Introduction
One guarantee thatcannot be given to patients is that they will not be harmed by the system meant to look after them. Individual stories of suffering caused by the healthcare system are moving and can be terrifying. Recently, a shocking story that affected the lives of more than seven thousand dental patients in Oklahoma, USA reflects how unsafe healthcare practices can affect lives of many patients and their families. At least sixty people among patients who were tested were positive for hepatitis or Aids after visiting a dental clinic in Oklahoma, which was accused of poor sterilization methods (Williams 2013, p. 4). This shows only one of many incidences where patients were harmed, but the problem goes beyond those stories that hit the headlines. Many instances of iatrogenic harm that are not common exist.
In Dental practice, the possibility of unfavorable measures is present all through the process, involving, for instance identification, defective apparatus, all-purpose safety, and unfortunate communication with the patient or other health experts, insufficient disease management or ravage management. Decrease of unpleasant measures and enhancement of client wellbeing are most successfully realized through the process and precautionary action to trim down undesirable events. The dental occupation is dedicated to offering secure dental care, which is essential in guaranteeing high-quality general health, and aspires to reduce hazards and set up a culture of patient safety (Monteiro 2004, p. 3)
Cross infection is one of the severe problems that may impinge on the patient security in dental practice. The increased profile of infectious diseases arising from blood-borne viruses, such as human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV), has resulted in the detailed study of infection control (IC) procedures within dentistry. Following Infection control measures, such as the wearing of gloves, masks, and the autoclaving of hand pieces, have been reviewed regularly with additional recommendations continually being issued in the light of new scientific evidence (Kohn 2003, p. 14). Dentists are expected to take sufficient safety measures when handling this clients and staff as regards to the possibility of cross-infection. Failure to offer and make use of decontamination, disinfection, and sterilization conveniences may lead to actions related to professional misconduct.
One the most important infection control protocol in dental practice is Decontamination. It is an amalgamation of processes, including clean up, disinfection andsterilization, utilized in thestorage of a re-useable medical device safe for supplementary use (Krause, McDonnell, Riedesel 2001, p. 19). Today, decontamination is a topic of public healthiness since it is known that decontamination failures can result in a variety of infections. It is probable that in many cases of cross infections, cleansing has been a causative aspect. Therefore, effective decontamination can make an important contribution to decrease the prevalence of acquired infections (Creedon 2006, p. 317)
Nowadays, most of the healthcare systems consider disease prevention as an important aspect of healthcare across the world and identified education as an important aspect in the prevention and control of acquired infections. However, the degree of knowledge about IC guidelines does not necessarily predict appropriate behavior. Studies showed that guidelines alone frequently had a poor impact on Health Care Worker (HCW) knowledge and behavior. Therefore, education must be conducted in such a way that practices are modified appropriately (Kretzer&Larso 2008, p. 24).Many researchers observe that comprehensive intercessions based on behavioral hypothesis have more chance of success than solitary strategies or education agendas focusing on one or two components.
Aims and objectives
The present Change Project aimed to ensure a safety of the patient and staff by improving the knowledge and practice of dental assistants to IC standards regarding decontamination using a behavior change model.
The objectives of the project are:
- To increase dental assistants knowledge about decontamination practice in dental clinics
- To increase dental assistants compliance to the adopted key performance indicator of good decontamination practice
The writer’s organization
Six months ago, the writer designated asthe head of dental department in the Primary Health care centers in the emirates of RasAlkhaimah. Primary healthcare centers (PHCs) are one level in a network of different levels governed by the ministry of health (MOH) in the UAE.The centers provide services like family medicine, maternal health sciences, care of elderly together with dental services. The PHC dental clinics provide general and preventive dental treatment. There are 18 PHC centers in RasAlkhaiamah established since 1984, 15 of them are with dental services.The PHC serves a population of 231,000 people.The local statistics show that an average of 200 patients are seen monthly in the morning clinics shifts. Statistics for 2008 showed 12% increase in the number of clients visiting general practitioners at the centers with an average of three visits per person. The strategic plan from MOH is to improve continuously the quality and quantity of PHC services (Abcioglu 2000, p. 184). Data extracted from MOH reports indicates that UAE Nationals strongly prefer public dental facilities to private sector. That enforces the MOH to enhance and develop the healthcare safety system.
Rationale for the Project
In November 2013, the Infection Control Committee (ICC) in PHC conducted Auditing visits to all dental clinics.The purpose of the visit was to assess the level of compliance to IC standards. The results of the audit gave a clear indication that the decontamination practice was inadequate in some of the dental clinics. In general, decontamination according to HTM01-05 is the process by which reusable substances are made safe for further use and for workers to handle. It is expected to reduce the dangers of cross-infection between clients and between customers and workers. Decontamination involves several stages, including cleaning, disinfection, inspection, and sterilization. In order to achieve effective decontamination of the instruments, every stage of the process should be done thoroughly.
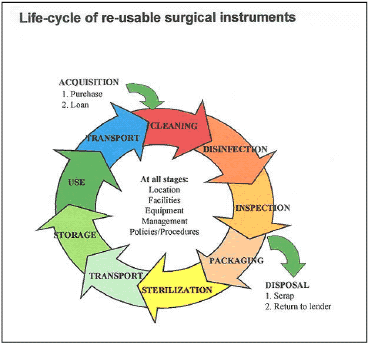
To understood decontamination amply, it requires precise accomplishment of all the measures talked about in the life cycle with appropriate controls and observations in place. Supervision and definite supplies relating to cleansing practice are accessible over quite a few years. According to the international guidelines, inadequate decontamination could be a source of cross infection and considered a potential risk that should be dealt with as a priority. Guidelines insist on adequate Cleaning followed by sterilization for all reusable instruments that have become contaminated with saliva, blood, or other biological fluids and should be cleaned and sterilized after use (Dawe 2009, p. 6).
Decontamination in Dental clinics in PHCs
In PHC, the cleanup of devices is mostly done using manual cleaning although studies showed using automated equipment can be moreproficient and safer (Bagg, Smith, Hurrell, McHugh & Irvine 2007, p. 12). All dental clinics in PHC use manual cleaning because of shortage in resources. Audit feedback showed that the manual cleaning process was generally poorly controlled practices. For example, the staff uses hand wash soap as a detergent to clean instruments. In addition, the range of disinfectors was used but without following the manufacturer instructions. Concerning the doctor’s security, the majority of those carrying out the work without putting on the protective eyewear to protect against splash, risk their lives. None of the medical staff had a magnifier accessible for examination of minute or complex devices or duty illumination for sanitation assessment. In more than half of the packaging area was not evidently separated out from the location where cleaning and disinfectionwere conducted. It is suggested that dirt free and unclean locations within the dental hospital should be obviously identified.Biological indicators were not used in PHCclinicsto check the effectiveness of sterilization cycle. Staff training in decontamination was provided mainly by lecture or training by a senior nurse, who already had not been trained sufficiently on decontamination guidelines.
Decontamination espoused in PHC is not being applied efficiently for two major reasons. The first is that the dental assistants are not trained effectively to follow the guidelines. The second is the lack of resource. For example, there is no supply with eyes protectors for securing staff from any injury during cleaning of the instruments.Also the brushes used to clean the instruments are old and not regularly changed.
Causes of poor compliance to decontamination good practice in PHC Dental clinics
The dental assistants are the one conducting decontamination in PHC dental clinics. Most of them are general nurses with no dental background. In a focus group meeting with the dental assistants, they mentioned several reasons acted as barriers to follow good decontamination practices. First, it is the lack of effective training on decontamination practices. The training given to the assistants was an orientation of one day by a senior nurse. Second, most of the staff complained from workload, which made it difficult for them to practice decontamination effectively. Finally, the lack of resources makes it hard for the staff to practice decontamination effectively. For example, detergent was not supplied to staff, which made them use hand wash soap to clean instruments. Regarding education and training, most of the staff’s opinion is that education through lectures and presentations are not enough for them to adhere to the best practice. They also complained that due to staff shortage, their managers would not allow them to attend educational workshop.
Summary
It can be concluded thatDental personnel has a responsibility of taking suitable safety measures to look after their clients and themselves from the danger of cross-infection. Failure to offer and employ enough cleansing, disinfection, and sterilization conveniences may lead to actions related to professional misconduct). To reduce the threat of transmission of infection among clients and between patients and Health Care Worker (HCW), a sensible and practical routine for the prevention of cross-contamination should be followed. Studies reveal thatmulti-dimensional interventions are required for IC Program success. Many of these documents have identified education as an important aspect in the prevention and control of infections. Indeed, education is critical since it enables a community to identify a disease. In addition, studies determine that to improve the Compliance of the HCW to IC guidelines, proper ways must be found to help them change their behavior or performance (Woodward 2000, p. 5).
References
Abcioglu, YH 2000, ‘Molecular evidence of nosocomial transmission of hepatitis C virus in a haemodialysis unit’, European Journal of Clinical Microbiology and Infect Disease, vol. 19.no. 3, pp 182-186.
Bagg, AJ, Smith, D, Hurrell, S, McHugh, S & Irvine, G 2007, ‘Pre-sterilization cleaning of re-usable instruments in general dental practice’, British Dental Journal, vol. 202.no. 2, pp 1-12.
Creedon, S 2006, ‘Infection control: behavioral issues for healthcare workers’, Clinical Governance: an International Journal, vol. 11.no. 4, pp 316-325.
Dawe, S 2009, ‘Decontamination of Re-usable medical devices policy’, NHS Foundation Trust, vol. 3.no. 1, pp 4-21.
Kohn, WD 2003, ‘Guidelines for Infection Control in Dental Health-Care Settings’, MMWR, vol. 52.no. 17, pp 1-16.
Krause, J, McDonnell, G &Riedesel, H 2001, ‘Biodecontamination of animal rooms and heat-sensitive equipment with vaporized hydrogen peroxide’,Contemp Top Lab AnimSci, vol. 40.no. 1, pp18-21.
Kretzer, RN &Larso, E 2008, Behavioral interventions to improve infection control practices, Free Press, Washington.
Monteiro, O 2004, ‘Patient Safety’, Council of European Dentists, vol. 2.no. 3, pp 2-7.
Williams, J 2013, ‘One confirmed hepatitis C infection in ongoing investigations of Tulsa dental office’, American Dental Association, vol. 1.no. 1, pp 1-6.
Woodward, CA 2000, ‘Strategies for assisting health workersto modify and improve skills: Developing quality health care – a process of change’, Center for Health Economics and Policy Analysis, vol. 3.no.1, pp 1-52.