Core Concept
The presented case describing the experience of Juan and his family is an example of how trauma can affect the mental health of the child and create severe problems for the relationship in the family. Based on the proposed situation, the boy who periodically remains with his father without the presence of his mother after the parents’ divorce begins to show signs of stress and frustration. Aggressive behavior, sleep problems, unhealthy sexual interest, and several other factors indicate that the child has challenges with socialization.
At one of his sessions with a therapist, Juan admits that his father acted as an unhealthy and sexual harassed him. After revealing the shocking truth, his mother, Mrs. Hernandez, notes that the father himself was subjected to a similar form of abuse in childhood. This example matches one of the 12 core concepts that interpret traumatic responses in families and children: “trauma experiences affect the family and broader caregiving systems” (“The 12 core concepts,” 2012, p. 4). The boy’s current family, as one of the most important caregiving systems, cannot provide him with adequate support due to the fact that the mother does not know about the shocking details of the father-son relationship. As a result, Juan shows signs of post-traumatic adaptation and stress caused by the abuse. According to his behavior, the abused child has mental problems that are manifested in the aforementioned symptoms. In addition, the experience affects other caregivers, including the child’s mother and preschool teacher, who also feel anxious. Therefore, the consequences of the trauma experienced are severe and influence different parties, which complicates the process of Juan’s socialization and his successful coping with stress.
Risk Factors
In the case under consideration, the proposed core concept concerning the consequences of trauma for the child and the implications on other caregiving systems is accompanied by specific risk factors. According to Lieberman and Knorr (2007), these factors can have individual, familial, community, and societal contexts. For instance, the authors cite examples of poverty, inadequate housing, and several other challenges that often exacerbate deviant behavior caused by past trauma (Lieberman & Knorr, 2007). In relation to Juan’s situation, all of these four categories of factors may be distinguished based on the background of the case.
- Individual. Firstly, the parents’ divorce is a factor that has influenced the boy’s psyche. Secondly, the described problems have caused disrespect for adults, which manifests itself in Juan’s relationship with his mother and teacher. Thirdly, the inability to express feelings and emotions due to unformed social skills complicates the therapeutic activity and successful care of the child. As Kellogg (2009) notes, unhealthy sexual behavior is a form of emotional distress. Finally, the boy has a hereditary predisposition to substance abuse, which is also a risk factor.
- Familial. Juan’s mother is a victim of domestic violence by her ex-husband. Due to the divorce, Mrs. Hernandez is experiencing financial challenges, which complicates the situation and limits the woman’s ability to provide comprehensive assistance to her son. Juan’s father, who appears to have had an unhealthy interest in the child, is prone to substance abuse and has a history of drug use. The father’s family had difficulties with immigration and faced refugees for political reasons. Finally, bilingualism promoted in the family may be a risk factor at an early age for a boy.
- Community. Juan’s tensions with peers due to the boy’s deviant behavior are a risk factor. In addition, his mother’s mistrust of Child Protective Services (CPS) complicates the situation and creates additional challenges. Moreover, the educational environment in which Juan studies is disloyal to the child’s behavior, and the boy’s psyche maybe even more threatened by pressure from the supervisory authorities.
- Societal. Increased control by the guardianship authorities and the involvement of the family in court proceedings complicate the process of restoring the child’s psyche. In addition, Mrs. Hernandez knows little about the legal aspects of custody and divorce, which hinders the successful litigation and clarification of the relationship between Juan and his father. Finally, refugee status leaves an imprint on the boy’s life and can be a sign of stigma in society.
The selected core concept suggests that the considered risk factors imply a close interaction between the experienced trauma and caregiving systems, which, in turn, requires comprehensive intervention to resolve the problem.
Supportive Factors
Supportive factors are incentives that can help overcome the current challenges caused by specific experiences. According to the idea one of the core concepts, these factors “buffer the adverse effects of trauma and its stressful aftermath” (“The 12 core concepts,” 2012, p. 4). For instance, as Lieberman and Knorr (2007) remark, supportive relationships can affect the psyche of children positively if the traumatic event happened once. However, in Juan’s case, the boy has reported a number of instances of abuse by his father, which exacerbates the situation. Therefore, guided by the same scheme as with risk factors, one should assess which supportive and promotive factors correspond to the case under consideration with the proposed core concept.
- Individual. Juan is physically healthy and has sufficiently developed cognitive skills. He seeks help from his mother, interacts with the therapist, and is able to express his thoughts, thereby simplifying the task for caregivers. The child is aware of the basic concepts of family and care and shows an interest in communication with peers.
- Familial. The boy receives support from his mother and from maternal grandparents. Mrs. Hernandez’s care and worrying about her son’s mental health are valuable supportive factors that can help address the current difficulties.
- Community. Despite the concerns of Juan’s preschool teacher, she supports the boy’s family and is concerned about his condition. The therapist is fully involved in the fate of the child and does everything possible to help the boy and find the cause of his behavior problems by identifying the traumatic experience. In addition, Juan has stable access to other healthcare professionals who are also willing to contribute to the normal socialization of the child.
- Societal. Although Juan’s problem is acute and deserves public attention, at the societal level, there are few supportive factors to help the child. The involvement of guardianship authorities in the boy’s life may have different consequences. Despite the rapid response of the responsible authorities to calls for help, the situation may turn out in such a way that Mrs. Hernandez might be held responsible for his son’s trauma.
While taking into account the considered core concept of the impact of trauma on caregiving systems, one can note that this concept allows identifying the main interested parties and their capacities to help. Juan demonstrates behavioral disorders that affect his family and peers, and targeted work carried out by adults is a valuable posttrauma adjustment mechanism.
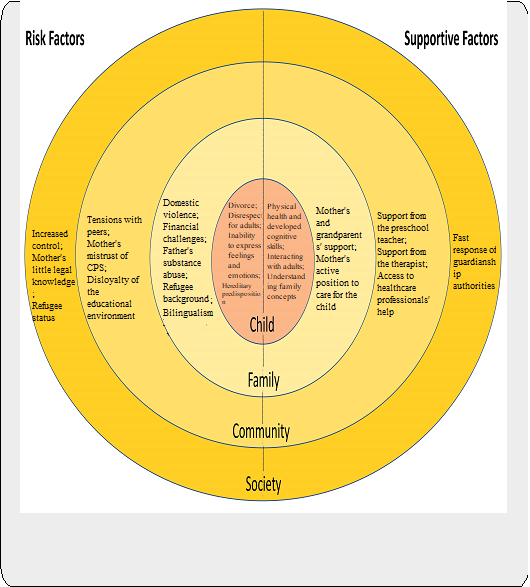
Protective Shield Factor Map
Based on the aforementioned risk and supportive factors, an appropriate Protective Shield Factor Map may be compiled. This diagram demonstrates which levels deserve addressing by comparing them, thereby identifying which ways to mitigate the existing problems are possible. In Figure 1, this map is displayed, and based on the core concept suggesting the impact of trauma on caregiving systems, one can conclude that many parties are involved, and Juan’s problem is acute.
Implications of Interactions Between the Risk and Supportive Factors
Knowing about risk and supportive factors at each system level presented in the Protective Shield Factor Map may help evaluate valuable implications. Lieberman and Knorr (2007) argue that abused children are more prone to behavioral disorders than children raised in a calm and healthy environment. By assessing the individual level in Juan’s case, one can highlight the main concerns of the boy to develop appropriate therapeutic intervention and address the existing gaps. At the familial level, the awareness of Juan’s obstacles and strengths may contribute to creating a supportive parenting environment and addressing negative impacts through effective childcare steps (Kellogg, 2009). Community factor analysis is a background to assess the existing incentives associated with Juan’s problem in his environment to assign stakeholder roles and use available resources (Lieberman & Knorr, 2007). Finally, at the societal level, the key task is to provide the child with socialization conditions free of bias and disloyalty by evaluating social stereotypes and developing a method for adapting the child to society. These steps are valuable decisions to implement due to the existing map of risk and supportive factors.
References
The 12 core concepts. (2012). The National Child Traumatic Stress Network. Web.
Kellogg, N. D. (2009). Clinical report – The evaluation of sexual behaviors in children. Pediatrics, 124(3), 992-998. Web.
Lieberman, A. F., & Knorr, K. (2007). The impact of trauma: A developmental framework for infancy and early childhood. Pediatric Annals, 36(4), 209-215. Web.