Abstract
The conclusions of this awfully intense and ruthless respiratory syndrome (SARS) in Hong Kong shaped many issues for health support behavior among older citizen with a poor social and financial standing and so. With an alarming situation that this helpless group could be at superior risk of contracting the sickness or spreading it to others, the accomplishment of health endorsement activities appropriate to this group was measured to be essential through the epidemic. So we employed Behavioural and Cognitive-behavioural therapy for their treatment
Objectives
What we are doing in this paper is to assess the effectiveness of delivering a telephone fitness education program that will deal with nervousness levels, and data and practice of measures to avoid transmission of SARS among some senior citizens with low SES and for this intention we are focusing on the Behavioural and Cognitive-behavioural therapy to cure such people. Various Subjects were employed from licensed associate of a government aided and sponsored social examine centre in Hong Kong and living in inexpensive accommodation estates.
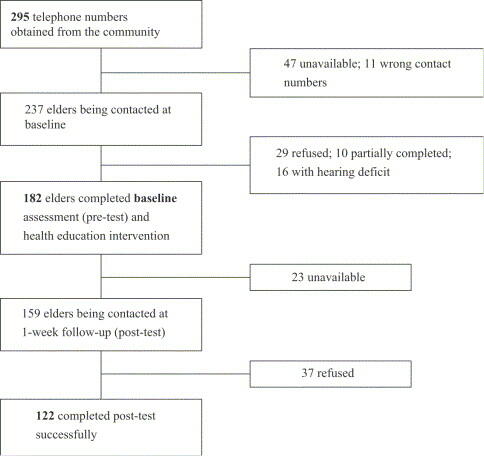
The eligibility criteria were: (1) aged 55 or above; (2) able to speak Cantonese; (3) no hearing impairment, and (4) reachable by telephone. Of the 295 eligible subjects, 122 senior citizens completed the whole study.
Introduction
The aging population is mounting in Hong Kong, as it is in a different place. In Hong Kong, an adult aged 55 or above is measured as an older adult for the reason that of the lowering age of giving up jobs. (Department of Health, 1-45) with nearly equal to 21.2% (n=1,475,000) of the entire population aged 55 years or greater than that as Hong Kong Census and Statistic Department (HKCSD), declared on 31 December 2005 In fact not like other demographic groups in Hong Kong, literacy rates are low down in this group with more than 31.2% not having take on any formal learning. We investigated that the citizen who have taken little formal education, 39.5% finished primary education only so in other words, simply a small percentage of older citizens in Hong Kong are educated over primary stage (Department of Health, 11-45).
This grave condition presents different tasks for physical condition encouragement and disease obstacle activities, as numerous of the usual methods of spreading health information are not right for these inhabitants. Such sort of tests was mostly visible through the epidemic of brutal acute respiratory syndrome in Hong Kong. Over the path of the outburst, 1755 cases were report with 300 losses. Senior citizen of 55 years of age or older were 26.2% of the SARS cases but, the age-specific mortality rate for this mature demographic was concerning 54.5%. (Department of Health, 11-45)
Important things to start the project
- Experimental evidence on the success of telephone fitness learning among older citizens with least or no reserved education is missing.
- Low physical condition knowledge among the senior citizens and adults may produce a barrier in understanding of mass health learning against SARS, which might be critical for effecting behavioural transform. (Department of Health, 11-45)
- Telephone cognitive treatment could be an efficient means in improving health awareness by providing personality counselling on physical situation behaviours and communal sustain among senior citizens who lives unaccompanied.
- This is the most primary systematic examination to know the effectiveness of delivering telephone physical strength health education to senior citizens during the occurrence of SARS in Hong Kong and this analysis also add some knowledge on achievability and effectiveness of provided that telephone involvement for senior citizens in an infectious sickness outbreak, thus progressive its applicability in possible pandemics like avian and other influenzas (Department of Health, 1-45)
- As most of the people will rely that telephone health education is a safe and sound measure to provide health instruction when face-to-face measures are not feasible during eruption of infection (Department of Health, 11-45).
The Hong Kong Government begins a movement to keep the city healthy and dirt free. Measures to stop the transmission of SARS related to individual hygiene and ecological cleanliness was publicized daily in the media as a way to decrease infection. Nonetheless, the presence of functional harm resulting from chronic infirmity or facts deficits due to lesser literacy levels among the senior citizens may have an effect on their sympathetic and perceived relevance to habitual hygiene practice. Their observance to recommended illness control trial might be low and thus, more apprehension about senior citizens mainly those living alone was expressed by healthiness care providers and in the print and electronic media. While not paying attention to fitness and health measures among susceptible age group could create a very higher danger for contracting SARS and transferring the infections to others once turn out to be a carrier. In scrutiny of this confront, an alternative means to provide health instruction and support for them was considered vital to make sure the effectiveness of communicating the needed health messages to this defenceless group, specially during the eruption of SARS (Department of Health, 11-45).
According to the WHO, electronic -health recommends the use of electronic means into apply of defensive and promoting mental and cognitive condition so it can help provide health information and services to the public who have complexity in accessing healthcare institutions due to bodily illness, deficient resources, ecological constraints or other causes. Electronic -health relies on a number of advance expertises ranging from uncomplicated systems (e.g., telephone, duplicate machines) to multifaceted systems (e.g., satellite links, and incorporated services digital network). Among different sort of technologies, the phone can present a low-cost, convenient and simple method of delivery for health data, education and cognitive assistance for senior citizen at home. Ninety-three percent of the inhabitants have a telephone at home and it is also careful to be a safe evaluate of contact when having the SARS outbreak. (Department of Health, 11-45) Many examinations have shown that telephone contacts can have a very fine impact on various health promotion or illness avoidance programs. Various examiners have examined the effect of telephone appointments for influenza vaccination at a nurse-run clinic for 1820 senior citizens in the United Kingdom. They discover that that the uptake of immunization among the senior citizens was boosted by 6% by means of telephone meeting. (Department of Health, 11-45) inspected the positive effects of a telephone give up smoking service for about 3300 contributors in the USA. So by employing a randomised controlled trial plan, they found that the rates of smoking abstinence for the interference group were notably higher than for the organizers (p<0.001). Parallel outcomes about telephone counselling for smoking stop, manner towards current conduct knowledge on disease and prescribed ordinary medications (Department of Health, 2001,) were also accounted.
Even if not all literature supports the helpful effects of telephone learning on health promotion movement, for the idea of this examination, it was considered to be a gainful means of communication, and protected for both senior citizens and interviewers under the courage of minimal contact throughout the SARS outbreak. Student’s male attendant and nurses of a university hospital in Hong Kong consequently realized a telephone health promotion programme for a group of senior citizens. The aims of the examination were: (1) To find the bottom line data of senior citizens about their level of anxiety, facts of the main transmission routes of SARS, and events taken to prevent the spread of SARS. (2) To supply senior citizens with data related to the conduction modes of SARS and defensive measures as well as hold up through a fitness education programme (Department of Health, 66-78).
Literature Review
Empowerment has become an attractive concept for practitioners working with elder people, women and adolescents. It acknowledges that young people have a distinct capacity for facing life challenges and achieving positive development. It also focuses on raising youths’ consciousness to address society’s institutional or structural problems that adversely affect their lives. (Department of Health, 66-78) While many practitioners adopt the empowerment approach in rendering youth services, however, little attempt has been made to examine the concept of empowerment and its relevance to school social work. While education affects adolescents’ future trajectory of life and school social work is a significant auxiliary service in the school setting, there is a need for practitioners to explore the possibilities for generating empowering practices (Department of Health, 66-78).
School social work service has existed for almost a century in the develop countries but in Hong Kong situation is not satisfactory. Previously, school social workers emphasized assisting individual students, especially those who are maladjusted, in adapting to schools and using the learning opportunities presented there. During the transformation of modern school social work, practitioners have considered wider social systems contributing to the students’ situations and have identified a developmental perspective of this service. Nevertheless, the issue of balancing between serving individual students and serving the educational institution remains controversial. Some school social workers play the advocacy role in bringing about positive changes to the education sector, while others concentrate on helping students adjust in the existing school system. (Department of Health, 66-78) This dilemma is not only theoretical but also touches on the heart of school social work practice. It is suggested that the empowerment perspective, as it takes heed of social work’s dual obligation to both the individual and society and of their dialectical relationship, can replace the dichotomy of personal change against institutional change to become the theoretical foundation of school social work (Department of Health, 66-78).
In Hong Kong, school social work service has existed for more than 30 years, and the policy of “one school social worker for each secondary school” (Department of Health, 66-78) was implemented in 2000. This service was positioned as an integral part of the school system according to the government’s policy. Nevertheless, although the empowerment approach has become a rising trend in many youth service units, the practice of empowerment in school social work remains underdeveloped (Department of Health, 66-78).
Local practitioners have sought to achieve a balance between changing individual students and advocating improvement in the education sector, yet the criticism has been that they put more emphasis on helping students adapt to the school environment rather than to mobilizing students and school personnel to initiate constructive changes to the school and education systems the practice of empowerment in the field of school social work simply empty rhetoric? This paper explores the possibilities for carrying out empowering practices among school social workers in Hong Kong. It investigates how school social workers use various strategies to interact with service users, service partners, the school, the community, and the education sector to generate empowering practice for positive youth development (Department of Health, 66-78). It also discusses whether the concept of empowerment is applicable in the context of elderly care and school social work. Empowerment by the help of Behavioural and Cognitive-behavioural therapy in the school and community are perceived as political arenas that practitioners must take into account (Department of Health, 66-78). They are highly significant for promoting outcomes associated with positive experience and performance of young people. It is therefore necessary for practitioners to treat the school and the community as both the subject of empowerment and the crucial channels for empowering service users and partners. At the initial stage of data analysis, a set of narratives arose that depicted the insufficiency of empowerment in these dimensions. Further review of the stories showed, however, that the research participants indeed chose their battlefields very carefully. They first went for easier victories to carry out the personal dimension of empowerment before tackling the bigger issues in the school and community. They also perceived empowerment in the school and community dimensions as a long-term “battlefield.” (Department of Health, 66-78).
Collaborate with school personnel to initiate positive changes to school policies. Empowerment in the school dimension is realized by altering school policies that pose barriers to students’ social and educational functioning. The narratives of Mary and Joyce are good examples of how practitioners empower school personnel to identify and modify school policies that curtail students’ learning and development and how they motivate school personnel to refine the punitive student codes of conduct. In the case of a student with learning difficulties, Mary gained the support of school personnel to pursue organizational changes in response to the student’s needs. We were modifying the school policy to suit student needs, and the result was very satisfactory. The student could be promoted to a better class in Form Two, and she could receive her classmates’ support and acquire better communicative skills (Department of Health, 66-78). The school personnel might feel worried that if they broke the school policy, many students would request promotion to a better class, and then they would face a lot of troubles. However, in this conference they began to think that the development of a student was more significant than the maintenance of certain school policies (Department of Health, 33-55). The adjustment of the promotion mechanism is a kind of organizational change. Once school personnel agree to adjust the school policy in response to a special case, it becomes a reference for the future. The school in Mary’s narrative also provided extra resources for the student and made adjustments to the curriculum and academic standards to suit her study pace. As discussed in the previous section, Joyce assisted a service user in complaining to the District Council and the Education and Manpower Bureau about her discontent with the school penalty policy (Department of Health, 2006, 33-55). Although there was no immediate change in the policy after those actions, Joyce did not give up. She formed an alliance with some teachers and put the item on the agenda of a meeting. Finally, a consensus was reached (Department of Health, 33-55).
I voiced my view in the coordination meeting of the discipline committee, the counselling team, and the school social worker. I claimed that it was meaningless and useless to record students’ names so frequently… I also tried to help the school personnel think about why students failed to hand in their homework assignments on time. Maybe there were many underlying problems. They accepted my viewpoint, and thus there was a set of new arrangements that the students’ names would only be recorded a maximum of two times, and teachers would follow up with those students.
We have regular sharing sessions for welfare organizations in this community, and I think it is worthy to attend these sessions because we can discuss our common concerns on youth affairs in this community. Furthermore, we can attend the meetings of the District Council, or we have joint efforts with the police, school, and other welfare organizations on some issues. I think we have different levels of cooperation, and we have many channels and opportunities to exchange our information and opinions (Department of Health, 33-55).
Methodology
To examine the effectiveness of the program in terms of the participants’ anxiety, knowledge about the main transmission routes of SARS and measures for preventing SARS
Sample and design
The study used a pretest/posttest design. Potential subjects were recruited from registered members of a government subsidized social servcentrenter in the Southern District of Hong Kong which provides various services to senior citizens such as home visits, social activities and meals-on-wheels service. The criteria were theme who: (1) aged 55 or over; (2) were talented to converse Cantonese; (3) had no hearing injury, and (4) were accessible by telephone. (Department of Health, 33-55)
Initially, 295 registered members of the social service centre were contacted by telephone to determine their eligibility; a total of 182 senior citizens were successfully contacted at baseline for health assessment and health education (i.e., response rate=61.7%). However, only 122 completed the post intervention questionnaire (i.e., follow-up rate=67%). The attrition in the follow-up was mainly due to refusal and non-response telephone calls (Fig. 1).
Measurement
A survey instrument developed by Leung et al. (2003) was modified and adapted for the use in this study. The original survey instrument comprised 60 questions and is divided into seven parts: (1) self-perceived general health status and level of anxiety; (2) use of health services; (3) possibility of contacting diagnosed SARS cases; (4) belief of contracting SARS; (5) knowledge of transmission of SARS; (6) measures taken to prevent transmission of SARS; and (7) socio-demographics. Other details of the instrument have been described in this paper, the level of anxiety, knowledge level regarding SARS transmission modes, and practice of preventive measures will be presented (Department of Health, 33-55).
Procedure
The Institutional Review Board approved this study. All the potential subjects were approached via telephone during the period between 15 and 25 May 2003 to determine their eligibility. After gaining their verbal consent, interviewers collected the baseline data regarding the level of anxiety, knowledge and preventive measures taken to prevent transmission of SARS. Based on the results of the baseline data, the interviewer provided health education to the participants and clarified their misconceptions. A follow-up phone call was made 1 week after the collection of the baseline data and interviewers used the same questionnaire for evaluation (Department of Health, 33-55).
Data analysis
The level of anxiety, knowledge and practice of preventive measures regarding SARS were the main outcome variables. Descriptive statistics were used to assess all variables. Paired-sample t-test was used to assess the level of anxiety before and after the intervention. The McNemar test was used to examine the change of the level of knowledge about the transmission routes of SARS prior to and after the intervention. Sign test was used to investigate the change of practice of preventive measures before and after the intervention. An alpha of 0.05 or less was considered significant. (Department of Health, 33-55)
Results
Demographics
Information about the demographics of the participants is presented in Table 1. The majority of the participants were female (63.0%). More than half of the participants (58.3%) did not live with the family. The majority did not have any formal education (50.0%) or received low educational level (30.2%). About 83.0% were retired and did not have a monthly income. (Department of Health, 33-55)
Level of anxiety
The levels of anxiety before and after the intervention are presented in Table 2. Only 33.6% perceived a medium level of anxiety or above. While their anxiety level was generally low before the intervention, it was significantly lower following the intervention (t=3.28, df=102, p<0.005). (Department of Health, 33-55)
Changes of the participants’ knowledge of the three main transmission routes (droplets, direct physical contact, and urine/feces) before and after the intervention are presented in Table 3. A significant difference was found in their knowledge of droplet (p<0.001) and urine/faeces (p<0.005) transmission. Although no statistically significant change was found in the transmission route of direct physical contact (p>0.05), more participants answered correctly following the intervention (Department of Health, 33-55).
Discussion
Level of anxiety
Overall, the participants experienced low levels of anxiety at the time of baseline data collection. This may be due to geographic location among the participants who lived in an area with the least severe outbreak of SARS. Although their level of anxiety was low at both measurement periods, the mean total scores of anxiety were significantly lower after the intervention. More participants reported a low level of anxiety following the telephone intervention. These findings support those of (Department of Health, 33-55), who reported that the provision of care through telephone is an effective means to provide cognitive support to clients at home. (Department of Health, 33-55)
Implications
Although WHO removed Hong Kong from the SARS list in 23 June 2003, the possibility of another outbreak of SARS or other infectious diseases still exists. Recently, the Hong Kong Government emphasizes the importance of preparedness for influenza pandemic (Department of Health, 11-123) and healthcare professionals play a vital role to deliver health promotion and education to the public. It is, therefore, important that healthcare professionals understand how to deliver key health-related information to the public effectively, particularly to vulnerable groups such as senior citizens with low socio-economic status (SES) (Department of Health, 15-98).
In contrast to the general population, senior citizens in Hong Kong are comparatively socially isolated and have low literacy rates. Alternative methods of disseminating essential information to senior citizens are important to enable them to acquire updated information and take appropriate preventive measures to maintain health. E-health is an effective method for health education and promotion and many senior citizens are more likely to have access to information technologies such as telephone and television (Department of Health, 1-5).
Various consequences of the examination proved that that telephone health learning was very good in relieving anxiety and civilizing knowledge of the main broadcast routes of SARS in senior citizens, but not development carry out of stopping SARS. Therefore, the strategy that this study used could be helpful for the future development of health education and promotion for senior citizens. A combined measure, such as television health education and telephone follow up calls may be desirable to improve health behaviour practices, especially when dealing with possibly pandemics such as avian and other influenzas (Department of Health, 11-123).
Limitations
First, the senior citizens in this study were recruited from a district that was later reported to have the lowest infection and mortality rate of SARS among the 18 districts in Hong Kong. Therefore, generalization of the results to all senior citizens in Hong Kong is questionable. Furthermore, the study results indicated a low level of anxiety in the senior citizens, which could have resulted from living in a relatively “safe” district.
Second, the small sample size and a relatively short time period between the intervention and the follow-up may have resulted in the insignificant differences in the practice of preventive measures after the intervention (Department of Health, 44-87).
Third, the infection rate of SARS was gradually decreasing during the study period. The Hong Kong daily infection rate of SARS (Department of Health, 11-123) was about 3 cases per day during baseline data collection (Department of Health, 11-123), and it further declined to about 1 case per day during the 1-week follow-up. This could have affected the perceived importance of practicing the preventive measures since the overall risk seemed to have reduced as the epidemic was waning. Further follow-up could be useful in identifying sustainable changes of relevant behaviours and practices. (Department of Health, 90-123)
Fourth, although providing telephone intervention was the safest means to communicate with the senior citizens during the SARS epidemic, there were several drawbacks. For example, there is only limited amount of information that one can provide in a single telephone call. Thus, the interviewers have to balance the time spent on each call and to ensure the provision of adequate information for each respondent. It is not advisable to overload the senior citizens with too much information, as they may not be able to capture and remember all the contents in one single telephone call. Finally, the senior citizens might be exposed to other health education and preventive measures on SARS via television and other media during the outbreak. Therefore, it is difficult to attribute the positive changes solely to the interventions (Department of Health, 11-22).
Conclusion
In a nut shell we can say that telephone health learning was very fine in relieving anxiety and improving knowledge of the most important spread routes of SARS in this typical age group and Telephone call appears to be a realistic way of providing health learning to defenceless groups when face-to-face compute is not feasible and may be functional in raising health awareness all through future outbreaks of rising infections. (Department of Health, 11-22)
Actually it is the initial methodical study to assess the efficacy of telephone health learning in improving senior citizens ’ knowledge and carry out of preventive measures through the SARS epidemic. Our initial findings are encouraging in demonstrating the effectiveness of a telephone health education programme in relieving anxiety and improving knowledge of the main transmission routes of SARS in senior citizens. However, an effective intervention to change the embedded health behaviours remains to be established and tested. The use of technologies such as telephone appears to be an effective means to educate and provide social support to the vulnerable senior citizens during outbreaks of SARS and other possibly pandemic crises. Future research should explore the effectiveness of health promotion programmes using multiple information technologies that are accessible to, and appropriate for, senior citizens in changing their health behaviour practice (Department of Health, 11-22).
Appendix
a The test value and P value are determined by Student’s t test, χ2 test, or Mann–Whitney test as appropriate.
* P<.05 (two-tailed).
Table 2.Psychological and behavioural responses to SARS outbreak [n (%)]
References
Department of Health. NHS Executive, Finance Directorate. Primary Care Trust Revenue Resource Limits Exposition Book 2003-04 to 2005-06. Leeds: NHS Executive, 2001, 11-45
Department of Health. Reforming Emergency Care Strategy. London, Department of Health, 2001, 66-78
Department of Health. ‘Shifting the Balance of Power: The Next Steps’ 7.3 See 7.2; 33-55
Department of Health. Countering Fraud in the NHS. London: Department of Health, 1998.111-123
Department of Health. The Counter Fraud Charter. London: Department of Health, 1999.11-22
Department of Health. Modern Social Services – a commitment to reform (2002). London, Department of Health, 2002; 90-123
Department of Health. Social Services Performance Assessment Framework Indicators. London: Department of Health, 2002.44-87
Department of Health. The Removal, Retention and use of Human Organs and Tissue from Post-mortem Examination. London, Department of Health, 2001.1-5
Department of Health. Health Protection: A Consultation Document on Creating a Health Protection Agency. London, Department of Health, 2002;200-233
Department of Health. Departmental Investment Strategy: a summary. London: The Stationery Office, 1999 (Cm. 4324).15-98
Department of Health. Delivering the NHS Plan London: The Stationery Office, 2002
Clements, A, Henderson, BJ, Tyndel, S, Evans, G, Brain, K, A stoker, J, and Watson, EK 2002 (In press).
Diagnosed with breast cancer: the impact of women’s experiences on their views of participating in an early mammographic screening programme Eur J Cancer Care.
Woodrow, C, Watson, E, Rozmovits, L, Parker, R, and A stoker, 2002 J (In press). Public perceptions of communicating information about bowel cancer screening Health Expectations.
Bankhead, C (2007). Ovarian Cancer In: Cancer Diagnosis in Primary Care, ed. by Hamilton W, Peters TJ. Churchill Livingstone Elsevier, Edinburgh, chap. 10, pp. 105-111.
Clements, A, Watson, E, Rai, T, Bukach, C, Shine, B, and A stoker, J (2007).
The PSA testing dilemma: GPs’ reports of consultations with asymptomatic men. A qualitative study. BMC Fam Pract, 8(1):35.
Evans, R, Edwards, AGK, Elwyn, G, Watson, E, Grol, R, Brett, J, and A stoker, J (2007). “It’s a maybe test”: men’s experiences of prostate specific antigen testing in primary care. Br J Gen Pract, 57(537):303-10.
Evans, R, Elwyn, G, Edwards, A, Newcombe, R, Kinnersley, P, Wright, P, Griffiths, J, A stoker, J, and Grol, R (2007). A randomised controlled trial of the effects of a web-based PSA decision aid, Prosdex. Protocol. BMC Fam Pract, 8(1):58.
Evans, R, Elwyn, G, Edwards, A, Watson, E, A stoker, J, and Grol, R (2007).
Toward a model for field-testing patient decision-support technologies: a qualitative field-testing study. J Med Internet Res, 9(3):e21.
Feldman-Stewart, D, Brennenstuhl, S, McIssac, K, A stoker, J, Charvet, A, Hewitson, P, Sepucha, KR, and Whelan, T (2007). A systematic review of information in decision aids. Health Expect, 10(1):46-61.
Goldsmith, M, Bankhead, C, and A stoker, J (2007). Improving the quality of the written information sent to women about breast screening: Evidence-based criteria for the content of letters and leaflets NHS Cancer Screening Programmes, Sheffield. (ISBN: 978-1-844663-043-1).
Goldsmith, M, Bankhead, C, and A stoker, J (2007). Improving the quality of the written information sent to women about breast screening: Guidelines on the content of letters and leaflets NHS Cancer Screening Programmes, Sheffield. (ISBN: 978-1-84463-045-5).
Goldsmith, MR, Bankhead, CR, and A stoker, J (2007). Synthesising quantitative and qualitative research in evidence-based patient information. J Epidemiol Community Health, 61(3):262-70.
Goldsmith, MR, Bankhead, CR, Kehoe, ST, Marsh, G, and A stoker, J (2007). Information and cervical screening: a qualitative study of women’s awareness, understanding and information needs about HPV. J Med Screen, 14(1):29-33.
Gribble, SM, Kalaitzopoulos, D, Burford, DC, Prigmore, E, Selzer, RR, Ng, BL, Matthews, NSW, Porter, KM, Curley, R, Lindsay, SJ, Baptista, J, Richmond, TA, and Carter, NP (2007). Ultra-high resolution array painting facilitates breakpoint sequencing. J Med Genet, 44(1):51-8.
Henderson, BJ, Tyndel, S, Brain, K, Clements, A, Bankhead, C, A stoker, J, and Watson, E (2007). Factors associated with breast cancer-specific distress in younger women participating in a family history mammography screening programme. Psychooncology.
Hewitson, P, Glasziou, P, Irwig, L, Towler, B, and Watson, E (2007).Screening for colorectal cancer using the faecal occult blood test, Hemoccult.Cochrane Database Syst Rev(1):CD001216.
Martin, F, Camfield, L, Rodham, K, Kliempt, P, and Ruta, D (2007). Twelve years’ experience with the Patient Generated Index (PGI) of quality of life: a graded structured review. Qual Life Res, 16(4):705-15.
Rai, T, Clements, A, Bukach, C, Shine, B, A stoker, J, and Watson, E (2007).
What influences men’s decision to have a prostate-specific antigen test? A qualitative study. Fam Pract, 24(4):365-71.
Tyndel, S, A stoker, J, Henderson, BJ, Brain, K, Bankhead, C, Clements, A, and Watson, EK (2007). What is the psychological impact of mammographic screening on younger women with a family history of breast cancer? Findings from a prospective cohort study by the PIMMS Management Group. J Clin Oncol, 25(25):3823-30.
Webster, P and A stoker, J (2007). Does the English Breast Screening Programme’s information leaflet improve women’s knowledge about mammography screening? A before and after questionnaire survey. J Public Health (Oxf), 29(2):173-7.
Advisory Committee Breast Cancer Screen (2006). Screening for Breast Cancer in England: Past and Future. NHSBSP Publication 61. NHS Cancer Screening Programmes, Sheffield. (ISBN: 1 84463 026 9).
Bankhead, C (2006). Identifying potentially significant diagnostic factors for ovarian cancer in primary care: a qualitative and quantitative study. PhD thesis, University of Oxford, Oxford.
Bankhead, C, Collins, C, Stokes-Lampard, H, Kehoe, S, Clements, A, Mant, D, Wilson, S, Rose, P, and A stoker, J (2006). Identifying potentially significant diagnostic factors for ovarian cancer in primary care: a qualitative and quantitative study. Department of Health, Final Report.
Brown, J, Welton, NJ, Bankhead, C, Richards, SH, Roberts, L, Tydeman, C, and Peters, TJ (2006). A Bayesian approach to analysing the cost-effectiveness of two primary care interventions aimed at improving attendance for breast screening. Health Econ, 15(5):435-45.
Goldsmith, M, Bankhead, C, and A stoker, J (2006). Improving the quality of the written information sent to women about cervical screening: Evidence-based criteria for the content of letters and leaflets. NHSCSP Publication No. 26 NHS Cancer Screening Programmes, Sheffield. (ISBN: 978 1 84463 036 3).
Goldsmith, M, Bankhead, C, and A stoker, J (2006). Improving the quality of the written information sent to women about cervical screening: Guidelines on the content of letters and leaflets. NHSCSP Publication No. 27 NHS Cancer Screening Programmes, Sheffield. (ISBN: 978 1 84463 035 6).
European Observatory on Health Care Systems (2000) Health Care systems in Transition: Germany, Copenhagen: World Health Organisation.
Ferris, G., Roderick, P., Smithies et al (1998) An epidemiological needs assessment of carotid endarterectomy in an English Health Region. Is need being met? British Medical Journal 317: 447-51.
Filakti, H. and Fox, J. (1995) Differences in mortality by housing tenure and by car access from the OPCS Longitudinal Study, Population Trends 81: 27-30.
Fitzpatrick, J. and Kelleher, M. (2000) Geographic inequalities in mortality in the United Kingdom during the 1990s. Health Statistics Quarterly 7: 18-31.
Foster, P. (1996) Inequalities in health: what health systems can and cannot do. Journal of Health Services Research and Policy, pp179-82.
Frankel, S., Farrow, A. and West, R. (1989) Non-attendance or non-invitation? A case-control study of failed outpatient appointments. British Medical Journal 298:1343-1345.
Frankel, S., Eachus, J., Pearson, N. et al (1999) Population requirement for primary hip-replacement surgery: a cross-sectional study. Lancet 353: 1304-9.
Fraser, S., Bunce, C., Wormald, R. and Brunner, E. (2001) Deprivation and late presentation of glaucoma: case control study. British Medical Journal 322: 639-43.
GMS Working Group (2000) National Review of Resource Allocation. Report from the General Medical Services Working Group, unpublished report submitted to Sir John Arbuthnott’s Steering Group, 2000.
Goddard, M. and Smith, P. (1998) Equity of access to health care. Centre of Health Economics, York: University of York.
Goldman, L. and Cook, E.F. (1984) The decline in ischemic heart disease mortality rates: An analysis of the comparative effects of medical interventions and changes in lifestyle. Ann Intern Med 101: 825-836.
Goodchild, M. (1987) Spatial autocorrelation. Norwich: Geobooks.
Gordon, D., Davey Smith, G., Dorling, D. and Shaw, M. (1999) (eds) Inequalities in Health: The evidence presented to the Independent Inquiry into Inequalities in Health. Bristol: The Policy Press.
Gordon, D., Adelman, A., Ashworth, K., Bradshaw, J., Levitas, R., Middleton, S., Pantazis, C., Patsios, D., Payne, S., Townsend, P. and Williams, J. (2000) Poverty and social exclusion in Britain. York: Joseph Rowntree Foundation.
Gordon, D. and Townsend, P. (2000) (eds) Breadline Europe: The Measurement of Poverty. Bristol, The Policy Press.