Abstract
“Skill mix as the range of different skills possessed by the members of a group or required for a particular job” (Richards et al., 2000, p. 186). Its role in transferability of skills and knowledge in the community nursing context is highly debated among different stakeholders. While many agree that having differently skilled nurses working together allows transfer of skills, some argue that this method of skills development could erode quality of professionalism.
Proponents further argue that skill mix allows community nurses to accomplish their duties more effectively by having different skills available on site. It further allows better quality of results when nurses with different skills can specialize in the area in which they are good at. It also allows them to train and learn new skills from each other to ensure they stay relevant in the industry. By so doing, they are further able to deliver better quality and perform more duties.
This research proposal will be focused on community nursing and how skill mix allows the development of skills. It will focus on the role of nursing skill mix on transferability of skills and knowledge among registered nurses working in the community nursing context. The area of implementation for the paper is North Batinah Region in Oman. Professional development in this paper will address administering medical services, having proper professional ethics, and being able to execute professional duties in a skilled manner.
This research proposal highlights methods that will be used to collect primary and secondary data. In preparation for that, it analyzes literature on the different aspects surrounding skill mix. These include skill mix and quality, and the role of nursing skill mix in ensuring professional development in the healthcare sector.
The impact of nursing skill mix on professional development
Introduction
Richards et al. (2000, p. 186) defines “skill mix as the range of different skills possessed by the members of a group or required for a particular job”. The role of skill mix in transferability of skills and knowledge has been a source of debate in the healthcare industry for a long time now. “An important potential contribution to the efficient use of the health workforce, is the possibility of ‘skill mix’ changes” (Richardson et al.,1998, p. 120). Some regions agree with this argument and others dispute it. This is evident from the levels of implementation of skill mix initiatives that have taken place in different countries. Among the countries that take skill mix seriously is Russia, Spain, Russia and the United Kingdom.
The role of skill mix in professional development in the community nursing context is driven by different factors and considerations. “There are large differences in reported physician/nurse ratios across OECD countries and evidence of significant changes over time in some countries, which raises the issue of direction of change and desirability” (Bluestone, 2006, p. 211). Changes and strategies utilized further depend of different factors.
As Banham and Conelly (2002, p. 259) explain, “changes implemented in skill-mix may be driven by a variety of motives including service innovation, shortages of particular categories of workers (especially in inner cities or rural areas), quality improvement, and a desire to improve the level of professionalism”.
Professional development in this paper is defined as “skills and knowledge attained for both personal development and career advancement” (Speck and Knipe, 2005, p. 113). In a community or group context, it involves engaging shared learning and having a team that is working towards common objectives. Community nursing on the other hand is “a part of healthcare that works with people and families to help prevent diseases, maintain health and treat any existing health problems by supporting and maintaining patient’s independence, safety and healthy lifestyles” (HealthInsite, 2011, p. 1).
According to Benner (2001, p. 74), “the pursuit of skill mix in the new National Health Services (NHS) has divided managers and healthcare professionals”. If this were to be done in the community nursing sector, the threat of losing quality in the sector would be more real. Such a measure would also lead to the erosion of value for quality. As Blank and Burau (2007, p. 34)explain “trade unions see the spectra of redundancy, while professionals fear the erosion of quality in the sector”. The debate over the issue of skill mix in community nursing continues to heighten and more issues keep arising.
For example, arguments between professional community nurses and other stakeholders over what should be done have resulted in a belief that only community nurses can comprehend the complexity of their skills (Joint Commission on Accreditation of Health Care Organizations, 2005). They therefore argue that they should be allowed to make all the decisions that affect how they implement initiatives such as skill mix and its role in professional development.
According to Borbasi and Gaston (2002, p. 31), “skill-mix changes may involve a variety of developments including enhancements of skills among a particular group of staff substitution between different groups, delegation up and down a uni-disciplinary ladder, and innovation roles”. In the context of community nursing, several simplistic approaches to the issue of skill mix in the past have not done much to allay the confusion and disagreements (Moram, 1999). When skill allocation is in such a way that it only allows nurses to do what they have been trained to do, the possibility of skill redundancy is real (London Department of Health, 2002).
It is for this reason that skill mix initiatives are implemented. Having a group of differently skilled nurses work together allows them to learn from each other, and transfer skills they have perfected in to the rest of the team. Since communities have many changing needs, having nurses whose skills are constantly updated is only possible by having them interact with different skills regularly. As Wrede (2008, p. 128) argues, “at its best, careful consideration of skill mix offers much in terms of aligning services more appropriately to the health needs of local populations”.
Having a team that shares common objectives for the process they are engaged in makes it possible for them to extract skills that are useful in their line of duties from their team mates, and use them to expand their knowledge (Marriner-Tomey, 1993). Chen et al. (2004, p. 1986) adds that “skill transferability is also achievable if a team realizes that skill is a product of ability and experience as well as grade, a point that district wide reviews seem to have failed to grasp”.
Cribb (2005, p. 13) argues that “a culture of long service and low staff turnover of staff exists, which means that skill mix must be developed with existing staff, with room for maneuver only when staff leave”. It is important to realize that skill mix works by ensuring that each staff member has a unique cluster of skills, a very significant factor in the completion and success of various team works. Skill mix can be used as encouragement to have community nurses expand the scope of their skills and knowledge, and develop different styles that suit the current medical needs in communities (Ministry of Social Affairs and Health, 2002). When skills are properly nurtured and developed, it is easier for them to accomplish different duties and monitor them accurately (Shumbusho, et al., 2009).
Statement of the problem
The community nursing sector is today faced with many challenges that make it hard to deliver quality and do it consistently (Parle, Ross and Doe, 2006). Key among these challenges is professional development. There are constant disputes over roles and responsibilities between senior and junior nurses, and other medical professionals, perhaps from the lack of constant initiatives to upgrade skills and adjust roles (American Association of Colleges of Nursing, 2011). The complexity of the community nursing profession makes it hard for governments to intervene wherever professional related challenges arise.
The Gallup Organization (2000, p. 1), “established that nurses had the highest standards of honesty and ethics in that year”. Ten years later, the industry faces major challenges as far as ethics and discipline are concerned. The healthcare industry is faced with challenges that come with the constant changes happening in the industry. More cases of questionable conduct are filed each day and ethical concerns and issues are still evident.
Regulations, policies and expectations from customers may sometimes be hard for community nurses to keep up (Rese et al., 2005). In order to ensure that community nurses still hold that position they held a few years back, it is necessary that they have initiatives and someone to help them constantly update their skills. This paper seeks to understand the role of skill mix in professional development in the context of community nursing.
The survey will be focused on community nursing and how skill mix allows the development of skills. It will focus on the role of nursing skill mix on transferability of skills and knowledge among registered nurses working in the community nursing context. It will study the allocation of different skills to nurses to work in one primary healthcare organization. The area of implementation for the paper is North Batinah Region in Oman. Professional development in this paper will address administering medical services, having proper professional ethics, and being able to execute professional duties in a skilled manner.
Aim
Analyze the impact of nursing skill mix on professional development in community nursing.
Objectives
- Conduct a literature review to evaluate the impact of nursing skill mix on professional development, specifically in community nursing
- To evaluate how skill mix can participate in nursing professional development.
Rationale
This research has specific practical value. Having considered the results, it will be possible to state whether skill mix plays a vital role in nursing professional development. The answers will explain different responsibilities of skill mix and how they contribute to the health care’s development. The influence of skill mix is evident in its role in training, coaching and development.
Skill mix and key issues
As Constable and Russell (1986, p. 24) explain, “it constitutes the professional reward aspect which incorporates processes and procedures for tracking new skills, measuring job values, designing and maintaining results structures, creating performance and ensuring benefits”. However, it is important to note that skill mix management is not just about skill development. It is also about quality performances which boost confidence in the industry, and improve employee’s confidence as well as motivation. Key issues to address in skill mix in the community nursing sector are;
- How to ensure external and internal competitiveness and equity.
- How to reward community nurses as individuals and promote team work as well.
- Which skill mix management processes are appropriate for the community nursing sector.
- How to devolve power and ensure nurses can manage their own skill mix strategies while staying within the sector’s policies.
- How to motivate those community nurses who have reached the highest level of career possible in the sector.
- How to ensure skill mix initiatives translate to improved performance.
- How to structure and design skills evaluation schemes.
- How to ensure community nurses are prepared for both their inputs and outputs.
- How to make community nurses recognize and appreciate skill mix as a positive technique in the healthcare sector.
In today’s scenario, there are various skill mix trends available for the community nursing sector (Rechel and Dubois, 2006). As Armstrong, Duncan and Peter (2010, p. 100) explain “more industries today choose to develop increased awareness of the need to treat job measurement as a process for managing relatives, which, as necessary, has to adapt to new organizational environments and much greater role flexibility”. Others choose skill mix structures that cover every employee regardless of their position. Team pay is a common trend in any industry trying to introduce new initiatives in their sector (Hughes, 2004). Other trends include performance awards and more sensitivity to functional markets to enable the sector retain talented employees.
Literature review
To understand the background of this paper, several books, journals and articles proved extremely resourceful. Statistics in the healthcare sector were sourced from government and non-government databases. The American Association of Colleges of Nursing, through their article about shortages, explain the depth and length of the situation in the sector. One of the biggest challenges facing the industry today is shortages, skill development and changing demands and medical needs. It is also the drive behind many other strategies and initiatives being implemented in the sector. These challenges demand initiatives that will ensure constantly updated skills, well trained and professionally developed community nurses.
To understand transferability of skills and knowledge as a professional development technique, Cheng Wai explains the concept and its applicability in graduates. The author explains that “transfer of skills allows effective and continuous application of skills, knowledge and attitudes that were learnt in different environments by different people” (Cheng, 1998, p. 94). This according to the author increases learning and helps professionals develop their capabilities further. For transferability of skills to work, there has to be different professionals with different skills and capabilities. Skill mix then plays a significant role since it creates this kind of an environment.
Rallings, outlines and explains important and relevant skills for community nurses. The author begins by helping the reader understand the background of community nursing. He explains community nursing as “a unique area of nursing practice that extends the delivery of professional nursing care beyond the walls of hospitals to every conceivable environment in which the recipients of care may be located” (Rallings, 2009, p. 3).
Their skills include collaboration, advocacy, and policy enforcement, among others. Unlike other nurses, community nurses are expected to have skills in surveillance, community organizing, social marketing and outreach. Community nurses play a crucial role in performing disease and other health event investigations. As a result, they are expected to have good investigative and research skills.
McCormack, Kim and Robert discuss how how practitioners can be enabled and supported to initiate and implement development and change. The authors state that “besides the fact that the term ‘practice development’ is poorly understood, there is a constant emphasis on the development of practice in contemporary healthcare” (McCormack, Kim and Robert, 2004, p. 15). As argued by the authors, “staff involved with developing practice need to operate within a framework that recognizes the complexity of bringing about change successfully within different medical sectors” (McCormack, Kim and Robert, 2004, p. 55). This should be the case in community nursing where the people involved need to understand the complexity of skill mix and its role in skills transferability.
McSherry and Jerry, outline the meaning of excellence in practice. According to the authors “core contemporary issues used to illustrate excellence include evidence-based practice, clinical governance, and health and social care standards” (McSherry and Jerry, 2008, p. 113). They outline key topics involved with ensuring quality in the healthcare sector. One of them is national service frameworks which covers areas such as community nursing. Excellence in this area of practice can be achieved through different initiatives such as skill mix, which will allow transferability of skills and knowledge by having differently qualified personnel working together and learning from each other.
In his article, Trautman explains how to support change with knowledge transfer skills. The first steps according to the author include identifying the areas that need change, identifying strategies that are already working and those that are failing, and identifying ways through which information can be moved efficiently. As explained by the author, skill mix supports knowledge transfer through on-boarding new employees, merging different teams together and cross-training professionals.
Skill mix supports transferability of skills and knowledge by allowing nurses with a specialty in different areas to share it with others. They share their skills and knowledge in a specialized way serve as the go-to-person and train many people (new or existing) on the topic they have specialized in (Trautman, n.d). The centrality of the people working together as a team helps them improve consistency and improve potential for every member of the group. Supporting knowledge transfer according to the author includes defining roles and clarifying the expectations of each of the roles performed by the members of the team.
Skill mix creates a set up where each person is able to say where they would be glad to help. Skill mix initiatives further recognize that it is not possible for one to succeed at their job if the rest of the team is not up to speed. Through skill mix, every member of the team is prepared for future leadership roles. Team meeting, schedules and other activities involved in team work are well taught to every member of the team. To improve the team’s success, every nurse would be willing to play their role in ensuring that collective results are good. Instead of working as competitors, nurses will be able to work towards a common goal and enjoy better results.
Bourgueil, Philippe, Julien and Engin (2008, p. 4) explain that if the sector wants to fully reap the benefits of skill mix, “they need to determine what skills are needed to get a job done and then decide who has those skills and the time”. One of the challenges identified by the authors is turf protection. These sentiments are echoed by the The National Pharmacy Association (2010, p. 2) who further argue that “the department of health should determine which services are to be offered in each community as the starting point for determining how many people would be needed, where, and with what sets of skills”. Problem solving methodologies, soft skills for change agents, statistical tools for accomplishing different investigative and research assignments, among others, should be established too.
Fisher explains skill mix in the context of community nursing. The author argues that “at a time when spending in the NHS is under heavy scrutiny, it is very important that all decisions are based on the best evidence and knowledge that works” (Fisher, n.d., p. 300). The author brings together available research on the subject of skill in community nursing and has put it in a professional context to help the reader understand the background of the problem and available solutions. She believes that “skill mix decisions should be led by the clinicians, and evaluated for their clinical effectiveness, not as a cost saving measure” (Kuokkanen and Leino-Kilpi, 2000, p. 238).
Fisher’s work illustrates that the right combination of skills will enhance community nursing outcomes by allowing skills, knowledge and ideas to be transferred and shared among each other. However, the author warns that inappropriate skills substitution will not bear much fruits. Instead, it can lead to more vacancy rates due to a decreased morale. The book discusses delegation and accountability, as well as their roles in ensuring that challenges facing skill mix initiatives are resolved appropriately.
Mashaba in his book takes the reader through nursing education, giving it an international perspective. Part of the book takes a close look at transferable skills in nursing. The author points out that “ making transferable skills explicit in a practice paradigm allows nurses to be aware of the skills so that they can relate to others and identify which aspects of their nurse practice are relevant to other roles or work they wish to take up” (Mashaba, 1994, p. 144).
The book concludes that transferability of skills and knowledge is a critical element of learning. Depending with the settings, transferable skills can be specialized or general skills in the practice such as group work and data handling skills.
Skill mix as applicable in the entire medical profession, especially in nurses, as explained by Banham and Conelly. These authors elaborate on whether skill mix is a substitution or diversification technique. According to the authors, skill mix can be implemented to achieve either of the two. However, using skill mix as a diversification technique serves more benefits than substitution. Diversifying the skills and responsibilities of community nurses allows them to do perform more responsibilities, while being able to deliver in their core responsibilities.
One way through which this happens is skill and knowledge transferability. Instead of substituting a nurse and replace him/her with one who has the desired skills, a team of skilled nurses working together allows them to share and transfer skills to each other, and in the long run, the team is equipped to perform most of the tasks on the ground.
Buchan, in his article on determining skill mix, explains practical guidelines for managers and health professionals. The author provides practical guidelines for professionals considering skill mix as a skills and knowledge transferability technique. The author further offers four major stages in the implementation of skill mix. In the context of community nursing, these stages are driven by several questions including what the sector needs to address by implementing skill mix, what the span of control is for the sector, what resources are available and approaches through which skill mix can be implemented.
The skill mix cycle as explained by the author includes “evaluating the need for change, making change happen by identifying and implementing solutions, identifying the opportunities and barriers for change through a span for control, and finally planning for change through available resources” (Buchan, 2004, p. 6).
These guidelines are further explained by Buchan and Calman (2005, p. 40) who explain that “firstly, there is need to define the currently available skills, in terms of activities, staffing configuration and many other considerations”. Change is not possible if there is no clear direction of the starting and ending point. To successfully implement effective skill mix, there is need to evaluate its effects. There has to be a clearly set and defined baseline indicator.
Factors to consider in this step include activities and roles performed indicators for measuring outcome, the needs of different client groups, quality of care provided and that expected, staff involved, and their availability and capabilities. After these factors have been put into consideration, the authors further explain that “the skills which can be shared and transferred from one nurse to the other need to be assessed” (Buchan and Calman, 2005, p.13). This step involves identifying the most urgent needs and assessing how applicable available solutions are.
When these steps and factors have been considered and undertaken, it is then easy to use skill mix as a way to transfer skills and knowledge within nurses. Identifying the current situation of a team allows them to identify what is lacking and which skills need to introduced. It is through such initiatives that nurses are able to learn and get skills from the rest of the team. The end results is a fully equipped team with capabilities to perform most of the duties, without having to recruit new nurses with specialized skills into the team.
Buchan and Dal Poz review the evidence in the of skill mix in the healthcare workforce by discussing the reasons why it is so important. The authors argue that “for the mix of the nursing staff, increased use of less qualified staff will not be effective in all situations, although in some cases, increased use of care assistants has led to greater organizational effectiveness” (Buchan and Dal Poz, 2002, p. 580). Evidence collected from their research indicates that there is a lot of underutilized avenues for developing the community nursing profession. Mixing different skill mixes in various community programs will allow the sector to explore new roles and skills.
In his book, Benner offers appropriate mechanisms that can be used to help community nurses develop from novices to experts. Perhaps this is the biggest role of skill mix and skill transferability. The book addresses excellence and power in clinical nursing practice. Incentives, recognition, rewards and strict discipline measures are key strategies towards ensuring that nurses deliver, work together, benefit from each others diverse skills, and stay disciplined. When such measures lack, the sector’s efforts to use skill mix as a skill transferability initiative may not be rewarding.
Leadership plays an important role in how skill mix initiatives are implemented, and the role they play in skill and knowledge transferability. To understand leadership and its role in nursing, Borbasi and Gaston explain the concept by categorizing them into different classes.
They classify them into organizational management, creation and vision, communication and strategy. When a leader understands this, he/she is willing to stay in line with the management and follow the hospital’s policies and regulations. As a leader, managers should work on being more visionary and equip themselves with the required strategies. Such qualities will help them direct their teams and services to a better future in the industry. To be an effective leader, they also need to work on their problem-solving skills, which the authors point as a fundamental element of a leader and a mentor.
The need for professional ethics and mentorship is addressed by Constable and Russell who explain the effect of social support and the work environment among nurses. Through an empirical study on 310 nurses at an Army Medical Centre in Colorado, the article points out that burn out is a significant problem among nurses, and needs to be addressed urgently. The results revealed that major determinants of burnout and skills deterioration include lack of motivation, physical discomfort and decreased performance, among others.
This is further discussed by Canham and Joanne in their book on mentorship in community nursing. The book goes further to address the challenges and opportunities in the area. It starts by pointing out that “the importance of the community practice teacher is increasing with the expansion in primary care” (Canham and Joanne, 2002, p.112).
Specialist areas of community practice as outlined by the authors include children’s community health, occupational health nursing, health visiting, and general practice, just to mention a few. Skill mix can be used as a knowledge transfer initiative by having nurses specialized in these areas work together. The results will be community nurses with capabilities to work and serve in any of the specialities mentioned above, and many others such as community nursing mental health.
The authors are supported by Cribb, who in his book addressing health and the good society. The author sets healthcare ethics in social context by explaining the need for professional ethics, guidance and mentorship in the sector. He helps the reader understand mentorship in clinical practice in undergraduate nursing education. The authors argue that this is where mentorship begins in nursing, and should not stop after people have grow their career to senior nurses. The authors explain how important it is to ensure that nursing students have the right perception about nursing even before they begin their careers. Just like students, senior nurses need support and mentorship from managers and other people above them.
Policy instruments that support skill mix can be understood more clearly by reviewing Buchan’s work and other authors that agree with him and support his arguments. According to the author, “skill mix initiatives focus on changing professional roles-directly and indirectly” (Buchan, 2004, p. 22). Nurses change their roles indirectly by modifying the interface between services. They do so directly through delegation, having new types of workers introduced in the profession, change of roles and skills, and introduction of new skills.
The author continues to explain that skill mix initiatives are motivated by various factors. Motivation includes both qualitative and quantitative considerations. Qualitative considerations include professional development, work concerns and quality, as well as quality improvement. Quantitative considerations include the need for cost-effectiveness, shortages and wrong distributions of a workforce.
One of the policy instruments supporting effective implementation of skill mix is “modifying or introducing new professional roles through the development of different organizational and regulatory arrangements, including regulating professional scopes of practice and overcoming institutional barriers” (Cowen and Moorhead 2006, p. 113). Like many other professions, nursing is slowly evolving to meet the current needs of their clients. As this happens, training and skill development is changing to meet the expectation of different stakeholders in the industry.
Another policy supporting skill mix initiatives is “supporting new or enhanced professional roles through collective financing and altered financial incentives” (Dierick-van Deale et al., 2010, p. 30). Cost cutting measures have a significant influence on initiatives implemented in the healthcare industry. Financial incentives put in place have to be able to give considerable returns to the stakeholders. The third policy supporting skill mix is “ensuring the educational foundations (completed and capacity) for the new and expanded professional roles” (Eastaugh, 2004, p. 14).
However, WHO caution that the drive for any initiative as the nursing industry tries to implement skill mix must be must be sensitive to the professionals and to the system (World Health Organization, 2006). As further supported by Harris (2005, p. 234) explains, “across the initiatives, it is essential that the professional organizations affected and the government supports new professional roles”. One size approaches aimed at meeting all the objectives do not work. Specific initiatives must be set to meet specific goals and objectives.
Skill and knowledge transferability as a solution to skill development is explained in details by Bourgeault and Mulvale. Their work is further supported by Buchan who asks the question, ‘if skill mix is the solution, then what is the answer?’. The authors give a background of these problems by explaining that the nursing profession is marred with shortages and imbalances in culture, gender and other social factors.
The number of nurses needed each year to cope with increasing demands for healthcare are far much more than the number of nurses graduating from colleges every year. The US Bureau of Labor statistics support the authors’ arguments by stating that in the United States, the healthcare sector is constantly growing and there had been a creation of more than 37,000 new jobs created in the month of March alone. However, only half of these nurses will be a available to fill up the positions.
Buchan confidently states that skill mix can serve as an initiative to support skills transfer and as a solution to the current situation. Skill mix allows the creation on new responsibilities and roles, by allowing people trained in different professions to interact. Creating new roles and responsibilities also allows nurses to easily delegate their duties amongst themselves, since everyone is equipped with the necessary skills through transferability. As result, there is more delivery of services with the available number of nurses available.
One of the major skill mix initiatives is training and capacity building. Training and capacity development through working together, mixing skills and transferring them to each other allows those under training to undertake more responsibilities and tasks than they did before. Through training, the nursing industry will be able to develop the skills of those in the sector but are not necessarily trained in specific areas of specializations.
To be able to serve more patients today, these will allow nurses to do more than they were initially trained for. For example, nurses who have been trained to take care of patients, do ward rounds and other tasks in a hospital may not have much experience on how to perform complex community nursing duties. By working together with more experienced nurses in the field, the need to go back to school and be trained is reduced. Furthermore, through practice and referring to what the rest of the team is doing, practical skills development is made possible.
However, Bourgeault and Mulvale warn that it is important to realize that forced skill mix will not deliver much. The industry must implement its strategies in consultation with nurses and all the people affected. A sector which has an open communication culture allows employees air their concerns and complains, some of which may be affecting their service delivery. It also allows managers and the executive to relate and connect better with every part of the organization including employees at the lowest level.
Healthy communication between people on all levels is a good way to source information and allow the executives make more informed decision, considering every person’s needs. A sector which adopts a culture of punishment for poor performance may be able to improve its productivity but will not enjoy the loyalty of its employees since they work from fear.
Buchan explains that training and sharing of skills are aimed at preparing individuals to keep their skills updated and ready to undertake higher levels of work when chances arise. It also provides a possibility of performance change. Skill mix allows skill sharing through skill transferability and will help the community nursing sector retain their pool of human resource and stay up-to-date with current and relevant skills in the market. It also makes the nurses feel cared for and they are then motivated to give better quality to their clients.
Bourgeault and Mulvale explain in details the factors influencing the ability to scale up skill mix initiatives. One of them is contextual framework. Cited Dyro’s work in their literature, it is explained that “the contextual factors that enhance or impinge on the scaling up of skill mix initiatives can be divided into three levels: the macro, meso and micro levels” (Dyro, 2004, p. 112). Macro factors cover the influence of regulations and policies that cover practice such as education systems in different regions, professionalism as understood in different regions, and statutory recognition of nursing in that particular region. Economic domains are also part of the macro factors.
Factors at the meso level include those in the local organizations’ level such as institutional arrangements. They include educational systems, organization’s settings and community’s expectations. As cited in the author’s work, Culyer and Newhouse ( 2000, p. 23) explain that, “contextual micro-level factors affect the quality of skill mix initiatives at the level of everyday practice, and include interpersonal relations between the various health professionals and any previous experience they have had with skill mix initiatives”
In view of these considerations, through the development of regulatory changes and organizational arrangements, policy instruments for skill mix will need to allow the introduction of new professional roles. They will have to support the new roles through available and new policies such as collective financing to ensure the whole public is involved. Any policy instrument for a skill mix will also need to ensure that competence and capacity for the new roles are located at the right place.
As summarized by the two authors, contextual factors affecting skill mix initiatives can be broken down into macro, meso and micro as below;
Skill mix may involve creation of completely new skills and responsibilities, or transfer of existing skills from one nurse to the other. It could also involve re-structuring different areas of community nursing to meet different needs other than the existing ones. In many cases, regulatory changes have to be effected to allow a full implementation of skill mix. “The regulation of professional scopes of practice are particularly critical and can either enable or hinder enhancement or substitution opportunities, depending on the accommodation of overlapping costs of practice” (Denny and Earle, 2005, p. 112).
Like every other initiative, skill mix as a professional development technique faces several challenges and hindrances. In countries where skill mix has been pursued to integrate and in-collaborate effective services such as Germany, their biggest challenge still remains the fragmentation of the healthcare system (WHO, 2007). Countries such as Russia, which have pursued skill mix initiatives with high levels of commitment, are still not able to implement it as it should, due to the same challenge and many others. As Coombs (2004, p. 56) explains, “further barriers, which are embedded in the regulatory framework and stakeholder arrangements, include the absence of uniform regulation of provider organizations and poor coordination across the various sectors and occupational groups”.
Further challenges arise from the fact that the community nursing sector is polarized by many associations and funds, a factor that makes it hard for the industry to introduce any new professional groups into the existing teams. Any interventions from external stakeholders are always met with resistance and long processes of consultations. “The regulation and organization of the healthcare are highly physician-centered” (Freeman, 2000, p. 67). Even as states take up more interventionist roles, incentives and policies in the sector continue to be heavily focused on the professional aspect community nursing.
In Spain for example, “many institutional with different interests are involved in decision-making about human resources for health, which is also the case in the decentralized system of healthcare provision” (Hall and Buch, 2009, p. 34). Such a situation makes it too hard for involved stakeholders to come into consensus on the necessary regulations, working conditions, training requirements and other important structures required in skill mix. Community nursing managers are faced with limited flexibility and are not able to negotiate their way forward as they try to implement skill mix in a way that benefits everyone. Even though many governments remain crucial in the structuring regulations, they still have a limited capacity to enforce the commitment of nurses to the objectives of skill mix.
The authors further explain changing incentive structures as another significant factor affecting the ability to scale up skill mix initiatives in community nursing. “Appropriately implementing new or enhanced professional roles for existing professionals have been highlighted as critical factors in the success and sustainability of skill mix initiatives” (Bourgeault and Mulvale, 2006, p. 5). This is evident in countries such as the United States, Canada and the United Kingdom. “If the substitute professionals’ skills are comparable to that of the current professional group, this negates any benefits” (Hutchinson, Marks and Pittilo, 2001, p. 1250).
There are many other factors that influence how skill mix initiatives and their role in skill transferability are implemented. For example, “in Russia, where most human resource issues are defined by the federal law of labor, the potential exists to have the government support skill mix initiatives” (Jones et al., 2005, p. 560). Weak professional development mechanisms still pose as one of the major challenges for regions trying to implement skill mix in their nursing sector. The decision on whether to develop and upgrade nurses’ skills in a school setting or have this is done during practice through skill mix, is many times based on available structures.
Educational competence and capacity are critical determinants of what role skill mix plays as a professional development initiative in community nursing. If a team is made of inadequately trained community nurses, then they may not be able to influence each other positively as far as skills and knowledge are concerned. To understand why this is a significant factor, Mason and other authors point out a few case studies where this has been experienced. “As noted in the case of the United Kingdom, educational competence for enhanced or new professional roles is vital, and so is the capacity to train for those new roles” (Mason, Coleman, O’Keefe, Ratcliffe and Nicholl, 2006, p. 437).
This calls for proper and effective educational delivery structures in community nursing training institutions. In countries such as Spain where community nursing programs only involve short training programs, educational capacity and competence has been a significant concern. It is for this reason that the country has been for a long time debating on whether teaching of community nurses should be upgraded and the scope of training be expanded.
Successful transfer of skills in a team is achievable when things are done in a systematic order. There has to be a detailed establishment of skills available, and those lacking in each member of the team. To understand this procedure, the skill mix cycle is explained in details by Buchan using his research and other authors’ works as quoted in his article. Among the works he uses is that of Maynard and Scott who explain that the first step in skill mix implementation is evaluating the problem. “Firstly, there is need to define the current services, in terms of activities, professional capabilities, staffing configuration and many other considerations” (Maynard and Scott, 2003, p. 112).
Change is not possible if there is no clear direction of the starting and ending point. To successfully implement skill mix as a skill transferability initiative, there is need to evaluate its effects. There has to be a clearly set and defined baseline indicator. Factors to consider in this step include activities and roles performed, indicators for measuring outcome, the needs of different client groups, quality of care provided and that expected, and staff involved, there availability and capabilities. After these factors have been put into consideration, “the problems that may be solved by skill mix changes need to be assessed” (McCormack and McCance, 2010, p. 200).
The second is making change happen through identifying and implementing solutions. The third step involves identifying the opportunities and barriers for change. This is through establishing the span for control. The last step is planning for change. This step is where an honest assessment of available resources should be done. It is also the step where required resources are identified and possible returns evaluated.
Why community nurses need skill development
Community nurses play a critical role in ensuring that primary nursing care is available to people with different medical needs. “Traditionally, community nurses meet a continuum-of-health needs that range from the management of specific disease/s to broader community development and public health promotion needs” (Richardson, et al., 1998, p.190). Care programs for a patient must consider all the factors that affect his/her needs and health status.
Making sure that these factors are right is a role that has been left to nurses in the hospital. Outside the hospital, nurses still help ensure they are right through direct involvement or advice to other care takers. “In recent years, the community nurse’s role has began to shift, directing more attention to the provision of disease recovery nursing care for transitioning clients as they move out of the hospital environment ” (Loon, 2007, p.4).
Changing social demographic
“Many developed countries today are experiencing a vastly improved life expectancy” (Spreeuwenberg and Vrijhoef, 2010, p. 29). The demand for health and community services is going up as more countries put in measures to reduce mortality rates due to different reasons. “While it cannot be assumed that all older persons will have increased health needs, age-specific prevalence of profound disability increase from about 5% at age 70 years to 50% at age 90 years” (Loon, 2007, p. 12). This combined with the fact that the baby-boomers generations are approaching these number of years, the need for community nursing is only expected to escalate.
This issue is further made complicated by the fact that most aging persons today are no longer taken care of by their families and relatives. “This is due to geographical distances, escalating numbers of divorce, reducing number of children that couples choose to have today, and a changing attitude towards care for the elderly, among others” (Porter-O’Grady, 2003, p. 107). These factors set a stage for a growth in demand for community nurses and their services.
To effectively address the increased demand for community nursing, it inevitable that many governments and region will need to invest heavily in skill development as far as community nursing is concerned. Stakeholders will need to redesign care and service options to allow community nurses perform more duties and serve more people. Even with the best intentions, nothing much will be achievable if skill development in community nursing is not addressed.
Changing acuity and complexity of clients
“Changes in demographics, living styles and environmental factors will result in increased complexity of care demands” (Loon, 2007, p. 12). The number of aging populations is on the rise. The number of disabilities is still significantly high in most regions. There is also an increase in the number of people suffering conditions that restrict them from core activities. Such conditions include stroke, musculoskeletal, respiratory complications, just to mention a few. “Therefore, it is likely that community nurses will see more people with complex comorbid conditions that impact their ability to self-care” (Buchan, 2004, p. 12).
At a time when the world does not have lasting solutions to the above named trends, the need to prepare and equip community nurses with appropriate skills is overwhelming. Skill development can be achieved through many initiatives such as training, coaching, and skill transferability possible through skill mix (Kernick and Scott, 2002). Skill development and any other initiatives considered must be able to meet the needs of the nurses, and do so in a favorable cost (KaiserEdu, 2010).
Changing value systems
“In community nursing, diverse value systems influence how each person in the nurse/client interaction views the person, the community, health, disease, illness, wellness and the role of professionals in the sickness/wellness situation” (Loon, 2007, p. 20). In the past years, self-medication was an acceptable practice and posed no dangers to the people of a community. Today, health complications are more diverse and one solution may lead to other complications (Bourgueil, Philippe, Julien and Engin, 2008). Drinking alcohol was considered as social pastime activity that brought no harm to the people. Today, modern brews pose major health risks to the consumers. Therefore, there is need for availability of medical consultations close to the people.
As these changes occur, community nurses need cultural competence to be able to influence medical decisions of the people they are serving (Blank and Burau, 2007). In order to serve the people effectively and avoid resistance, they need to align their value systems with those of the people.
This is a bigger need today in increasingly multicultural communities. It is important for community nurses to be able to address the differing practices in communities and address any obstacles that stand in the way of giving professional care. Nurses can do these through skill development and working with other nurses who understand the people they are serving more. Therefore, skill transferability is not just restricted to professional challenges, but also other skills such as dealing with people (Borbasi and Gaston, 2002).
Changing scope of practice
Along with other regions in the world, North Batinah, the place chosen for this study, is experiencing a shortage of nurses. The community nursing sector is affected by the shortages and may not have enough professionals to attend to all the duties (Cowen and Moorhead, 2006). Expanding community nurses’ professional roles will improve decision-making and expand the scope of community nursing (Buchan and Calman, 2005). Therefore, skill development is critical to the region’s capacity to meet its community nursing demands.
The scope of nursing can be expended through various ways. It can be done by adjusting curriculum in schools, increased years of schooling, training, coaching, just to mention a few (Gaist, 2009). It is also achievable through skill transferability where nurses with different skills work with each other, influence and learn from one another.
Methodology
Background
“The pursuit of skill mix in the new National Health Services (NHS) has divided managers and healthcare professionals” (Benner, 2001, p. 100). Opponents argue that if it was to be adopted fully, the threat of losing quality in the sector would be more real. Such a measure would also lead to the erosion of value for quality.
Proponents argue that skill mix will allow the healthcare sector to develop skills through skill transferability and other procedures. The debate over the issue of skill mix continues to heighten and more issues keep arising. For example medical professionals argue that decisions on whether to implement such initiatives should be entirely left to them since the government does not understand the complexities of the profession.
In the context of community nursing, skill mix can be used as a skill transferability initiative. According to Borbasi and Gaston (2002, p. 32), “skill-mix changes may involve a variety of developments including enhancements of skills among a particular group of staff substitution between different groups and innovation of roles”. The sector will many times take the option of hiring and working with unqualified personnel that spend money on conducting further training on nurses. “At its best, however, careful consideration of skill mix offers much in terms of aligning services more effectively and more appropriately to the health needs of local populations” (Wrede, 2008, p. 129).
It is important to realize that skill mix works by ensuring that each community nurse has a unique cluster of skills, a very significant factor in the completion and success of various team works. Skill mix can be used as encouragement to have community nurses expand the scope of their skills and knowledge, and develop different styles that suit the current medical needs (Ministry of Social Affairs and Health, 2002). When skills are properly nurtured and developed, it is easier for them to be transferred to other team players in the course of working together. This research paper is aimed at researching on these arguments and giving a conclusion and recommendations based on the results.
Research methodologies to be used in this research project will include the study of books, academic journals, online articles, past projects by different authors, statistics from government and non-governmental organizations on skill in the healthcare sector. It will also involve a study of various academic works and research papers on skill mix, skill development and human resource crisis management in the healthcare sector.
From books, different academic articles and online articles already reviewed, it is clear that the healthcare industry is among those suffering increased need for care services and a diminishing capacity to satisfy them. To prevent such challenges, the industry has realized that the most important factor in human resource management today are skill development. This is best achieved through different initiatives such as skill mix, motivation, and appreciation. As a result, a lot of attention is being put on skill mix in the healthcare sector.
It is also clear that the sector is spending a lot of money to ensure satisfaction, safety and motivation of the nurses, especially those involved in the challenging tasks of serving communities. These conclusions and information were collected from reports by different research organizations and individual surveys from scholars. Different reports utilized in this proposal served very effective and relevant in an attempt to understand the topic’s background. Recent and past books and research papers by different authors will also be helpful in understanding different skill mix initiatives and strategies as far as skill development is concerned. Views from fellow students will also be collected to get their thoughts on the subject and how it affects them.
Primary data used in this research project will be collected by from a survey conducted on several people from the sector. The survey will be conducted in cooperation with organizations and staff federations in the healthcare industry. It will be open to all employees in the community nursing sector in all categories in North Batinah region in Oman. The survey will be aimed at informing the various discussions on skill mix management, as well as its role in skill development. Involving all employees in the nursing sector, regardless of their category or specific location in the area, will ensure that the survey collects comprehensive information representing all employees in the community nursing sector.
The initial findings of the data will be focused on three main questions;
- Reasons for joining the nursing profession and why they chose to be involved in community nursing
- Reasoning for staying in the nursing profession
- Role of skill mix in professional development from the participants’ view
The survey will target 100 participants. Such a high number is used in order to demonstrate the level of importance of the topic.
The survey will be divided into three sections. The first section will seek to understand reasons that motivated the respondents to join the nursing profession at the first place, as well as their reasons for getting involved in community nursing. The second section of the survey will be aimed at understanding why the respondents have chosen to stay in the profession. There will be different reasons to choose from varying from financial reasons, career development and relationships at work.
The third and most significant section of the survey will seek to gather information on the role of skill mix in professional development in the community nursing sector. This section will cover the participants’ understanding of the concept of skill mix, their appreciation for it, and their views on its relevance in the sector.
Another source of information will be from an interview with five experts in the healthcare industry. Participants will be chosen from their level of experience and understanding of professional development in community nursing. The interview will be aimed at understanding how the culture of skill mix appreciated in the sector, by studying how are able to provide quality through skill development. The interviews will further discuss the need for professional development and training among community nurses, and the role of skill mix in skill transferability.
The interviews will be used to further establish how this has been taken up in different regions such as the United States, the Asian region and the European countries. They will further be used to seek the experts opinion on how through labor regulations, the sector is being forced to establish consultation channels between all the relevant stakeholders before decisions are made. The interviews will further be used to discuss the role of respecting professionals in the community nursing sector and how skill mechanism can be used as a solution to different challenges facing the sector. Creating favorable work conditions is another important issue that will be discussed in the interviews, as well as how far the nursing industry has come in achieving this.
Another significant topic of discussion with the interviewees will be community nurses’ satisfaction and its role in quality ensuring quality in the sector. This topic will cover promotions and career development and how they are being addressed in the nursing profession. Process improvement will be analyzed to understand how by making effort to make a working system better, the sector can make it easier for medical professionals to work. Other important measures to be discussed in the interview will include the role of a good corporate culture, job enrichment and effective skill development.
Data analysis and discussions will be written from the findings in different academic resources, the survey and the interview. It will review and classify findings from different statistics and the situation in the community nursing sector as far as skill mix and professional development are concerned. It will also present statistics and information collected from the outlined sources to get a professional understanding of the topic. The findings will be used to structure an argument and different discussions. The healthcare’s position and capability to manage skill development will also be reviewed, discussed and evidence presented. The results will be interpreted and a more detailed examination given.
Participants
To collect comprehensive data and information, this study will be conducted on 100 participants. It will be open to all employees in the community nursing sector in North Batinah region in Oman. The survey will encourage participants from all categories and locations ion the area to ensure equal representation. It will target 100 participants. The big number of participants signifies the level of importance of the topic.
The interviews will have five participants. The interviewees are expected to have a good understanding of how the culture of skill mix is applied and appreciated in the industry, especially as far as community nursing is concerned. They will be further expected to understand healthcare trends in different regions. Since the interviews will be used to discuss the role of respecting professionals in the healthcare sector and how skill mechanism can be used as a solution to different challenges facing the sector, a long term experience in the sector will be required.
Professional nurses will account for 70% of the participants. Half of these are expected to have had experience in community nursing. The remaining 30% of the participants will include healthcare officials, government representatives in the health sector, and non-governmental organizations working with community nurses. To ensure gender balance in the study, 60% of the participants will be female, while the remaining percentage will be male. There will be an age limit of 25 years to ensure information is only collected from experienced participants. The questionnaires will be accessible to the participants for a period of three months to ensure participants fill them at their own time without pressure.
Recruitment
Recruitment will be done by using social network and online forums to reach out to targeted participants. The snowball technique will also be used to reach the targeted number of participants required for the study. In this technique, people familiar with the study will be used to reach out to more people who will then be directed to the research’s weblink. For the interviews, specific people will be contacted on the phone by fetching their numbers from directories. All participants will be presented with adequate explanations and guidelines for the study. All participants will also be required to fill and sign a consent form agreeing to voluntary participation.
Data collection
The research methodology applied in this research project would be designed to achieve the set objectives of the paper. It will include study of books, academic journals, online articles, past projects by different authors, government statistics and interviews with experts in the health and wellness industry. It will also be through conducting interviews on senior and junior nurses, healthcare experts, and key stakeholders from non-government and government organizations on the issue. To understand the background of the problem, literature relating to skill mix in the nursing sector will be reviewed.
Primary data collection will be done by administering questionnaires and doing interviews. Secondary data will be collected from past research projects, government and non-governmental statistics and other relevant sources. The questionnaires will be filled online and will be divided into three sections. The first section will seek to understand the participants’ reasons for joining the medical profession. The second section will be used to understand their reasons for staying in the medical profession and the third section will be used to seek their view on the role of skill mix in professional development.
Case design
The case design will be comprehensive and complete enough, to allow stakeholders understand and utilize the information in decision-making easily, whether they were part of the research team or not. These stakeholders include nurses, other medical professionals, government officials, and other stakeholders. Reviewing a case design should be critical to ensure its validity and applicability (Farr, 2011).
This will be ensured in this research project. Cross-comparing the case design and its outcome, with similar research projects conducted in the past, will help this research to highlight commonalities and identify areas where the results need to be strengthened. Data analysis tools and software will be beneficial when sorting out data and identifying patterns. As Laurel (2003, p. 43) argues, “data analysis techniques can help gain greater insight into trends being investigated”.
Justification of the methodology
Appreciative inquiry
“Appreciative inquiry is based on the assertion that problems are often the result of our own perspectives and perceptions of phenomena” (Laurel, 2003). The approach will be applicable when identifying what has worked well in the past and applying it in the current situation. This proved the most applicable methods when researching on the healthcare sector’s development and strategic planning. The method will prove particularly relevant when gathering information that will help the sector develop their development plan.
Case study design
According to McBurney and Theresa (2010, p. 230), “case studies are particularly useful in depicting a holistic portrayal of a client’s experiences and results regarding a program”. In order to implement any skill mix initiatives, the sector will need to confirm the effectiveness of its programs and processes. This entails evaluating their strengths, weaknesses and threats. A case design in this research will include arranging a wide range of information from different sources and similar projects in the past by the medical sector or other stakeholders. Comparing the results and patterns of past project will then help this research make relevant conclusions and recommendations. Evaluation will include both straightforward comparison and in-depth analysis.
Interviews
Interviews are a brilliant way to pursue in-depth information about a project. They are particularly helpful when a case needs follow-up, and when answers are required from a particular person (Farr, 2011). “The best way to get information during interviews is to ask open-ended questions” (Laurel, 2003, p. 13). Preparing for interviews will involve choosing settings with the least level of distraction, explaining the purpose of the interview to the interviewees, explaining the purpose of the interview to them, and recording it for reference purposes. This method of research will be beneficial when trying to understand the concept of community nursing, how skill mix can make it better, and any other information that does not involve a large target group.
Questionnaires
Questionnaires will be the most convenient and easy way to collect data from a large population. They are easy to design, and since they do not require a lot of time, it is easy to have respondents to cooperate. Their disadvantages include the fact that they do not allow the researcher to examine complex issues. Since the target group in this research project will be 100 people, questionnaires are considered the most efficient way of gathering information and opinions from them.
Data analysis
Jones (2000, p. 562) defines data analysis as “the process of inspecting, cleaning, transforming, and modeling data with the goal of highlighting useful information, suggesting conclusions, and supporting decision-making”. Data analysis comprises of diverse techniques depending with the type of data, and expected outcomes. When conducting a skill mix study, data mining is an indispensable technique since it involves discovering knowledge, as opposed to describing it.
“In any study focusing on attitudes and perception, the importance of primary data cannot be over-emphasized” (Jones, 2000, p. 562). In such a project, it is expected that at least 90% of the questionnaires distributed will be returned and filled correctly. Interviews will be scheduled early to guarantee enough time for preparation by participants. Secondary data will be extremely valuable and will be collected to augment the research. Before any data is collected, permission will be sought from different authorities such as the relevant ministries and health institutions where the participants work. An initial visit to these institutions will be crucial for introductory purpose, familiarization as well as seeking consent for the research project.
Data analysis tools and software will be beneficial when sorting out data and identifying patterns. As Punch (2006, p. 112) argues, “data analysis techniques can help virtually any research project gain greater insight into trends and insights in the area of study”. Available data analysis tools today include business intelligence platforms, the online analytical processing, excel power, among many others (Zikmund, 2000). Answers to close-ended questions will be analyzed in percentages while others will be individually analyzed and discussed.
Materials
Participants will be required to fill a three part questionnaire. The questionnaires will be available both online and in hard copy to allow participants fill them at their own time and comfort. There will be an available weblink where those who want to fill them online can access them. The questionnaires will be available for duration of three months. Materials needed for this activity will include the questionnaires themselves, a weblink and detailed instructions of what is expected of the participants.
Some interviews will be conducted on the phone. Any information required from government officials will be accessed online, after consent from concerned authorities. Sample investigative questions in this survey will include having participants explain what they understand by skill mix, giving examples of experiences they have had themselves in skill related initiatives. For the rest of the interviews, there will be need to arrange for venues where they will be conducted. Financial resources required for the project are outlined in the budget available at the appendices.
Expected outcome
For the proposed study, it is expected that it will be possible to identify the role of skill mix in professional development. The survey will be focused on community nursing and how skill mix allows the development of skills. It will focus on the role of nursing skill mix on transferability of skills and knowledge among registered nurses working in the community nursing context. It will study the allocation of different skills to nurses to work in one primary healthcare organization.
Interviews conducted on health experts, government officials and other stakeholders will help fully understand the background of the problem, and give a professional view. It is expected that from the information gathered, it will be possible to identify what stakeholders have done so far, what is working and what has failed. Such information will be vital for any country with ambitions of using community nursing to develop a healthy nation.
This research is significant to every citizen of the country. Every country recognizes that the quality of healthcare determines its future. By ensuring proper healthcare decisions are made, a country’s investments and developments in the sector are bound to produce results. The research is also significant to the community nursing sector, policy makers and involved stakeholders. It is significant to the direction that training and skill development takes. It is further expected that the results will help shape the way community nurses and their role in the healthcare sector is viewed.
Skill mix as a substitution or diversification technique will be researched on and discussed. From the literature review, using skill mix as a diversification technique serves more benefits than substitution. Diversifying the skills and responsibilities of nurses allows them to do perform more responsibilities, while being able to deliver in their core responsibilities. This argument will be further researched, evidence gathered and evidence presented on which among the two best applies in skill transferability.
In the process, the research will also establish practical guidelines for community nurses to maximize skill transferability through skill mix. There will be practical guidelines for stakeholders in community nursing considering skill mix as an option to ensuring professional development. Necessary resources and steps will also be established through a comprehensive literature review on the subject. It is expected that steps and guidelines gathered on the same will be relevant, comprehensive and viable enough for easy implementation.
The research will further help understand the value of quality in skills in the context of community nursing. Quality in the healthcare sector is a term that has different interpretations depending with the approach that a person takes. It is defined as the extent to which a product or service satisfy a person or a group (Bannerman, 2002). Quality in healthcare is the process of meeting the expectations of patients and health service staff.
The American medical Association views quality in health care in terms of the degree to which the probability of optimum patient’s outcome is influenced by the care services given to them. In health care quality is judged based on various domains. These domains include: effectiveness, capacity, safety, patient-centeredness, equity access and timeliness (Kim & Coyle, 2009).
Through the research, it will be possible to give suggestions and recommendations on the best quality improvement models. There are various quality improvement models that have been developed to ensure that services and products availed to clients are up to standard and that they meet the expected quality level. In long-term healthcare, extra attention needs to be to ensure that implemented measures are efficient enough and relevant for a long period of time. Applicable quality improvement models in community nursing include: Quality Assurance, Total Quality Management, Performance Improvement, the ISO standards and Six Sigma.
The research will be conducted with an understanding that community nursing is entrusted with a huge responsibility of improving the quality of life of a population. For regions where community nurses play a more significant role than just nursing, quality is both paramount and critical. As more regions compete to have the best healthcare in the world, several challenges and barriers are evident. Policy implementation has been a major obstacle for stakeholders who seek to invest in ensuring quality. The healthcare industry is strongly guarded by long policies and procedures of implementing even the smallest initiatives. As a result, small projects and initiatives might take too long and end up being irrelevant by the time they are incomplete.
Available quality improvement techniques include quality assurance which is involved with monitoring and evaluation procedures and techniques in a project to ensure that desired quality standards are met. In community healthcare, it is applicable to ensure that services provided are up to the recommended standard. Important techniques in quality assurance include putting in place checking and monitoring measures. The process involves assessment of quality to identify outlaying results so as to check if they indicate any inappropriate care.
Performance improvement is a significant technique easily applicable in skill mix to improve performance. Performance improvement is a concept that works towards continuous improvement and consistence in quality (Dunn, 2009). It is more focused on instilling quality in a particular product rather than trying to single out the errors present (Lockwood, 2005). It values the empowerment of individuals through trusting their abilities to improve quality, organizational learning, awareness and being sensitive to the patients needs. This model encourages continuous improvement, identification and prevention of defects (Buetow and Roland, 1999).
The research is further expected to help understand how community nurses can be empowered to perform more roles through skill mix. When well equipped and trained, community nurses perform diagnosis roles, they prescribe drugs, deliver children, do immunizations, follow-up on patients, and much more. By implementing skill mix initiatives, regions that have not been able to utilize their capabilities will be able to do so. For those nurses whose skills are more specialized, skill mix will allow them to perfect their skills even further by having every one perform what they are good at. For those whose responsibilities require them to perform different roles, skill mix will allow nurses to learn from each other, transfer skills to each other and increase their capabilities.
The research is also expected to gather views and suggestions on the role of technology in successful implementation of skill mix. Technology is important for effective management of key processes as the healthcare tries to implement and benefit from skill-mix. “Technology influences management and workforce in any sector by analyzing production, resource impact, routine to non-routine operations, structure impact, industry impact and work impact as well” (Winser and Keah, 2008, p. 100).
It allows the stakeholders together with the work force to match the resources available with technology, through different approaches. The management is able to run operations more easily changing techniques and processes to better and modern ones. Through such benefits, community nursing can be taken to a level where it serves more purpose in different regions.
Skill mix management features personnel administration, organizational management, industrial management and manpower management. People in an organization are a key determinant of how successful it is going to be and how long it will last. It is expected that these views will be discussed in the interviews. As the labor markets get more and more competitive and the need for talent becomes more obvious for optimum performance, human resource managers are facing major challenges as they try to get the best in the market, retain them and ensure they have consistent performance.
The nursing industry has especially been hit by a shortage and retention problems. This has especially affected the community nursing initiatives since they are mostly run by governments and more nurses prefer to work for private sectors. These issues will be discussed from available literature.
From the study, it will be possible to establish and discuss internal and external practices that influence community nursing in the healthcare sector. Internal factors to be discussed in the study include labor policies, training and support policy, shareholders and the labor market. External factors include government policies, legal factors, patients’ needs and technology as identified by Kotter and Heskett (1992). Since the healthcare industry is a significant part of every country, a global presence means that the behavior of different economies has enormous effects on its operations. The role of economical changes and trend, and how community nursing is run will be discussed.
As Beck (2010, p. 34) argues, “successful industries are becoming more adaptable, resilient, quick to change directions, and customer-centered”. The nursing sector today is constantly changing and demands strategic planning and organization. Technological innovations such as Human Resource Management Systems have made it easy for sector to handle information related to skills, knowledge, training and development. It is expected that through the interviews and study of different literature, it will be possible to confirm these arguments.
The issue of competition between government and non-government medical services will be discussed and how this influences community nursing. Gaining competitive advantage as an employer has become a major challenge for the nursing industry. As the labor markets get larger and more competitive, strategic human resource management is a key recipe when formulating effective strategies in the industry. Stakeholder in the sector must be able to establish what works in their human resource management efforts and what doesn’t, to eliminate those strategies that waste time and cost the industry.
Ensuring open communication channels between employers and employees is the first step towards identifying problems and implementing solutions. In order for the nursing industry to realize the benefits various skill mix programs, incentives, recognition, rewards, and strict discipline measures are key strategies towards ensuring that nurses deliver, keep in line with a their organization’s timeliness, and stay disciplined. When such measures lack, the industry’s efforts to have the best talent in their workforce may not be rewarding. These issues will be discussed and analyzed, and recommendations made over how the government can be a better employer to community nurses. This is in recognition that skill mix initiatives in community nursing will not offer many benefits if there are not enough nurses to be involved in it.
Project time schedules
This research dissertation will be completed in a duration of 3 months
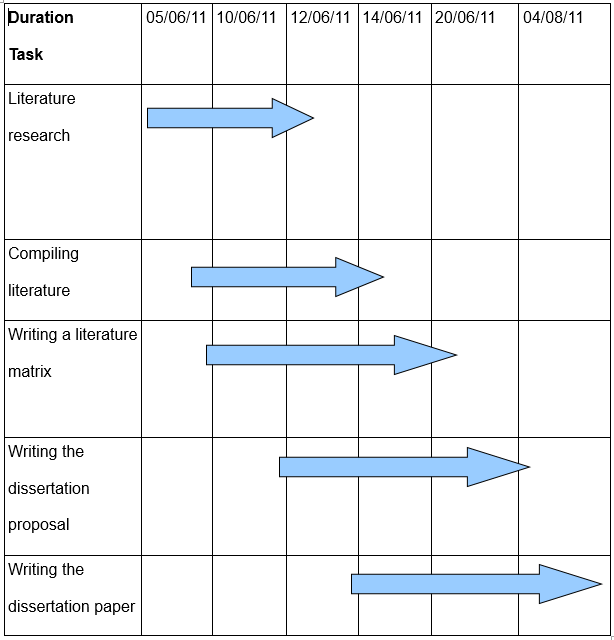
The budget is presented at the appendices.
Ethical considerations
There were a number of ethical issues that arose during the formulation of this research proposal. These issues are further expected to arise during the collection of data for the project. One of the most fundamental principles to be followed in a research project is voluntarism participation. “The principle requires that no participant should be coerced to participate in a research or give false information” (Houser, 2008, p.114 ). A participant must give consent before their identity is revealed if there is a need to do so, although for such a project, anonymity would be applied (Mathers, Amanda and Trent,1998).
During a research project, ethics also demand that the process must not subject the respondents to any danger or harm, a factor that will be taken very seriously. A researcher is supposed to apply the principle of anonymity to protect them from consequences of revealing the information they do (McBurney and Theresa, 2010). It is also the respondent’s right to be treated with respect and dignity during the study. These ethical issues are expected to be adhered to when this research project is being conducting.
Limitations
Limitations faced and further expected in the research exercise is language barriers since the health care industry employee a large number of foreigners. This makes it a bit difficult to collect views for the study. Lack of cooperation from some respondents is also a significant challenge and there are always fears that they may not give accurate answers or take too long to respond. Conducting a research project is an expensive activity and finances pose as a challenge (Houser, 2008).
These challenges will be addressed by conducting any investigations in English which is a common language, and using translators for participants that do not understand English. There will also be comprehensive explanations about the scope of the research to respondents to ensure they understand the objectives of the study. Explanations and elaborations are aimed at minimizing resistance. I will ensure a proper costing and allocation of funds is done before the task commences to take care of any financial challenges that may arise.
Skill mix as a subject raises very many controversies (Bluestone, 2006). Many medical professionals disagree on key issues related to the topic. While many feel that its initiatives could help solve several challenges in the medical profession, they disagree on how policies should be formulated and who should govern the changes that arise. Medical professionals feel that key decisions and their implementations should be left to them (Borbasi and Gaston, 2002).
Government officials on the other hand feel that its their responsibility to foresee any decisions that affect those in need of medical care. Such controversies and debates may pose as a challenge during the research. Too much contradicting information and opinions may make it hard for the paper to come up with a well supported conclusion.
Discussions
This survey is expected to strictly focus on the role of skill mix on transmission of knowledge and skills among registered nurses working in community context. Issues expected to arise in the survey include how different regions have implemented skill mix initiatives, and how well they have served as skill transferability techniques. It is is also expected that the research will help discuss and understand how well the concept has been received by community nurses. Challenges and opportunities will be discussed based on the data and information gathered from different resources, interviews and the survey.
Similar research projects conducted in the past include that carried out by The Queensland Government in 2009. The research was on community health nursing workforce development. It was based in Townsville Health Service District and focused on the current skill mix profiles in the region. The study defined skill mix as “the balance between trained and untrained, qualified and unqualified and supervisory and operative staff within a service area as well as between groups” (Queensland Government, 2010, p. 10).
To gauge the skill mix profile, the report first established the number of new positions added in the region within the last twelve months, as well as number of nurses available for each of the grades. It concluded that skill mix would be a viable option to assist nurses through professional changes in the community nursing sector, and enable skill enhancement.
Another study was conducted by Carr, who focused on perceptions and practice in community nursing. The study, which uses needs assessment factors to drive decisions, “suggested that it is important to recognize the community context of practice and how it increases the complexity of skill mix” (Carr, 2005, p. 74). The research also points out that skill mix and its role in skill transferability is an under-researched area. It concludes that skill mix can be used to address professional development through capturing skills from members of a team and making them available to other nurses.
Further areas of research on the topic in future should include the role of incentives in ensuring that community nurses appreciate skill mix initiatives and benefit from them. Such incentives include compensation for performance, effective human resource management and awareness on the initiatives. As explained, “strategic human resource management aligns an organization’s human resources function to its core business objectives” (Fombrun, Noel and Mary, 1999, p. 67).
This applies even in the healthcare sector. The task of managing employees in the healthcare industry should not be as daunting as it may sound, as long as the sector fully equips itself with the strategies, skills and knowledge to bring out the best of its employees. Despite the fact that proponents of human resource strategies have outlined their benefits to organizations for a long time now, they are not as widespread as may be expected. The results have been poor management of skills and increased costs of hiring and training new employees every too often.
As explained by Taylor (2002, p. 44), “strategic HR management involves more than just the administration of human resource programs or activities”. Effective skills management involves applying these strategies to employees’ management. This is further explained by Stewart who points out that “skill management should help an industry incorporate their plans into the mainstream of the industry’s strategy and management” (Stewart, 1995, p. 66).
It is also supposed to help organizations think strategically as far as human resources are concerned. According to Bratton and Gold (2003, p. 32), another significant benefit of strategic skill management is “designing performance incentives plans with the intention to continuously motivate employees and thus improve performance in a dynamic environment”.
Another area of study that should be given attention in future, and one that attracts a lot of attention is the relationship between different initiatives in the industry and costs. Health care finance and economics as a challenge in skill mix is explained by different analysts who argue the need to address the issues of cost in the healthcare industry. According to Eastaugh (2004), although citizens benefit from developed healthcare and nursing structures put in place in different nations, the costs are uncomfortable for most tax-payers. Administrative costs are a major contribution to the high costs of healthcare.
In many countries, it is estimated that administrative costs account for 6%-9% of the total healthcare costs. Administrative costs include salaries, payment for extra duties and other skill development programs. Future research should therefore focus on how skill mix initiatives can be used to minimize costs in the sector.
Conclusion
“Skill mix is involved with re-profiling, grade mix and multi-skilling” (Saarikoski and Leoni-Kilpi, 2002, p. 261).Furthermore, skill development is a key determinant of how well a workforce in any industry will perform. As (Bratton and Gold, 2003, p. 65) explains, “skill management in any organization is charged with the responsibility of implementing policies and strategies related to management of individuals who comprise the work force of an organization”.
In any industry, “the skill management strategy is expected to maximize returns on investment in the organization’s human capital, and at the same time do so in a way that creates minimal financial risks” (Bratton and Gold, 2003, 137). For the healthcare’s skill mix initiatives to pay returns, “skill development strategies must align the supply of skilled and qualified individuals and capabilities of the workforce with the industry’s plans to maximize output and secure future success” (McNamara, 2009, p. 1). Skill development functions have to be performed and implemented effectively and pragmatically.
Skill mix is aimed at initiating changes through substitution, diversification or other initiatives that ensure professional development (Sorense, et al., 2008.). “Changes implemented in skill-mix may be driven by a variety of motives including service innovation, shortages of particular categories of workers (especially in inner cities or rural areas), quality improvement, and a desire to improve the cost-effectiveness of service delivery” (Thyer, 2003, p. 75). When problems in the sector are well defined and established, it is easier to apply skill mix in specific areas and use it as a viable solution.
As McNamara (2009, p. 1) argues, “successful industries are becoming more adaptable, resilient, quick to change directions, and customer-centered”. This is required in the healthcare industry if it wants to develop and reap the benefits of available professionalism in the sector.
The healthcare needs today are constantly changing and demands constant innovations and change of solutions. Skill care management features personnel administration, organizational management, skill management and professional development (Wanless, 2002). As the medical professionalism gets more and more complex and the need for talent becomes more obvious for optimum performance, the sector is facing major challenges as the try to get the best in the market, retain them and ensure quality results (Bakker et al., 2000.).
As the industry further gets larger and more competitive, especially in private practice, strategic skill management is a key recipe when formulating effective professional development initiatives. The sector must be able to establish what works and what doesn’t, to eliminate those strategies that waste time and cost the sector. Another major challenge facing the sector is ensuring talented nurses and other medical professionals stay motivated and disciplined. This is increasingly becoming a concern as the public and private sector compete for the most skilled medical professionals in the industry (Weiner, 2002).
Ensuring open communication channels between all the stakeholders is the first step towards identifying problems and implementing solutions. Incentives, recognition, rewards, and strict discipline measures are key strategies towards ensuring that medical professionals deliver, keep in line with the sector’s timeliness, and stay disciplined (West-Burnham, 1997). When such measures lack, the medical sector’s efforts to develop the best skills in the market may not be rewarding.
Skill mix aims at assessing the nature of skills available for professionals, the expected results and actual results. There are three parts of skill mix initiatives namely; the purpose, return on its implementation and the most appropriate places to apply it. Skill mix constitutes the financial and non-financial aspect. “The financial aspect which incorporates processes and procedures for tracking market rates, measuring job values, designing and maintaining pay structures, paying for performance and giving employee benefits” (Heneman, 2002, p. 11). However, it is important to note that skill mix is not just about skill development.
It is also about other professional rewards such as ethics, which boost an employee’s ability and confidence. Key issues to address in skill mix include how to manage external and internal influences, as well as how to develop individual and team skills.
Skill mix in community nursing should address the most appropriate performance management processes for the healthcare sector, how power should be devolved to community nurses, and how they can manage their own skills development strategies while staying within the sector’s policies to allow every employee in every level is reached. It should also address how to structure and design job evaluation schemes. These will put into focus performance measures and what they are based on.
In today’s scenario, there are various skill mix trends available for the community nursing sector (Gaist, 2009.). As Kernick and Scott (2002, p. 44) explains “more industries today choose to develop increased awareness of the need to treat job measurement as a process for managing relatives, which, as necessary, has to adopt to new organizational environments and much greater role flexibility”. In the healthcare sector, others choose integrated skill development structures that cover every employee regardless of their position. Skill development in community nursing should cover all the nurses regardless of the level of work or duration of experience.
Team development is a common trend today in most industries and more important is being able to deliver as a team (Mathis and John, 2008). Having nurses with different qualities and professional capabilities at work makes it possible for them to deliver as a team. For those whose skills are more specialized, such settings allow them to perfect them. For those whose job positions require them to perform different responsibilities, skill mix will allow them to learn and expand the scope of the responsibilities they can handle.
Other benefits that will arise from skill mix in community nursing include performance awards and more sensitivity to functional skills to enable the sector retain talented employees. Building and developing skills ensures that nurses stay relevant in the sector. Through skill transfer, their skills are constantly updated and so is their knowledge of the patients’ needs. Performance is improved and functionality in increased. When they are able to perform, back each other up and deliver as expected,they are motivated to do more.
From the literature review, there are factors influencing the ability to scale up skill mix initiatives. One of them is contextual frameworks. “The contextual factors that enhance or impinge on the scaling up of skill mix initiatives can be divided into three levels: the macro, meso and micro levels” (Chow and Suen, 2001, p. 352).
The factors cover the influence of regulations and policies that cover practice such as education systems in different regions, professionalism as understood in them different regions, and statutory recognition of nursing in that particular region (Bondas, 2006). “Contextual micro-level factors affect the quality of skill mix initiatives at the level of everyday practice, and include interpersonal relations between the various health professionals and any previous experience they have had with skill mix initiatives” (Fulton, Scheffer, Sparks, Auh, Vujicic and Soucat, 2011, p. 53).
Skill mix serves a solution to several challenges facing the healthcare industry (Aiken et al., 2001, p. 49). It allows the development of new skills and ideas from each other, hence allowing people trained in different professions to build each other’s potential and capabilities. As result, there is more delivery of services with the available number of nurses available (Allan et al., 2000). Furthermore, it can be used to address the current increases in the cost of healthcare, an issue that is suggested for future research. A structure that allows skills growth will make it possible for nurses to focus more on major responsibilities and achieve perfection (McGuire, Henderson and Mooney, 1988).
Another appropriate area where community nursing can benefit from skill mix and transferability is ensuring quality. Skill mix allows the sector to integrate quality improvement techniques through training, coaching, delegation and a properly balanced workforce. Training and skill transferability is aimed at preparing individuals to keep their skills updated and ready to undertake higher levels of work when chance arises (Frankel, 2008). It also provides a possibility of performance change. Skill transferability will help the nursing industry retain their pool of human resource and stay up-to-date with current and relevant skills in the market. It also makes the nurses feel cared for and are then motivated to give better quality to their clients.
In conclusion, skill mix in community nursing will play a significant role in ensuring professional development (Griffeth and Peter, 2001). It plays a major role in skill transferability by allowing nurses to influence each other and teaching each other new ideas and skills. Developing community nurses skills allows them more efficiency in their supportive role to the physicians. Having a team of nurses with different skills allows more work to be done and patients with different needs attended to.
This research will analyze in depth the role of skill mix in skill and knowledge transfer by using research methodologies that allow an in-depth collection of information and data. These will include academic resources, statistics from different sources, and data from past research projects on the same topic from different authors. The most effective way to collect primary data in this survey will be conducting a survey on 100 participants. It will also be through interviews and discussions with a number of people chosen using a specified category. Its from the results that discussions and arguments will be developed. From the results, conclusions and recommendations will be drawn.
Recommendations
Skill mix initiatives in community sector should be able to identify which performance management processes are appropriate for it. The sector must be able to identify its needs and implement strategies that address them (Babwin,1998). Accessed on June 04, 2011 from Proquest.). Developing skills in any industry is a great way to ensure every employee benefits from professional growth strategies (Adkins, 2005).
Devolving powers in the sector is a good way to ensure that professionals in the industry can manage their own skill mix strategies while staying within the corporate policies. They are then able to reach every employee regardless of their level of employment (Gratton, 1999). The human resource management department may not be able to identify, recognize and reach all employees in the sector. Community nurses have less contact with the human resource managers. Allowing them the skills and power to implement skill mix initiatives at their own level is a way to reach everyone in the sector (Blank and Burau, 2007).
“How jobs are designed and evaluation schemes structured play a very important role in determining the level of success in skill mix” (Haesli and Boxall, 2005, p. 1954). Jobs designs should allow community nurses and other medical professionals working with them to accomplish their goals and targets. Undefined job responsibilities make it hard for employees and organizations to measure success (Cole, 2002). Evaluation schemes must also ensure that employees are tested on all relevant performance levels (Daft and Dorothy, 2009). They should test target deliveries, employee’s relationships with colleagues, and discipline levels among others. This way, skill mix becomes a comprehensive solution to most of the professional challenges facing the sector.
Appendices
Questionnaire
Fill your sex and age in the box
Age__
Sex___
Section 1
- Why did you decide to join the community sector?
- What were you doing prior to joining the sector?
- Did anything in specific motivate you to join the medical field?
Section 2
- For how long have you been practicing in the community nursing context?
- Why are you still in the medical profession?
- Do you consider leaving anytime soon?
- If you were to leave, what would be you reasons?
Section 3
- Are you familiar with the word skill mix?
- In your opinion, is it relevant in community nursing?
- What is its influence in community nursing?
- What is its role in skill transferability?
- Is skill mix a viable way of transmitting knowledge and skills among nurses?
- How does its implementation affect professional development among community nurses?
- If it was to be implemented effectively, what would be the short and long term benefits in community nursing?
- Are medical professionals supportive of skill mix in community nursing?
- Do you think stakeholders have done enough to get the best out of skill mix initiatives in community nursing?
- How would skill mix in community nursing improve performance?
- What is the role of technology in successful implementation of skill mix and helping community nurses benefit from it?
Budget for the research project
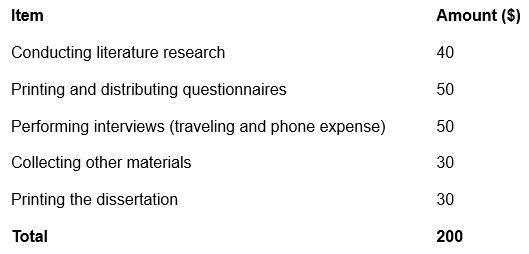
Required materials
- Questionnaires.
- A weblink.
- Detailed instructions of what is expected of the participants in hard and soft copies.
- A phone to contact interviewees and conduct some of them.
- Letters giving consent from concerned authorities.
- Investigative questions in hard copies and a soft copy.
- Venues where interviews will be conducted.
- Financial resources as outlined in the budget above.
Reference list
Adkins, C.L., 2005. Staffing organizations: A comprehensive applied exercise. Human Resource Management Review,15, 226-237.
Aiken, L. et al., 2001. Nurses’ reports on hospital care in five countries. Health Affairs, 20, 43-53.
Allan, H. et al., 2000. Leadership for learning; A literature study of leadership for learning in clinical practice. Journal of Nursing Management, 16, 545-555.
American Association of Colleges of Nursing, 2011. Nursing shortages. Web.
Armstrong, M., Duncan, P. and Peter, R., 2010. Evidence-based reward management: Creating measurable business impact from your pay and reward practices. Philadelphia PA: Kogan Page Limited.
Babwin, D., 1998. Move over JCAHO. Hospitals & Healthcare Network, 72(10), 57-58. Web.
Bakker, A.B. et al., 2000. Effort and reward imbalance and burnout among nurses. Journal of Advanced Nursing, 31, 884-891.
Banham, L. and Conelly, J., 2002, ‘Skill mix, doctors and nurses: substitution or diversification?’ Journal of Management in Medicine, vol 16, no. 4, pp. 257-270.
Bannerman, C., 2002. Health care quality assurance manual. Ghana: Ghana printing press.
Beck, D., 2010. HR can help ensure the success of family business-From mom- and-pop stores to Wal-Mart. Employment Relations Today, 35 (4), pp. 31-38.
Benner, P.E., 2001. From novice to expert: Excellence and power in clinical nursing practice. Upper Saddle River, N.J.: Prentice Hall.
Blank, R.H. and Burau, V.D., 2007. Comparative health policy. Houndmills: Palgrave Macmillan.
Bluestone, J., 2006. Task shifting for strategic mix. New York: Chapel Hill.
Bondas, T., 2006. Paths to nursing leadership. Journal of Nursing Management, 14, 332-339.
Borbasi, S. and Gaston, C., 2002. Nursing and the 21st century: What happened to leadership? Collegian, 9(1), 31-35.
Bourgeault I.L. and Mulvale, G., 2006. Collaborative healthcare teams in Canada and the U.S.: Confronting the structural embeddedeness of medical dominance. Health Sociology Review, 15(5), pp. 481-495.
Bourgueil, Y. and Philippe, L.F., Julien, M. and Engin, Y., 2008. Gps teamed up with nurses: A skill mix experiment improves management of type 2 diabetes patients. Web.
Bratton, J. and Gold, J., 2003. Human resource management theory and practice 3rd ed. London: Bath Press.
Buchan, J, 2004. Determining skill mix: practical guidelines for managers and health professionals. Web.
Buchan, J. and Calman, L. 2005, ‘Skill Mix and Policy Change in the Health Work Force: Nurses in Advanced Roles’, OECD Health Working Papers, 24, pp. 2-63.
Buchan, J. and Dal Poz, M.R., 2002, ‘Skill mix in the health care workforce: reviewing the evidence’, Bulletin of the World Health Organization, 80(7) , pp. 575 – 580.
Buetow, A. S. and Rowland, M., 1999. Clinical governance bridging the gap. New York: Gilford press.
Canham, J. and Joanne, B., 2002. Mentorship in community nursing: Challenges and opportunities. Malden, Mass.: JoAnne Bennett.
Carr, S.M., 2005. Delegation: perception and practice in community nursing. Primary Health Care and Development, 6, pp. 72-81.
Chen, L. et al., 2004. Human resource for health: Overcoming the crisis. Lancet, 364 (9449), pp. 1984-1990.
Cheng, W.L., 1998. Perceived transfer of skills and knowledge on MBA graduates: Test of a model. Hong Kong: Hong Kong Baptist University.
Chow, F.L.W. and Suen, L.K.P., 2001. Clinical staff as mentors in pre-registration undergraduate nursing education: Students perceptions of the mentor’s role and responsibilities. Nurse Education Today, 21, 350-385.
Cole, G.A., 2002. Management: Theory and practice. London: Continuum.
Constable, J.F. and Russell, D.W., 1986. The effect of social support and the work environment upon burnout among nurses. Journal of Human stress, 12, pp.20-26.
Coombs, M.A ,2004, Power and conflict between doctors and nurses: breaking through the inner circle in clinical care, Routledge, New York, NY.
Cowen, P. S. and Moorhead, S. 2006, Current Issues in Nursing, 7th edn, Mosby Elsevier, St. Louis.
Cribb, A. 2005, Health and the good society: setting healthcare ethics in social context, Oxford University Press, Oxford.
Culyer, A. J. and Newhouse, J. P. (eds.) 2000, Handbook of health economics, Volume 1, Part 2, North-Holland, Amsterdam.
Daft, R. and Dorothy, M., 2009. Understanding management. Mason, OH: South-Western Cengage Learning.
Denny, E. and Earle, S., 2005, Sociology for nurses, Malden, MA: Polity Press.
Dierick-van Deale, A.T., Steuten, L.M., Derckx, E.W., Metsemakers, J.F., 2010. Economic evaluation of nurse practitioners versus Gps in treating common conditions. British Journal of General Practitioners, 60(570), pp. 28-35.
Dunn, M.W., 2009. Leadership coaching: The development power of one-on-one. Employment Relations Today, 35(4), p.25-29.
Dyro, J.F., 2004, Clinical engineering handbook, Malden, MA: Academic Press.
Eastaugh, S.R., 2004, Health care finance and economics, Jones and Bartlett Publishers, Sudbury, MA.
Farr, R., 2011. Basic business research methods. Web.
Fisher, M., n. d. Skill mix in health visiting and community nursing teams: Principles into practice. London: Oxford Street London.
Frankel, A.., 2008. What leadership styles should senior nurses develop? Nursing Times, 104(35), pp. 23-24.
Freeman, R., 2000. The politics of health in Europe. Manchester: Manchester University Press.
Fombrun, C.J., Noel, M.T. and Mary, A.D., 1999. Strategic human resource management. New York: Wiley.
Fulton, B.D., Scheffer, R.M., Sparks, S.P., Auh, E.Y., Vujicic, M. and Soucat, A., 2011. Health workforce skill mix and task shifting in low income countries: a review of recent evidence, Human Resource for Health, 9 (1).
Gaist, P.A., 2009. Igniting the power of community: the role of CBO and NGO in Global Public Health, Springer, New York, NY.
Gallup Organization, 2000. Healthcare practice. Web.
Gardner, T., 2002. In the trenches at the talent wars: Competitive interaction for scarce human resource. Human Resource Management, 41(2), pp. 225-237.
Gratton, L., 1999. Strategic human resource management: Corporate rhetoric and human reality. New York: Oxford University Press.
Griffeth, R.W. and Peter, W.H., 2001. Retaining valued employees. Thousand Oaks, Calif.: Sage Publications.
Haesli, A. and Boxall, 2005. When knowledge management meets HR strategy: An exploration of personalization-retention and codification-recruitment configurations. International Journal of Lock Human Resource Management, 16(11), pp. 1955-1957.
Hall, M.L. and Buch, E., 2009. Skill mix decision – making for nursing Series Paper, ISBN: 978-92-95065-75-8. Geneva: International Centre for Human Resources in Nursing.
Harris, MG 2005. Managing health services: concepts and practice, 2nd edn, Elsevier, Marrickville.
Health Committee 2006-07, 2007. ‘Workforce planning: fourth report on session 2006-07, Volume 1’, Session Report, Health Committee, Great Britain House of Commons, House of Commons.
HealthInsite, 2011. Community nursing. Web.
Heneman, R.L., 2002. Strategic reward management: Design, implementation, and evaluation. Greewich, Conn.: Information Age Publications.
Hongoro, C. and McPake, B. 2004. How to bridge the gap in human resources for health. Lancet, 356, pp. 1451-1456.
Houser, J., 2008. Nursing research: Reading, using, and creating evidence. Sudbury, Mass.: Jones and Bartlett Publsihers.
Hughes, S. (2004). The mentoring role of the personal tutor in the “fitness for practice” curriculum; An all Wales approach. Nurse Education in Practice, 2, pp. 271-278.
Hutchinson, L., Marks, T. and Pittilo, M., 2001. The physician assistant: Would be US model meet the needs of the NHS? British Medical Journal, 323, pp. 1244-1247.
ICN, 2002. ICN announces its positions on advanced nursing roles. International Nursing Review, 49, pp. 202-206.
Jenkins-Clarke, S., Carr-Hill, R., Dixon, P., and Pringle, M., 1997. Skill Mix in Primary Care, A study of the interface between general practitioners and other members of the primary health care team’. York: University of York, Centre for Health Economics.
Joint Commission on Accreditation of Health Care Organizations, 2005. Accreditation Manual for Critical Access Hospitals, Joint Commission Resources, Oakbrook Terrace.
Jones, T.M., 2000. An integrating framework for research in business and society: A step toward the elusive paradigm. The Academy of Management Review, 8(4), pp. 559-564.
KaiserEdu, 2010. U.S Healthcare Costs. Web.
Kernick, D. and Scott, A., 2002, Economic approaches to doctor/nurse skill mix: problems, pitfalls, and partial solutions. The British Journal of General Practice, 52 (474) pp. 42-46.
Kernick, D. and Scott, A., 2002. Economic evaluation and doctor/nurse skill mix :Getting health economics into practice. Oxon: Radcliffe Medical Press
Kim, S. and Coyle, N., 2009. Quality of health care in England, Scotland, Wales & Northern Ireland: an intra-UK chart book. Oxford: Oxford University Press.
Kotter, J. and Heskett, J., 1992. Corporate culture and performance. The Free Press.
Kuokkanen, L. and Leino-Kilpi, H., 2000. Power and empowerment in nursing: Three theoretical approaches. Journal of Advanced Nursing, 31(1), pp.235-251.
Laurel, B., 2003. Design research: Methods and perspectives. Cambridge, Mass: MIT Press.
Lockwood, N.R., 2005. Crisis management in today’s business environment: HR’s strategic role. HR Magazine, 50(12), pp.1.
London Department of Health, 2002. HR in the NHS plan: More staff working differently. London: London Department of Health.
Loon, A.V., 2007. The changing professional role of community nurses. Web.
Marriner-Tomey, A., 1993. Transformational Leadership in Nursing. London: Mosby.
Mashaba, G.T., 1994. Nursing education: An international perspective. Kenwyn: Juta.
Mason, S., Coleman, P., O’Keefe, C., Ratcliffe, J. and Nicholl, J., 2006. The evolution of the emergency care practitioner role in England: Experiences and impact. Emergency Medical Journal, 23 (6), pp. 435-439.
Mathers, N.J., Amanda, H. and Trent, F.G., 1998. Ethical considerations in research. NHS Executive, Trent.
Mathis, R.L. and John, H.J., 2008. Human resource management. Mason, OH:Thomson/South-Western.
Maynard, A. and Scott, A,. 2003. Advances in health economics, John Wiley & Sons Ltd, West Sussex.
McBurney, D. and Theresa, L.W., 2010. Research methods. Belmont, CA: adsworth Cengage Learning.
McCormack, B., Kim M. and Robert, G., eds. 2004. Practice development in nursing. Oxford: Blackwell Publishing Ltd.
McCormack, B., and McCance, T., 2010. Personal-centered nursing – theory and practice, Wiley-Blackwell, Iowa.
McGuire, A, Henderson, J. and Mooney, G., 1988, The economics of health care: an introductory text. London: Routledge & Kegan Paul Ltd.
McNamara, C., 2009. Human resource management. Web.
Ministry of Social Affairs and Health, 2002. Decision in principle by the council of the state on securing the future of healthcare. Helsinkin: Ministry of Social Affairs and Health.
McSherry, R. and Jerry, W., 2008. An introduction to excellence in practice development in health and social care. Maidenhead: Open University Press.
Moram, R., 1999. Governing the healthcare state: A comparative study of UK, USA and Germany. Manchester: Manchester University Press.
National Pharmacy Association, 2010. Skill mix- Up skilling your staff. Web.
Parle, J.V., Ross, N.M. and Doe, W.F., 2006. The medical care practitioner: Developing a physician assistant equivalent for the United Kingdom. Medical Journal of Australia, 185 (1), pp. 13-17.
Porter-O’Grady, T., 2003. A different age for leadership, part 1. Journal of Nursing Administration, 33(10), pp. 105-110.
Punch, K., 2006. Developing effective research proposals. London: SAGE.
Queensland Government, 2010. Community health nursing worforce development report. Queensland: Queensland Governanment.
Rallings,J., 2009. Community health nursing competency and skills. Web.
Rechel, B. and Dubois, C.A., 2006. The health care workforce in Europe: Learning from experience. Copenhage: WHO regional Offices for Europe.
Rese, et al., 2005. Implementing general practice in Russia: Getting beyond the first steps. British Medical Journal, 331, pp. 204-207.
Richards, A. et al., 2000. Skill mix between nurses and doctors working in primary care-delegation or allocation: A review of the literature. International Journal of Nursing Studies 3, pp. 185-197.
Richardson, G. et al., 1998. Skill mix changes: Substitution or service development Health Policy, 45, pp.119-132.
Saarikoski, M. and Leoni-Kilpi, H., 2002. The clinical learning environment and supervision by staff nurses: Developing the instrument. International Journal of Nursing Studies, 39, pp. 259-267.
Shumbusho, F., Van-Griensven, J., Lowrance, D., Turate, I., Weaver, M. and Al, E., 2009. Task shifting for scale-up of HIV care: Evauation of Nurse-Centered Antiretroviral Treatment at Rural Health Centres in Rwanda. PLoS Medicine, 6(10), p. e1000163.
Sorense, R. et al., 2008. Beyond profession:Nursing leadership in contemporary healthcare. Journal of Nursing Management, 16, pp. 535-544.
Speck, M. and Knipe, C., 2005. Why can’t we get it right? Designing high-quality proffessional development for standards-based schools. Thousands Oaks, Calif.: Corwin Press.
Spreeuwenberg, C. and Vrijhoef, H.J., 2010. Economic evaluation of nurse practitioners versus GPs in treating common conditions. The British Journal of General Practice, 60(570), pp. e28-e35.
Stewart, G., 1995. Staff turnover: An analysis of casual factors that contribute to the attrition and retention of experienced nurses and midwives and Auckland Healthcare Services Limited. Auckland: University of Auckland.
Taylor, S., 2002. The employee retention handbook. London: Chartered Institute of Personnel and Development.
Thyer, G., 2003. Dare to be different: Transformational leadership may hold the key to reducing the nursing shortage. Journal of Nursing Management, 11, pp.73-79.
Trautman, S., n.d. Supporting change with knowledge transfer skills. Web.
Wanless, D., 2002. Securing our future health: Taking a long term view. London: HM Treasury.
Weiner, B., 2002. Human motivation: Theories and research. Newbury Park, California: Sage Publishers.
West-Burnham, J., 1997. Leadership for learning-reengineering’mind sets’. School Leading Ability and Management, 17(2), pp. 231-244.
WHO, 2007. Health workforce policies in the Europena region. Copenhagen: WHO Regional Offices for Europe.
Winser, J., and Keah, T., 2008. Principles of Supply Chain Management: A Balanced Approach. Mason, OH: South-Western Cengage Learning.
World Health Organization, 2006. The world health report: Working together for health. Web.
Wrede, S., 2008. Educating generalists: Flexibility and identity in auxiliary nursing in Finland. International Directions in Health Care, 5, pp. 127-140.
Yoder-Wise, PS 2003, Leading and managing in nursing, 3rd edn, Elsevier Health Sciences, Malden, MA.
Zikmund, W., 2000. Business research methods. Web.