Introduction
Health planning is a meticulous field for the application of planning principles, has concerns about access, equity, effectiveness, efficiency, and quality. Health service planning contributes to health gain in population as life betterment through accidents and trauma services, immunization, cancer treatments, supporting aged care, and many more. Planning for health services has become a vital part of policy formation for developed countries in order to satisfy the emerging needs of a growing population. Countries like Australia are developing new strategies to overcome the issues affecting health care such as changing epidemiology, aging population, demands of new technology, inequality, and the rising costs in health expenditure.
This assignment will be a basis for the development of health services plans for the new health authority – Cook Health that is the combination of New South Wales (NSW) & Queensland (QLD) states. Any health service primarily should monitor the incidence of infectious disease and act to control spread at the appropriate time. The planning and delivery of a health service is a tedious process. The planning team has the liability of ensuring the delivery of a quality health service like Cook health in a cost-effective manner. The planning team should meet the requirements of health service according to the defined policies and subject the procedures to approval and processing by funding agencies. Special funds and planning should be made for epidemic and large-scale disasters. “The HSP identifies NSW Health directions and policy requirements, HNE Health strategic directions and community needs, and describes the services to be provided in the future and how they will be provided” (Tamworth health services plan 2008-2012, 2008, p.9).
Currently, NSW and QLD have independent health services which provide a variety of state-wide and community services. NSW health services include 220 public hospitals, 500 community, children’s and family health centers, 220 ambulance stations, and a wide range of other services including aboriginal health, allied health, dental, mental health, and public health. Likewise, QLD is also successful in providing better health by creating trustworthy health care services.
Cook health authority should aim at providing appropriate medical support and rehabilitative services to NSW and QLD people. It should afford a distinctive approach to the care and treatment of residents and patients. Also, the Cook health strategies should help the elderly, disabled people, and people with chronic illness. Cook’s health strategic plan should focus on the promotion and protection of health including the prevention of ill health, obesity, smoking, and heavy drinking.
While planning Cook health services, the data including population, hospital types and their distribution, residential aged care centers, health professional’s – doctors & nurses availability, trends in Medicare needs to be analyzed to come to a conclusion thereby providing high quality, safe and sustainable health services to meet the needs of communities.
Population Statistics
Scalability of the health services is a very important factor. Resident population and migrant population is increasing every day which demands enhanced and robust services. “Population aging and growth will be the main drivers of demand for health services in the study catchment area, which will influence the mix and type of inpatient and ambulatory services required by residents over the next ten to fifteen years.” (New South Wales and Queensland joint planning study, 2007, p.2). The current population and projected population in age groups for each fifth year until 2025.
Table 1: Australian population in age groups till 2025
Hospital Statistics
In Australia, the number of public acute care hospital numbers grew from 712 in 1995–96 to 736 in 2005–06. The number of private self-supporting day hospital facilities increased from 140 in 1995–96 to 252 in 2005–06. The hospital segment includes more than 1,290 hospitals around Australia, with 82,000 beds. The model of an available bed is becoming less important due to increasing same-day hospitalizations and conditions of ‘hospital in the home’ care. Hospital bed numbers are affected by the range and types of patients admitted. As Cook is a combined state of NSW and QLD territories, the availability of hospitals and beds will be more. Hospitals can belong to either general hospital, causality, super-specialty, or multi-specialty. “Some of the key areas of patient flows from Queensland to New South Wales are for non-specialty medicine and surgery including cardiology and orthopedics treatment, gynecology, respiratory medicine, gastroenterology with the biggest inpatient inflow being for obstetrics.” (New South Wales and Queensland joint planning study, 2007, p.2).
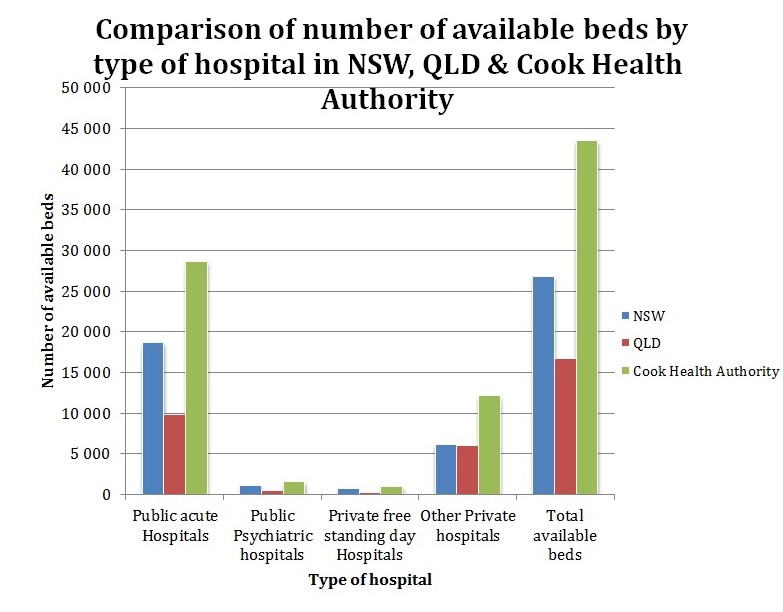
In 2006-07, the total number of Public Acute Hospital was 18,755 in NSW, 9,986 IN QLD that makes a total of 28,651 in Cook Health Authority. The Public Psychiatric Hospitals were 1,169 in NSW, 458 in QLD, and 1,627 in Cook Health authority. The Private free-standing day hospitals in NSW were 746, in QLD were 315 and in Cook, Health Authority would be 1061. It is evident from the graph that other Private Hospitals were 6,136 in NSW, 6,028 in QLD & 12,164 in Cook Health Authority.
Old Aged Statistics
“The proportion of older people who had received an enhanced primary care annual voluntary health assessment rose between 2001–02 and 2005–06.”
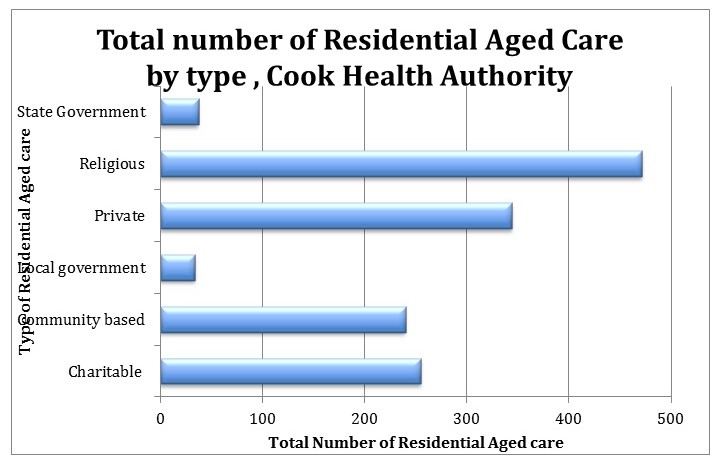
There are 470 religious Residential aged care facilities followed by 344 privately owned, 255 charitable, 240 community based, 37 state government, and only 34 are owned by local government.
Geographical Health Care Spread
Healthcare is a rising sector and there is 23% growth in Australia employed in health occupations between 2001 to 2006. Remote areas have less than half of medical practitioners and dentists’ supply compared with cities. The supply of general practitioners was about 9% lower in 2005 but in remote areas, the supply was 15% higher. Cook health service should design and implement plans in such a way that the general practitioners are available to remote areas people. “Comparing 2005 with 1997, the overall supply of primary care doctors (mostly general practitioners) was about 9% lower—but in remote areas, the supply was 15% higher” (Australia’s health 2008, 2008, p.408).
Government sops: Medicare Subsidy
The Government of Australia included a national subsidy scheme, Medicare which provides for free or subsidized treatment by medical practitioners, participating Optometrists, services by a nurse, certain diagnostic and therapeutic procedures, dentists, and allied practitioners. Medicare trend for consultations in the past is given below:
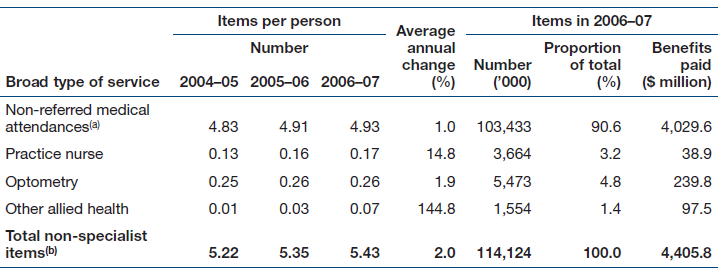
The above table includes general practitioner attendances, emergency attendances and attendances after hours, other prolonged attendances, group therapy, and acupuncture. In 2006–07, a total of $4,406 million was paid in Medicare benefits for non-specialist services, accounting for 38% of total Medicare benefits paid. Medicare also provides funds for medical specialist services. These services include specialists in private practice as well as medical services for private patients in public and private hospitals. “During 2006–07, an average of 6.5 specialist services per Australian were provided under Medicare.” (Australia’s health 2008, 2008, p.382). Cook health should educate people in their state about the Medicare policy so that they can be benefited from availing the services.
Recommended health facilities from the new unified services
Local governments usually contribute some of the funding for public and community health services. Cook Health services in new state ‘Cook’ should aim to provide a varied range of health services in NSW and QLD territories:
- District Health Service should focus on funds to rural communities for primary healthcare services of up to 5000 people.
- Countryside Health Service should focus mainly on funds to remote regions of NSW and QLD for primary care initiatives as an addendum to NRRHIP. “The National Rural and Remote Health Infrastructure Program (NRRHIP) aims to improve access to health services by providing funding to rural and remote communities where the lack of infrastructure is a barrier” (National rural and remote health infrastructure program, 2010, para.1).
- Maternal and Child Health Services should include parenting support services during antenatal and postnatal periods, early childhood attention programs, disease prevention, and treatment programs concerning child health and development. “Australia will also provide additional funding of up to $15 million over four years through UN agencies and NGOs for family planning and reproductive health activities to help reduce maternal deaths” (Smith, 2009, para.6).
- Aged Care Service should support older people to prevent disease and functional decline, extended endurance, and improve their quality of life. The program should work in harmony with Ageing, Disability and Home Care (ADHC) which is “committed to ensuring that older people, people with disabilities and their careers are valued, lead independent lives and have the opportunity to participate fully in community life” (About ADHC, n.d., para.2).
- Women’s Health Services should provide health promotion programs that help in. “increase the accessibility, sensitivity, and acceptability of health services for women” (Principles of Women’s health care, 2006, p.2).
- Men’s Health Service should focus mainly on promotional and educational programs
- Community Rehabilitation/Remedy Service should provide case management, prosthetic and equipment schemes, and home modification.
- Ambulance Services should focus on emergency pre-hospital patient care and transport in case of sudden illness and injury, rescue emergency patients, transporting patients between hospitals, perform road accident rescues and harmonize patient services in multi-casualty events.
Conclusion
Health services can be broadly categorized as public health services, primary care, and community health services, hospital services, and specialized health services. Cook Health is a public health service that would span across the two states robustly through proper planning based on existing and projected populations and conduct events, programs, or campaigns for health education, advising on lifestyle, controlling infections, monitoring of risk factors, and educating on unhealthy lifestyle choices. Cook Health can educate people on health issues in various sites like schools, colonies, and workplaces and also through media. Cook’s health should also focus on complements and alternative health care services such as acupuncturist, hypnotherapist, naturopath, and osteopath. With the above wide range of services, Cook health authority in the new state ‘Cook’ should provide state of the art health services both efficiently and effectively which would raise the bar for other health service agencies in Australia.
Reference
About ADHC. (n.d.). Human Services. 2010. Web.
Australian hospital statistics 2006. Australian Institute of Health and Welfare 2008, p.40. Web.
Australia’s health 2008. Australian Institute of Health and Welfare, pp.331-489. Web.
National rural and remote health infrastructure program. (2010). Australian Government, Department of Health and Ageing. Web.
New South Wales and Queensland joint planning study. (2007). NSW Health, p.2. Web.
Population projections. (2008). Commonwealth of Australia, p.44. Web.
Principles of Women’s health care. (2006). Women’s Health NSW, p.2. Web.
Residential aged care in Australia 2007. Australian Institute of Health and Welfare, p.39. Web.
Smith, S. (2009). Australian government committed to maternal and child health in developing countries. Australian Government, Media Release. Web.
Tamworth health services plan 2008-2012. Hunter New England, p.9. Web.