Abstract
The current research explores the notion of the universal health coverage from the perspective of business ethics and with references to comparing health care systems in the USA, Canada, and the UAE. The critical review of the previous research on the topic and the World Health Organization’s statistics was used as a method to examine the possible relationship between the governmental approach to distributing financial resources in the healthcare sphere, the population’s access to the care with the focus on poor people, and the patient health outcomes. It is found that the principle of the universal health coverage is fully adopted only in Canada. The USA started to reform the system in 2010, aiming at providing more citizens with healthcare services. The UAE is on the path to implementing the universal insurance as an alternative to the universal care in all Emirates.
Introduction
The universal health care is the goal for many governments in developed countries because the broader coverage is associated with positive health outcomes and decreased rates of deaths. When all citizens in developed countries have the access to the health care, the quality of life and its expectancy increase (Allin and Masseria 2; Fuchs 213). The purpose of this research is to examine the notion of the universal health coverage (UHC) in the context of business ethics and to compare the healthcare systems in the United States of America (USA), Canada, and the United Arab Emirates (UAE). It is important to examine the possible relationship between the governmental approach to distributing financial resources in the healthcare sector, the population’s access to the care, and the patient health outcomes. From this point, the research aims to provide the answers to questions about the general role of the universal care to affect health outcomes for patients and on approaches to implementing health care systems in three different countries.
Theoretical Framework and Topic Statement
The World Health Organization (WHO) discusses the universal health coverage as the main goal for healthcare systems in all countries, and the reason is in the necessity to provide the high-quality medical services to all categories of populations (World Health Organization 4). In this context, the UHC that is also known as the universal health care and the universal health system is the promotion of the equal access to healthcare services for all citizens, regardless of their financial status (Bennett, Ozawa, and Rao 1; Moreno-Serra and Smith 918). The broad health coverage is an important condition for different countries to guarantee that all citizens are adequately served in terms of their basic health needs (Kutzin 602). The UHC is discussed as the priority at the global level because today many poor people even in developed countries suffer from the lack of insurance to cover personal healthcare costs (Giedion, Alfonso, and Diaz 2). The idea of the UHC is based on the principle of providing the broad care services to all citizens, but the real situation is different, and the universal health care is adopted as the policy only in the limited number of states all over the globe.
Implemented health care policies are usually based on ethical norms and values that are related not only to the social sphere but also to the sphere of business. The reason is that the healthcare system develops according to business rules, and much attention should be paid to the correlation of costs and profits for public and private sectors of the healthcare system in a country. Therefore, the development of the healthcare system also depends on the utilitarian, egalitarian, libertarian, and democratic theories among others. The authorities following the utilitarian principles are inclined to evaluate the balance between costs and benefits translating advantages in monetary concepts, and the goal is the development of the most cost-efficient and beneficial system for the population (Mann 7; DeBoer 63).
Still, the idea of the UHC is not associated with this approach. The egalitarian theories associated with the idea of the equal distribution of services are more often referred to while discussing the UHC. Those authorities who propose both public and private healthcare services often use the libertarian theories that accentuate the right of an individual to choose any services. Ruger states that democratic theories are followed by the US authorities who propose the fair distribution of services according to the payment provided for the healthcare insurance (“Ethics in American Health 1” 1751; “Ethics in American Health 2” 1757). As a result, following different theories in discussing the idea of the universal health coverage, the state authorities promote multiple schemes for distributing medical services among the population.
Such developed countries as the USA and Canada have different approaches to providing health care services to populations. The approach utilized in the UAE differs from both the US and Canadian policies. Thus, the concept of the universal health coverage is not used in the USA because the main focus is on the healthcare insurance that is expected to cover medical costs of American citizens (Gorin 224). In the UAE, the idea of the universal healthcare system only begins to develop, and today the Emirates provide the wide range of free health care services for citizens, but the universal coverage is not accepted (Batniji et al. 344). Still, the most developed UHC is characteristic for the Canadian health system where the paid services include mainly dentistry and prescription of medicines (Siddiqi, Zuberi, and Nguyen 1453). Those countries that do not accept the UHC usually support their decision by stating that such coverage requires significant financial resources and spending (Savedoff et al. 922). Nevertheless, the researchers note that the universal healthcare system is not usually connected with significant costs if the country utilizes the effective finance spending mechanism.
The necessity to remove barriers to accessing the health care is discussed by representatives of the WHO as an important condition to address needs of the vulnerable population groups (World Health Organization 18). In this context, the lack of the access to the high-quality care is associated with violating human rights because the government is expected to address citizens’ needs regarding their well-being (Scott 17). The problem is in the fact that changes in the health status of the population depend on the access to health care services directly. The developed countries where more citizens are covered with free healthcare services often have the longer life expectancy (Savedoff 4). As a result, the consequences of non-providing populations with the universal health care can be dramatic, as the access of the poor people to medical services is limited in not only developing but also developed countries.
The questions that are related to the field of business ethics and aimed to be answered in this research are the following ones:
- What are similarities and differences in approaches of the USA, Canada, and the UAE to organizing the healthcare system and providing the universal health coverage?
- What are the universal health coverage and its role for people from the perspective of business ethics?
- What are similarities and differences in approaches of the USA, Canada, and the UAE to providing the expenditure on health?
- How should the health care be treated: as a right or a privilege?
- What is the connection between universal health coverage approaches and patient health outcomes?
- What are the consequences of the inefficient health coverage?
Referring to the determined research questions, it is necessary to find out how these countries’ approaches to the healthcare system can be explained from the point of business ethics. The problem is in the fact that the UHC is discussed by the WHO and other social organizations as an important condition to improve the health status of populations in developed countries. Still, these countries often avoid developing the universal health care system for their citizens because of such business ethics issues as the necessity to balance the health care costs and quality, high expenses of providing free medical services, the necessity to revise the insurance policy, and the need to cover large uninsured groups or poor citizens.
Methodology
The scope of the research was limited to discussing and comparing the approaches to realizing principles of the universal health care in such countries as the USA, Canada, and the UAE. In order to conduct the study on the topic and find answers to the determined research questions, the qualitative approach was chosen. The methods include the critical review of the WHO health and financing profiles for the selected countries and the review of the previous research on the topic to determine features of the healthcare systems in the USA, Canada, and the UAE.
First, the studies representing the discussion of different healthcare systems and approaches to promoting the UHC in the context of business ethics were searched. The peer-reviewed articles and reports were retrieved from Emerald, PubMed, ScienceDirect, ProQuest, and EBSCOhost databases with the help of such keywords as “universal care”, “coverage”, “expenditure”, “insurance”, “ethics”, “outcomes”, and their synonyms. The selected articles and reports discussed the topic from the perspective of business ethics referring to the correlation between financial and ethical elements of the health care coverage.
The second step was associated with searching the WHO website to retrieve Health Profiles and Health System Financing Profiles for the USA, Canada, and the UAE. The statistical data were properly examined for the further analysis and comparison of approaches used by the USA, Canada, and the UAE to organize their health care system and address the universal health coverage concept.
Results
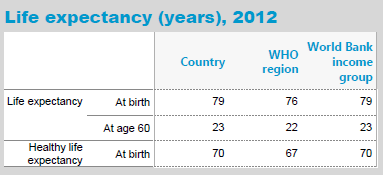
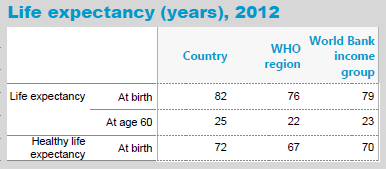
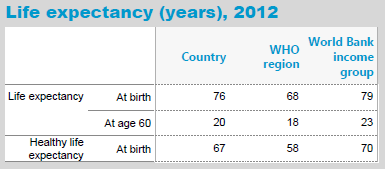
The data provided in the WHO Statistical Health Profiles for the USA, Canada, and the UAE indicate changes in the life expectancy and trends in the access to and utilization of the healthcare services in the countries. The data on the life expectancy in the USA are provided in Table 1. The data on the life expectancy in Canada and the UAE are provided in Table 2 and Table 3 accordingly.
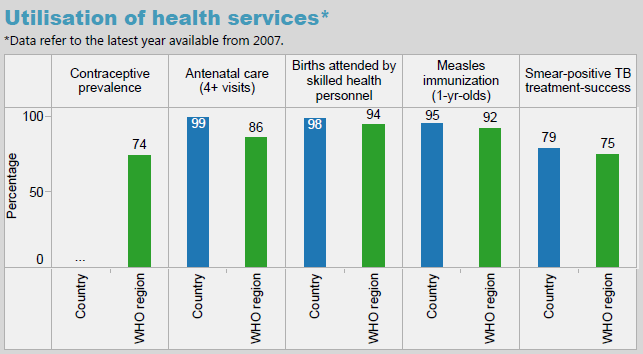
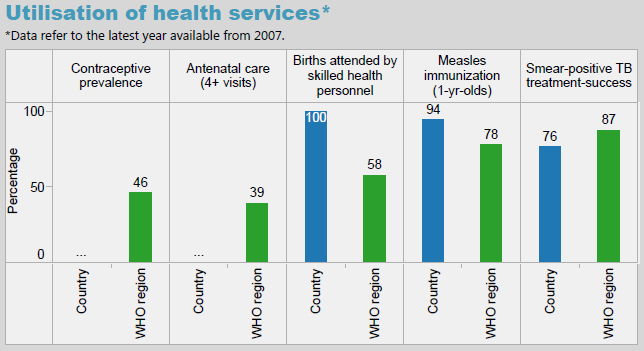
The data on the utilization of healthcare services for infants in the USA in 2007 indicates the difference between the access to the main services for pregnant women and for infants in the country and the WHO region. The data are presented in Figure 1.

The similar data are also available for Canada to represent tendencies of the families’ use of healthcare services in 2007, as it is provided in Figure 2.
For the UAE, the WHO data also provide the information on trends in accessing the basic healthcare services such as the antenatal care and measles immunization among others. The percentage is provided in Figure 3.
The additional statistical data on the health status of the populations in the USA, Canada, and the UAE, as well as the information on the governmental spending in the healthcare industry are presented in the WHO Health System Financing Profile. According to the WHO data, the USA spent more than $2,800 billion on the health care system in 2013 (WHO par. 8). In comparison, Canada spent $198 billion, and the UAE spent $13 billion in 2013 (WHO par. 10-12).
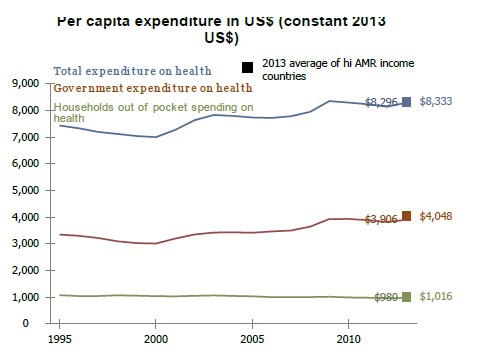
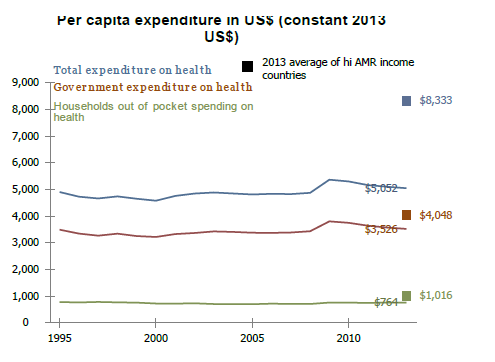
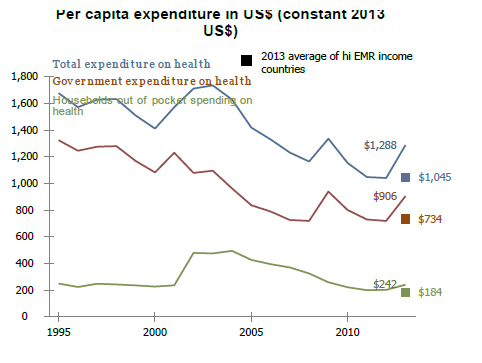
The WHO Health System Financing Profiles also provide the detailed information on the government expenditures in these countries. Figure 4 presents changes in the per capita expenditures of the US government on the health care during the period of 1995-2013. Figure 5 presents the similar data for Canada. Such data are also available for the UAE, and the information is proposed in Figure 6.
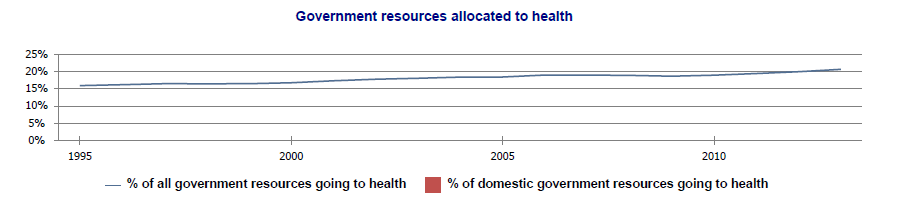
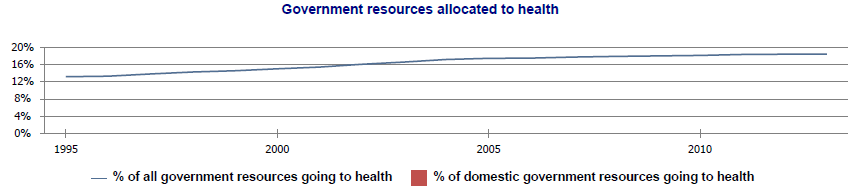
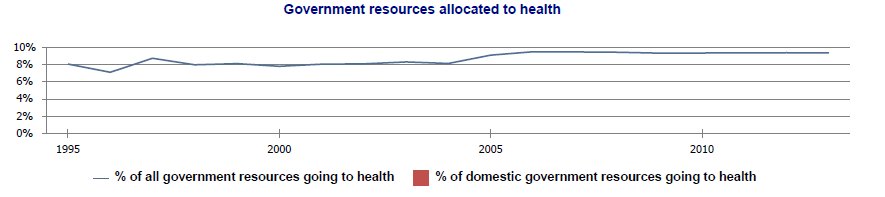
In order to understand the scheme of financing the healthcare system in the USA, Canada, and the UAE, it is necessary to refer to the percentage of the resources allocated by the government to the healthcare system. This percentage for the discussed countries is presented in Figure 7, 8, and 9 for the period of 1995-2013.
The probability of dying for individuals aged between 30 and 70 was 14% for both sexes in the USA in 2013. The causes included cancer, diabetes, heart diseases, and respiratory diseases. The probability for the Canadians was 11%. The probability for the UAE citizens was 19% (WHO par. 45-47).
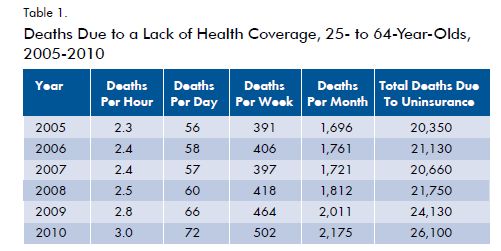
In addition, the reports on the healthcare insurance used in the USA provide the data according to which in 2010, there was about 50 million of uninsured Americans, and the lack of insurance led to increasing the number of deaths associated with the limited access to healthcare services in the USA during the period of 2005-2010 (Universal Health Care Foundation of Connecticut 4). Table 1 presents the data on deaths observed in 2005-2010 and connected with the lack of the health coverage in the USA.
These statistical data are important to be analyzed and compared with references to different situations in the USA, Canada, and the UAE in order to conclude on strengths and weaknesses of implementing the universal health coverage concept in these healthcare systems.
Discussion
The analysis of the previous research on the problem of the UHC in the world and in such countries as the USA, Canada, and the UAE combined with the analysis of the WHO statistical data allows concluding regarding the latest tendencies in adopting the universal health coverage concept in different contexts.
The Universal Health Coverage and Its Role
Having analyzed different approaches to promoting the universal health coverage, it is possible to state that the equal access of all citizens to the healthcare services is an important condition to speak about the effective system (Levesque, Harris, and Russell 19). One more required condition is the availability that means the provision of non-expensive services (Moreno-Serra, and Smith 918). Another condition is the high quality of provided services (Gray 1318). The problem associated with the UHC and related to the field of the business ethics is the issue of correlating costs and outcomes (Trotochaud 166).
Therefore, the UHC can be discussed as an appropriate policy when the quality of services is high, and costs are low, accentuating the cost-efficiency of the program. The provision of the universal care means that the gap between people’s needs for medical services and the actual utilization of these services is minimal (Kutzin 603). Thus, in the USA, the measles immunization is provided to 91% of infants, in Canada – to 95%, and in the UAE – to 94% of infants. The data demonstrate that the higher percentage is characteristic for countries where these services are mainly public. Those governments that focus on the idea of the UHC should not only provide free or public healthcare services but also guarantee their quality in order to make the coverage effective (Dalton et al. 2; Hurley 235). In this case, the role of the UHC is in improving the health status and outcomes for the population.
The Comparison of Healthcare Systems in the USA, Canada, and the UAE
Healthcare systems in the USA, Canada, and the UAE are quite different, and the UHC is provided to citizens only in Canada. In the USA, the UHC is guaranteed only for people who are aged over than 65 years (Siddiqi, Zuberi, and Nguyen 1453). However, in 2010, the Obama administration made significant steps in reforming the healthcare system in the country and adopted the Patient Protection and Affordable Care Act providing the mandatory health coverage for vulnerable categories of the American population. Still, the process of developing the system is rather challenging, and the access of the Americans to the care remains to be dependent on the insurance mechanisms, including the employment-based and family insurance types (Dalton et al. 3).
In Canada, the idea of the universal healthcare system is followed strictly. The public services are available to each citizen, and they do not cover the dental and vision care, as well the prescription of medicines. Thus, both private and public care services are proposed (Siddiqi, Zuberi, and Nguyen 1454). In the UAE, the approach to providing the universal care differs from both the US and Canadian strategies. The main focus is on providing the universal insurance for all citizens in the Emirates. This policy is effectively implemented in Abu Dhabi, it is developing in Dubai where more people continue to receive the medical insurance, and this approach is applied to other Emirates (Batniji et al. 345). Having both public and private healthcare facilities, the UAE authorities focus on the provision of the mandatory insurance for people living and working in the country (World Health Organization 8).
From this point, the life expectancy is an important indicator to demonstrate how the regular and easy access to healthcare services can influence the duration of the individual’s life. In the UAE, the age is 76 years, and this figure is the lowest in comparison to the measures of the USA and Canada, and the Canadians have the longest life (82 years). It is possible to state that the Canadian health care system contributed to improving the access to health services for all citizens regardless of their income status, and this fact can explain the high life expectancy in the country (Siddiqi, Zuberi, and Nguyen 1453).
The Expenditure on Health in the USA, Canada, and the UAE
The expenditure of the US government on the health care system is comparably high, and it was 21% in 2013. In Canada, the share of the spending is lower, and it is only 18% in relation to the overall governmental spending in 2013. The lowest percentage is typical of the UAE, and it is only 9% (WHO par. 17-19). It is characteristic for the USA to have the higher governmental spending in contrast to the regional averages because of high administration costs. The UHC can become the reality for the USA if the authorities focus on reducing administration costs and addressing the problem of rising medical costs during the periods of economic crises (Bailey 8).
It is also important to note that the government expenditure on health per capita is almost equal in the USA and Canada (more than $3,900 and more than $3,500 accordingly). The lowest expenditure is typical of the UAE (over $900), but it is higher than the average expenditure in the region (over $700). As a result, it is possible to state that the US and Canadian governments spend almost equal resources on supporting the health of their citizens, and there are opportunities for developing the universal health coverage concept in relation to the USA. When the per capita expenditure is high, it is possible to expect increases in the life expectancy.
Health Care as a Right and a Privilege
The discussion of the health care as a human right is a matter of debates because those countries that adopted the universal health coverage concept are regarded as supporting this right. On the contrary, those countries that refer to the public and private insurance to cover the health care costs seem to ignore the idea of the universal care (Baily 4). In case of the USA, those citizens who have no resources to pay for insurance are at risk of death because of diseases, and this approach can be discussed as unethical according to the United Nations’ Universal Declaration of Human Rights and the statement regarding people’s rights for an adequate standard of living and health (Hurley 235; Mann 8).
From this perspective, the universal healthcare is not a privilege, and each person should have the right to receive the adequate medical assistance. In this context, uninsured people are deprived of the right to be treated equally to those persons who can pay for the insurance (Bailey 4). In Canada, the health care is available for each person, and the human right to have the high-quality services is emphasized. In the UAE, the analogous limited approach is planned to be overcome with the focus on the provision of the mandatory insurance for all people in the country to avoid making the care a privilege.
The Connection between Universal Health Coverage Approaches and Patient Health Outcomes
In spite of the fact that the USA distributes about 20% of its total spending on the healthcare system, the rate of uninsured citizens is significant, and this fact explains why the probability of dying is still high in the country for persons aged 30-70 years (14%). However, this percentage is even higher in the UAE, where 19% of individuals are at risk of dying from cancer, diabetes, and heart and respiratory diseases. The lowest percentage is characteristic of Canada (11%). From this point, the UHC can directly lead to reducing the possibility of dying associated with the severe diseases requiring the constant monitoring and high-quality healthcare services (Kutzin 603). When more citizens have the access to the affordable health care, the patient health outcomes also improve (Levesque, Harris, and Russell 19).
Consequences of the Inefficient Health Coverage
The high percentage of persons dying from cancer, diabetes, and heart or respiratory diseases in states is usually discussed as the main negative consequence of the inadequate health coverage. In case of the USA, the problem is in the lack of insurance for all categories of the population. In 2010, the number of persons dying because of the lack of insurance coverage was more than 26,100 people, and in 2009, it was 24,130 people (Bailey 2). From this point, the absence of adequate and widely supported reforms in the healthcare system of the USA leads to increasing the number of annual deaths associated with the lack of the UHC (Savedoff et al. 925). Those poor people who cannot afford the insurance often suffer from severe diseases causing the epidemic situation in the country (Savedoff et al. 926). Such problem is observed in the UAE, where the authorities aim to address this social and ethical question while providing the universal insurance.
Recommendations
Referring to the experiences of the USA, Canada, and the UAE in addressing the idea of the universal health coverage, it is possible to state that both the USA and UAE have the potential to improve the population’s access to the health care. Recommendations to change the situation in terms of the business ethics should be the following ones:
- The governments of three countries should revise their approaches to distributing resources and budgets on covering healthcare services with the focus on prepaid funds.
- To achieve the higher positive outcomes in relation to the population health statuses, it is important to increase the pooled health funding.
- The USA should develop programs associated with the Patient Protection and Affordable Care Act to provide more vulnerable individuals with the access to the high-quality care while increasing the governmental expenditure per capita.
- The UAE should continue developing the strategy in terms of providing the mandatory insurance to guarantee the universal coverage.
- The Canadian government should focus on improving the quality of public healthcare services.
Conclusion
It is found that the universal health coverage based on the idea of the equal access to healthcare services is fully adopted only in Canada. The government aims to balance costs associated with the public care and its quality addressing basic needs of the population and primary ethical questions. The government in the UAE also accepts the necessity of the universal health coverage to address the citizens’ needs. Still, using the limited resources, the authorities implement the policy in separate Emirates while focusing on the provision of the mandatory insurance. In the USA, the situation is most challenging because the country is traditionally discussed as lacking the universal care. The only steps made to reform the system and increase the positive patient outcomes are associated with the Patient Protection and Affordable Care Act adopted in 2010. The reason is in the fact that the Act guaranteed more free health services for more Americans.
Works Cited
Allin, Sara, and Cristina Masseria. Research Note: Unmet Need as an Indicator of Access to Health Care in Europe. 2009. Web.
Bailey, Kim. Dying for Coverage: The Deadly Consequences of Being Uninsured. Washington: Families USA Publishing, 2012. Print.
Baily, Mary. The Ethics of Using Q1 Methods to Improve Health Care Quality and Safety. New York: The Hastings Center Publishing, 2008. Print.
Batniji, Rajaie, Lina Khatib, Melani Cammett, Jeffrey Sweet, and Sanjay Basu. “Governance and Health in the Arab World.” The Lancet 383.9914 (2014): 343-355. Print.
Bennett, Sara, Sachiko Ozawa, and Krishna Rao. “Which Path to Universal Health Coverage? Perspectives on the World Health Report 2010.” PLOS 7.11 (2010): 1-4. Print.
Dalton, Andrew, Eszter Vamos, Matthew Harris, Gopalakrishnan Netuveli, and Robert Wachter. “Impact of Universal Health Insurance Coverage on Hypertension Management: A Cross-National Study in the United States and England.” PLOS One 9.1 (2014): 1-12. Print.
DeBoer, Michael. “Legislating Morality Progressively-The Contraceptive Coverage Mandate, Religious Freedom, and Public Health Policy and Ethics.” Journal of Law and Health 28.1 (2015): 62-120. Print.
Fuchs, Victor. “Ethics and Economics: Antagonists or Allies in Making Health Policy?” Western Journal of Medicine 168.3 (1998): 213-230. Print.
Giedion, Ursula, Eduardo Andres Alfonso, and Yadira Diaz. The Impact of Universal Coverage Schemes in the Developing World: A Review of the Existing Evidence. Washington: The World Bank, 2013. Print.
Gorin, Stephen. “Universal Health Care Coverage in the United States: Barriers, Prospects, and Implications.” Health & Social Work 22.3 (1997): 223-230. Print.
Gray, Jeremy, Christopher Millett, Sonia Saxena, Gopalakrishnan Netuveli, and Kamlesh Khunti. “Ethnicity and Quality of Diabetes Care in a Health System with Universal Coverage: Population-Based Cross-Sectional Survey in Primary Care.” Journal of General Internal Medicine 22.9 (2007): 1317-1320. Print.
Hurley, Jeremiah. “Ethics, Economics, and Public Financing of Health Care.” Journal of Medical Ethics 27.4 (2001): 234-239. Print.
Kutzin, Joseph. “Health Financing for Universal Coverage and Health System Performance: Concepts and Implications for Policy.” Bulletin of the World Health Organization 91.8 (2013): 602-611. Print.
Levesque, Jean-Frederic, Mark Harris, and Grant Russell. “Patient-Centred Access to Health Care: Conceptualising Access at the Interface of Health Systems and Populations.” International Journal of Equity Health 12.1 (2013): 18-24. Print.
Mann, Jonathan. “Medicine and Public Health, Ethics and Human Rights.” Hastings Center Report 27.3 (1997): 6-13. Print.
Moreno-Serra, Rodrigo, and Peter Smith. “Does Progress Towards Universal Health Coverage Improve Population Health?” The Lancet 380.9845 (2012): 917-923. Print.
Ruger, Jennifer Prah. “Ethics in American Health 1: Ethical Approaches to Health Policy.” American Journal of Public Health 98.10 (2008): 1751-1756. Print.
—. “Ethics in American Health 2: An Ethical Framework for Health System Reform.” American Journal of Public Health 98.10 (2008): 1756-1762. Print.
Savedoff, William, David de Ferranti, Amy Smith, and Victoria Fan. “Political and Economic Aspects of the Transition to Universal Health Coverage.” The Lancet 380.9845 (2012): 924-932. Print.
Savedoff, William. A Moving Target: Universal Access to Healthcare Services in Latin America and the Caribbean. Washington: Inter-American Development Bank, Research Department, 2009. Print.
Scott, Charity. “Belief in a Just World: A Case Study in Public Health Ethics.” Hastings Center Report 38.1 (2008): 16-19. Print.
Siddiqi, Arjumand, Daniyal Zuberi, and Quynh Nguyen. “The Role of Health Insurance in Explaining Immigrant versus Non-Immigrant Disparities in Access to Health Care: Comparing the United States to Canada.” Social Science & Medicine 69.10 (2009): 1452-1459. Print.
Trotochaud, Karen. “Ethical Issues and Access to Healthcare.” Journal of Infusion Nursing 29.3 (2006): 165-171. Print.
Universal Health Care Foundation of Connecticut. Uninsured: The Costs and Consequences of Living without Health Insurance in Connecticut. New York: UHC Foundation of Connecticut, 2005. Print.
WHO. World Health Organization: Countries Profiles. 2015. Web.
World Health Organization. Arguing for Universal Health Coverage. Geneva: WHO Publishing, 2013. Print.