, Journal of Economic Perspectives, vol. 14 no. 3, pp. 159-181.
Foster, D & Jonker, J 2005, ‘Stakeholder relationships: the dialogue of engagement’, Corporate Governance, vol. 5, no. 5, pp. 51-57.
Francis, R 2013. Report of the Mid Staffordshire NHS Foundation Trust public inquiry. Crown, U.K. London.
Freeman, R, Wicks, A & Parmar, B 2004, ‘Stakeholder theory and “the corporate objective revisited”’, Organisation Science, vol. 15 no. 2, pp. 364-369.
Gilbert, D & Rasche, A 2007, ‘Discourse ethics and social accountability: the ethics of SA 8000’, Business Ethics Quarterly, vol. 17 no. 2, pp. 187-216.
Goffee, R & Jones, G 2001, ‘Followership’, Harvard Business Review, vol. 79 no. 11, p. 148.
Harrison, J & Wicks, A 2013, ‘Stakeholder theory, value, and firm performance’, Business Ethics Quarterly, vol. 23 no. 1, pp. 97-124.
Hausman, D & McPherson, M 2006, Economic analysis, moral philosophy, and public policy, 2nd edn, Cambridge University Press, New York.
Hendry, J 2001, ‘Missing the target: normative stakeholder theory and the corporate governance debate’, Business Ethics Quarterly, vol. 11 no. 1, pp. 159-176.
Hillman, A & Klein, G 2001, ‘Shareholder value, stakeholder management, and social issues: what’s the bottom line?’, Strategic Management Journal, vol. 22 no. 1, pp. 125-139.
Ingley, C & Walt, N 2004, ‘Corporate governance, institutional investors and conflicts of interest’, Corporate Governance: An International Review, vol. 12 no. 4, pp. 534-551.
Kaptein, M & Tulder, R 2003, ‘Toward effective stakeholder dialogue’, Business and Society Review, vol. 108 no. 2, pp. 203-224.
Kaufmann, D, Kraay, A & Mastruzzi, M 2006, Governance matters V: Governance indicators for 1996-2005, World Bank Institute, Washington, DC.
Maak, T 2007, ‘Responsible leadership, stakeholder engagement, and the emergence of social capital’, Journal of Business Ethics, vol. 74 no. 1, pp. 329-343.
MacGillivray, A, Begley, P & Zadek, S 2007, The state of responsible competitiveness 2007, Accountability, London.
Magness, V 2008, ‘Who are the stakeholders now: an empirical examination of the Mitchell, Agle and Wood theory of stakeholder salience’, Journal of Business Ethics, vol. 83 no. 1, pp. 177-192.
Phillips, R 2003, Stakeholder theory and organizational ethics, San Francisco, Berrett-Koehler Publishers, New York.
Phillips, R, Freeman, R & Wicks, A 2003, ‘What stakeholder theory is not’, Business Ethics Quarterly, vol. 13 no. 1, pp. 479-502.
Rowley, T & Berman, S 2000, ‘A brand-new brand of corporate social performance’, Business and Society, vol. 39 no. 1, pp. 397-418.
Savitz, A & Weber, K 2006, The triple bottom line, Jossey-Bass, San Francisco.
Schneider, M 2002, ‘A stakeholder model of organisational leadership’, Organisation Science, vol. 13 no. 2, pp. 209-220.
Tashman, P & Raelin, J 2013, ‘Who and what really matters to the firm: moving stakeholder salience beyond managerial perceptions’, Business Ethics Quarterly, vol. 23 no. 1, p. 4.