Introduction
Application of local anaesthetics has prime importance in pain control and effective management of patients while dealing with dental care. This is because its use is very safe and convenient. The key contemporary practice of dentistry is to manage pain and apprehension. Patients who really are afraid of dental treatment and also those who face the medical prognosis of a bitter and perhaps stressful process justly anticipate that the alternatives of conscious sedation should have potential to assist them.
Conscious sedation is
1-6 A technique in which the use of a drug or drugs produces a state of depression of the central nervous system enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation. The drugs and techniques used to provide conscious sedation for dental treatment should carry a margin of safety wide enough to render loss of consciousness unlikely.
It is used for medical procedures in which the frozen individual can react to verbal guidance of the dentist. However, the patient does not feel any pain, and at the same time acquires a transformed level of cognizance. This type of sedation is used when it is essential for a patient to be reactive, and also for minor operations which does not require the use of general anaesthesia. It can also be used with the patients who do not co-operate with care providers.1
Indications for sedation
The indications for sedation in dental patients are mainly categorised as their psycho-social behaviour, potential to medical and dental treatments. They can be identified as phobias, anxieties, inability to take medicines intra-orally, frequent fainting while undergoing procedures, idiosyncrasy to local analgesia, hypertension, epilepsy, asthma, ischemic heart disease, spasticity disorders etc. Some other factors for sedation are physical disabilities, and oral surgery procedures like exodontias and implants. Certain systematic problems seen in the patients are also considered as indications to sedation while in the handicapped it is exodontias and restorative. 7
There are different types of sedation methods that are applied in adults and children. They are oral sedation, inhalation sedation, intravenous sedation and transmucosal sedation. In transmucosal sedation oral, nasal and rectal administration are done conveniently according to the level of anxiety and phobia in patients. Such applications and administering the medicines are in accordance with the general stature of the patients. Special attention is given to physically challenged patients and to those who are suffering from learning problems and mental disorders.7-12,
Risk factors
In spite of what is said above, drugs that suppress the nervous system cause some effects. If small doses are given, it will bring about light sedation. The patient is conscious in this state but the anxiety is well removed. But with an increased dose added by other drugs will cause major depression in the central nervous system creating deep sedation. When the consciousness is gone, the light general anesthesia will start to work which can be deepened by the administration of additional drug. In this regard it would be interesting to note that a population-based study conducted in UK recorded 1:250,000 as mortality rate in the administration of general anesthetic during 1970-1979. This reveals that any treatment using local anesthesia is less risky than the general anesthesia. It is assumed that if anesthesia is given for a longer period it will result in greater morbidity and mortality rate. Therefore, when depressant drugs for conscious sedation are applied careful titration and monitoring are required to ward off unexpected deep sedation in the patients. Though the risk factors are less in conscious sedation, the safety of the patients is resting with the dentists in their selection of the drug and clinical judgment to cope with the problems of anxiety and pain control.8
The provision of adequate control for anxiety is an essential component to the practice of dentistry. The General Dental Council has suggested that control for anxiety is both a right for the patient and a responsibility on the part of the dentist.1 All patients are worthy of appropriate anxiety control for any dental procedure. The methods must be selected considering the welfare of the patient undergoing the specific treatment. To identify a single method to all patients is not appropriate; a range of alternatives have to be provided. It is crucial that a broad scope of security between conscious sedation and the unconscious state rendered by common anaesthesia is observed. Verbal, touch and defensive reflexes have to be maintained in conscious sedation in contrast to the total communication loss in general anaesthesia. Needless to say, there has occurred a solid transformation in the provision of anguish and nervousness management in dentistry in the UK, since 1998. This has led to an improved stress on the protected provision of conscious sedation rather than relying on general anaesthesia. 1
General anaesthesia can be used only in response to clinical needs. The publishing of ‘A Conscious Decision’ in 2006 ended in the surcease of general anaesthesia for dentistry which was put into force in Scotland from April 2001.1 General anaesthesia makes a patient unconscious for a long period and it is only practiced in surgery cases. In dentistry it is less applied as it may bring in complications in the patients. Local anaesthesia blocks the feeling from the intended body part and eliminates pain during the dental procedures. The sedation techniques adopted in dentistry are intravenous sedation, inhalation sedation, oral sedation and transmucosal sedation. In transmucosal sedation oral, nasal and rectal mode of administering the drugs are practised. Pharmacological agents such as Diazepam, Midazolam, Propofol, Nitrous Oxide, Servoflurane and Lorazepam are the drugs used for conscious sedation in dentistry. 8, 9
It is true that there are some side effects linked with conscious sedation. Several instances of nauseous feeling were reported by patients after the sedation recently. Sometimes they may feel sick on waking up from their sleep. It may also cause headaches to a few patients. In such cases it does well if nutritious fluids are taken in immediately after the conscious sedation. If the side effects prolong for a considerable period the fact should be brought to the notice of the doctor without any delay. 8, 9
In the medical commune, arguments with regard to conscious sedation still persist. There were instances of unwanted usage of sedation methods in the patients. It has to be noted that the drugs should be applied very cautiously to assure that the patient is sedated, but not to make them comatose. Dentistry Organisations have precise thumb rules about conscious sedation which they continuously advocate to their members. 8, 9
Anxiety as a factor for conscious sedation
Patients with wide variety of anxieties often visit a dentist. These fears stem in them either due to experiences of their own or of a member in their family. Such anxieties may link to needle phobias or to particular sounds or even feelings of the dental office. Even though the pain by itself may be the most important factor for anxiety to the patient, other causes may also add to their fears. The oral cavity is an extremely innervated structure and is sometimes described as the main “emotional centre” of the body.7-16
To overcome anxiety in the patient a dentist uses conscious sedation, which is a form of drugging by which a patient stays conscious with all the defensive reflexes held together. These exhibit unharmed laryngeal and pharyngeal reflexes and also the homeostatic respiratory and involuntary nervous system. 7-16
The main objective of using conscious sedation by dentists is to change the mood of the patient resulting in his/her reaction to pain which might ensue in achieving enhanced acceptance of dental treatment. This mode of sedation might help the patient to respond to the commands of the dentist and forces them to be co-operative, thereby providing a level of memory loss or “telescoping” of time. 5, 7, 8, 11, 23, 40
Methods of sedation used
Inhalational sedation
The success of the technique reckons on apt titration of nitrous oxide to the individual patient’s reaction and is backed up by behaviour direction techniques. Committed inhalation sedation mechanisms do not permit hypoxic degrees of sedation. Inhalational sedation has a conventional part in dental practice and can be made use of more commonly in other circumstances. Nitrous oxide has both tranquilising and analgesic actions. It can also be measured quickly and at the same time have an evenly rapid healing time and few side effects. It has to be used by mixing it with oxygen which might provide only extra benefit. The effectiveness and security of nitrous oxide/oxygen mixes are shown by its long use in dentistry. Nitrous oxide as a sedative is also applied extensively in the Accident & Emergency Department10 and preliminary work has established that it can be utilised efficaciously for pliable sigmoidoscopy. 11 Nitrous oxide and intravenous midazolam are effective for the majority of patients and have an excellent protection record.
Intravenous Sedation
Intravenous sedation is generally attained by the shot of a single drug. Apart from this, there are a number of other techniques practiced by some healthcare pros. They may use a blend of sedative drugs or intravenous sedative(s) with either inhalation or oral sedation. A variety of these systems have been used productively within randomised controlled tests to furnish conscious sedation of dental patients9-26. The success of intravenous sedation is straightaway linked to titration of the dose based on the individual patient’s requirements and so the application of preset doses or bolus techniques is undesirable 27.
Oral Pre-medication
The function of oral pre-medication is to assist the patient’s fear management prior to the actual treatment, and is not in reality a perfect sedation technique. Oral pre-medication along with a small dosage of benzodiazepine can be prescribed to help in sleeping. This may be used the night before the treatment or to help an anxious patient’s travel under close superintendence for treatment. Patients who are supposed to get oral pre-medication must obtain suitable pre- and post-operative directions.27-29
Oral and Transmucosal Sedation
Sedation may be attained by the oral or transmucosal administering of benzodiazepine. The pharmacokinetic feature of midazolam gives the medication the most preferred alternative28, 29. It has been seen that quite a few small randomised assured trials of midazolam delivered orally or intranasally to provide conscious sedation for alveolar patients is both safe and helpful 30-33. These techniques are used only when the titrating techniques are found to be unsuitable.
Dental implants
The provision of dental implants changed the dental practice in UK. It revolutionized the replacing of lost teeth. There is dependability and also has predictability about the success of the dental procedures. However, the resources of National Health Services are very limited and the number of patients referred for NHS-funded and NHS oriented implants in much higher than the available resources. Therefore, to combat the situation, the Royal College of Surgeons of England issued the Guidelines for the selection of deserving patients for dental implants by NHS.34-38
In implant therapy the ‘tooth’ is permanently attached to the jaw. The dentists evaluate the problem of the patients and refer them for dental plate or implants. Implants have the advantage of a natural look and they more or less look as if they are natural teeth. Implant dentistry is conducted in two stages – surgery and restoration. Normally, a prosthodontist does the restoration work but sometimes some dentists do both. A dental implant is basically a process whereby a screw is laid into the jaw and to this a cap is fastened. Sometimes implant failures arise if the dentist does not notice insufficient bone support while fixing the screw.34-38
More and more patients are now seeking a long term solution to replace the lost teeth and dental implant is the nearest procedure that one can find. The time taken for a dental implant surgery depends on the work that has to be done. All procedures are performed under local anaesthesia. This ensures that the patients undergo a relatively pain free process. The dental implant process is done in stages lasting from 3 to 6 months in many cases. It is not an overnight procedure. Average cost of an implant is about £2000, which is a huge amount for a layman. But the long term benefits outweigh the costs. However it depends on the type of dental implants that are required. 34-38
Dental implants are created with the help of commercially and medically unadulterated Titanium. Advantages of such implants are:
- Changed capacity to chew and speak correctly
- Regaining of facial aesthetics
- Conservation of continuing jaw bone structure
- Lessening of likely gum troubles and infections
These and many other constituents relating to dental care and the effective application of sedation methods to avoid pain and anxiety in patients are analysed in this research paper. The effectiveness of such methods is appraised with a critique’s approach by comparing the methods adopted by the different departments under dentistry. The study is thus departmentalized and is given under separate chapters excluding what is stated in the previous pages under this very Introduction part. They are:
- Methodology. It is the application of research methods. It contains the description and reasoning of the research methods applied to, including data collection, and how it has been collected. A brief analysis of data collection method is also given here.
- Literature review, wherein a review of the data collected is provided
- Summary, which carries a short account of the residual outcome of the review.
- Analysis of the research
- Discussion of the findings with regard to the contents of the previous chapters.
- Conclusion. It gives a clear interpretation of the problems and offers solution to them.
- Recommendations to the furtherance of remedial measures are covered in this chapter.
Methodology
Research Method
There are several sources available over the Internet about research methods that are applicable to academic studies of this nature 1, 2. The Economic and Social Research Council (ESRC) defines research methods as follows:
Research is the application of systematic techniques and methods in pursuit of answers to questions. These questions and answers can be highly specific, or abstract and general, depending on the type of research being undertaken, from basic to applied ones.3
Therefore, the research project about Conscious Sedation Methods Used for Adults in Dentistry is identified as an applied research study. However, Davison and Vogel state that research philosophy is a conviction about the manner in which data should be collected, examined and applied. 4, 5 It involves the compilation and examination of information based on its quality and not quantity. They use un-constructed logic to unscramble the significance of research. Qualitative methods are frequently denoted to as being subjective, 6 while quantitative methods are research methods concerned with numbers and anything that is quantifiable. They are distinguished from qualitative methods. 7
The present research approach about Conscious Sedation Methods Used for Adults in Dentistry is typically designed for the practitioners who analyse the data to improve their practice. 8 Therefore the study is completely observational. Also to get the desired results clinical trial study is also adopted on par with the observational study. Comparative studies on the performance of different drugs in each technique applied are necessary to know the sedation quality of the drugs.
Data Collection
The primary data will be collected through different studies and an analysis will be conducted. The quantitative data will be subjected to statistical analysis. Secondary data will be gathered by other means like questionnaires. An extensive search will be undertaken to gain a comprehensive understanding of the role of Conscious Sedation Methods Used for Adults in Dentistry in general. It will also be used to identify the extent to which conscious sedation strategy leads to customer satisfaction.
Data collection procedures
Information for the conduct of this study has been retrieved chiefly from books, journals, governmental agencies, dentistry organizations and study group’s reports. Dentistry guidelines and policy documents and recommendations were also collected and reviewed. Internet sites such as National Electronic Library for Health Guideline Finder, Medline, Cochrane Library, Wiley inter-science, Ovid etc., were visited for study materials to address the research questions.9
Research Design
A comparative and cross-sectional design will be used to enable a collection and comparison of data. Quantitative data related to a few variables to detect patterns which can hopefully answer the research questions will be gathered.
Sampling Plan
Non-probability sampling will be applied for primary data collection methods.
Data Collection
Written materials like textbooks, journals and reports will be used to explain the circumstances of the proposed research. The Dental Sedation Teachers Group which is a national forum will also be consulted for information pertaining to conscious sedation in dentistry. Other methods of survey will be carried out if needed to study and discover the similarities if any and to research further facts.
Data Analysis
The association between dental anxiety and the application of pain and anxiety control standards in the patients under study was analysed. It was found that about 30% of the patients reported being pretty anxious, very anxious or panicked about visiting a dentist. There was a triple conflict between the reported use of anaesthesia and sedation and responders’ inclination for these treatment modes. These data propose that alarm of dentistry is still predominant and that patients who are fearsome would look for oral health care more on a regular basis if common anaesthesia or conscious sedation were more promptly obtainable. 10
The oral path is naturally the most dependable mode for drug administration. Protection is rendered against foreign contents by the vomiting mechanics, first-pass voiding and a muffled anaphylaxis reaction. The comparatively slow concentration cuts distributional influences and permits realisation of injurious courses and the option to put off further assimilation. The oral route also averts local harm linked with needle puncture, ischemia from intra-arterial shot and vein soreness contributing to thrombus phlebitis. On the other hand, variables determining drug assimilation—as well as gastric evacuating, GI assimilation, GI deactivation, first-pass liverwort metabolic process and variance in patient reaction linked to using determined doses—frequently bring up safety fears that fix drugging and drug effectiveness.10
Grounded on this thoughtfulness, the administration of two 0.25-mg dosages of oral or a beneath the tongue triazolam divided by time should be better than injecting a single 0.5-mg dose. Multiple drugging can sustain the length of the outcome and allow for fixed power to titrate the dose to accomplish the wanted effect. Sublingual shot of triazolam will create a quicker onset and augment titration capability by dipping some of the variables linked with oral injection. The dosage interval for measuring triazolam, on the other hand, is not yet established, nor have the associations amid the plasma density, effect-site density and detected sedation being demonstrated. Ultimately, the equaliser between intense tolerance to the sedative outcomes of several dosages and their mixed toxic consequences is not clear. Uncommitted data propose that while there is a high-quality bond between plasma intensity and observer-rated sedation in the first 2 hours after injecting a 0.25-mg dose, a disassociation takes place as the drug effect comes down more quickly than does the plasma concentration. Acute pharmacy active tolerance to triazolam has been established most distinctly by analyses in which the reaction of the drug spread out over several hours even when the plasma density is held unvarying.10
Literature Review
Introduction
Dental phobia is very common and most people fear going to the dentist for several reasons. According to a recent survey, 30% of patients still keep away from dentists. Due to this phobia, people refrain from seeing a dentist despite having acute dental problems like an abscess or a severely painful tooth. Sedation dentistry has come to the rescue of such people who get easily frightened by the mere thought of visiting a doctor. Conscious sedation methods have become the choice for millions of patients as it is a relaxed, painless and anxiety-free experience that solves all dental treatment problems. This treatment is referred to as sleep dentistry. It is very effective and a dentist can perform the dental procedure without any difficulty. The patient does not feel any pain or discomfort during the dental work.1
The present research approach about Conscious Sedation Methods Used for Adults in Dentistry is typically designed for the practitioners who analyse the data to improve their practice. Therefore the study is completely observational. Also, to get the desired results, clinical trial study is also adopted on par with the observational study. Comparative studies on the performance of different drugs in each technique applied are necessary to know the sedation quality of the drugs. 8
Difference between General anaesthesia and Local anaesthesia
General anaesthesia can be used only in response to clinical need. The publishing of ‘A Conscious Decision’ in 2006 ended in the surcease of general anaesthesia for dentistry which actually was put into force in Scotland from April 2001. General anaesthesia makes a patient unconscious for a long period and it is generally used in surgery. In dentistry it is less applied as it may bring in complications in the patients. Local anaesthesia blocks the feeling from the intended body part and eliminates pain during the dental procedures. 1
Indications for sedation
The indications for sedation in dental patients are mainly categorised as their psycholo-social behaviour, potential to medical and dental treatments. They can be identified as phobias, anxieties, inability to take medicines intra-orally, frequent fainting while undergoing procedures, idiosyncrasy to local analgesia, hypertension, epilepsy, asthma, ischemic heart disease, spasticity disorders etc. Some other factors for sedation are physical disabilities, and oral surgery procedures like exodontias and implants. Certain systematic problems seen in the patients are also considered as indications to sedation while in the handicapped it is exodontias and restorative. 14, 15, Types of sedation methods:
There are different types of sedation methods that are applied in adults and children. They are oral sedation, inhalation sedation, intravenous sedation and transmucosal sedation. 72 In transmucosal sedation oral, nasal and rectal administration are done conveniently according to the level of anxiety and phobia in patients. Pharmacological agents such as Diazepam, Midazolam, Propofol, Nitrous Oxide, Servoflurane and Lorazepam are the drugs administered for conscious sedation in dentistry.15, 16 Such applications and administering the medicines are in accordance with the general stature of the patients. Special attention is given to physically challenged patients and to those who are suffering from learning problems and mental disorders.32, 33, 71, 72
Risk factors
In spite of what is said above, drugs that suppress the nervous system cause some effects. If small doses are given, it will bring about light sedation. The patient is conscious in this state but the anxiety is well removed. But with an increased dose added by other drugs will cause major depression in the central nervous system creating deep sedation. When the consciousness is gone light general anesthesia will start to work which can be deepened by the administration of additional drug. In this regard it would be interesting to note that a population-based study conducted in UK recorded 1:250,000 as mortality rate in the administration of general anesthetic during 1970-1979. This reveals that any treatment using local anesthesia is less risky than the general anesthesia. It is assumed that if anesthesia is given for a longer period it will result in greater morbidity and mortality rate. Therefore, when depressant drugs for conscious sedation are applied careful titration and monitoring are required to ward off unexpected deep sedation in the patients. Though the risk factors are less in conscious sedation, the safety of the patients is resting with the dentists in their selection of the drug and clinical judgment to cope with the problems of anxiety and pain control.15
Problems Facing Female Staff and Assistants
Epidemiologic studies conducted to ascertain the relationship between exposure to anaesthetic gases and fertility problems in women have showed that the female dental personnel are affected by the exposure to nitrous oxide. The fertility of the females who were exposed to such gases was less than those unexposed. It was evident that the female dental assistants who were exposed to nitrous oxide for above five hours in a week had only 41% fertility in each menstrual period against the unexposed women staff. 37 The anaesthetic effects seen in the reproductive system of the female dental assistants when they were subjected to 33 different sedative agents proved that out of them only nitrous oxide has adverse effects on their fertility.38
These problems pose concerns about the safety measures and training required for the dental personnel to make them prepared for carrying out conscious sedation to the patients. 39 In this regard it must be seen that there is a great difference in the matter of safety between general anaesthesia and conscious sedation. General anaesthesia will cause loss of verbal communication between the patient and the sedationist or the practitioner. Therefore, it is necessary that every practitioner who is giving conscious sedation must be trained theoretically and practically. Accordingly, the General Dental Council of UK has stipulated relevant guidelines and has implemented adequate training programmes towards this end.40, 53-57
Sedation Practices
The U.K. Academy of Medical Royal Colleges and their Faculties have recommended that the principles of managing the patients who are subjected to healthcare procedures and safe handling of sedative drugs should be retained. The Academy’s Working Party has directed the dental personnel to be sympathetic in the patient management while carrying out the clinical care. Every step should be taken so that the sedation technique adopted shall be for pain relief only and in response to the behavioural pattern of the patient. If the pain is unpredictable, the same should be brought to the notice of the patient and a safe measure has to be conceived to manage the situation. The sedation drugs should be administered only with respect to the requirement of the patient. 39, 53-57, 61-64
Conscious Sedation methods used for Adults in Dentistry
In the past years there have been advancements in the field of sedation dentistry, and oral sedation specially has gained popularity among the different methods of sedation. The methods of conscious sedation include medicines that act as sedative drugs. These drugs are anti-anxiety agents and are potential to reduce the level of pain in the patient. There are other conscious sedation methods that use nitrous oxide and intravenous injections to cure dental ailments. People who suffer from a high level of anxiety are given various drugs and intravenous sedation while treating dental problems. These drugs are extremely helpful in sedating patients when the dental work is done. They are most effective to sedate any dental patients. 1-3
The oral and IV sedation dentistry are not dissimilar. And the only difference seen is in the mode of administering them. When compared to oral sedation, IV sedation dentistry is given through an injection to sedate and relax the patient instantly. As the patient goes into a deep level of consciousness the doctor is able to do his work knowing that it will certainly reduce the pain.1, 61
Amnesia is a well known side effect to IV and oral sedation. It helps the patients to have a painless dental treatment as they do not feel or remember anything regarding the procedure. This is a popular method in which amnesia is a known side effect to IV and oral sedation. Most patients do not experience any pain and feel as if the dentist has not touched their mouth at all. The oral sedatives are more acceptable now days and therefore, intravenous sedation dentistry is not generally used by doctors. 1, 61
Sedation Dentistry
Sedation dentistry is fast gaining popularity among various sects of people. An important necessity in sedation dentistry is that the patient should have a responsible caregiver. A patient may not be in a condition to drive home carefully after the medication is given. The caregiver normally stays with the patient for several hours after the treatment to ensure that they do not fall asleep due to the sedation. In generic, the stage or level of sedation differs from patient to patient and that too falls mainly on the mode of administration and type of the sedative drug selected for the dental treatment. The level of the sedation can vary from slight to deep depending on the drug used and other factors like the anxiety quotient present in the patient and the amount of time taken for conducting the surgery. It also rests on the type of surgery undertaken for the patient. Doctors normally administer only common analgesic to their patients by means of nitrous oxide inhalation. This is considered to be the mildest sedative in dentistry. There are some other medications that can be used to induce the same level of sedation in the patients.1, 60
Oral sedation is known to bring moderate level of sedation in patients, and doctors recommend it as it diminishes the overall awareness of any pain in them. The patient is subjected to reduced awareness to sights and sounds as well. Intravenous sedation causes deep sedation, thereby taking the patient to a higher level of depressed consciousness. Here, the doctor has to control the movement and breathing of the patient. The effects of intravenous sedation may last for many hours after the dental surgery and as such the patient does not feel any discomfort. 1
The above sedation methods are intended only to overcome the anxiety problems that persist in the patients and are not meant to replace the specific local anesthetics used during the process of dental treatment. Almost all dental doctors resort to sedation dentistry as they find it to be more convenient and safe while providing treatment to their patients. Among the several conscious sedation methods available now, doctors prefer oral sedation as the most suitable and convenient sedation method. To them, it is very easy to be administered and does not involve injections as most people are afraid of it. A patient who is given oral sedation sleeps through the entire procedure and hardly knows what is happening. As a result, the visit to the dentist is a relaxing and a pleasant experience. However, the patients do remain conscious despite their own perceptions. The service of the local anesthetic is highly required here to alleviate the pain of the patient and to block the responses. However care should be taken to administer it only next to oral sedation.1
In the last decade there have been concerns related to sedation techniques used in dentistry that do not require the services of an anesthetist. But such frights are unwarranted now. The performance during the past few years have proved that sedation dentistry has edged over all other forms of dental treatments and that it is now very popular at a global level. The term sedation dentistry is a synonym for the use of anesthesia while carrying out all types of dental treatments. As the patients are sedated by medicines they get into a relaxed state similar to sleep which helps the dentists to do their work more effectively. 2
Sedation dentistry is helpful to dentists because during its application they could keep the patients remain in the treatment chair even if it takes a long time for the treatment. To facilitate this, after taking the patients into confidence the doctors apply sedation methods so that they could deal effectively with their dental phobia and control their movements as well. 2 In a recent survey conducted among the dental patients it was revealed that the provision for dental sedation was still not up to the mark. The demands are very high for dental sedation but the availability of the facilities is far less. They were of the view that it would be a boon if more access is provided to the highly anxious dental patients.51
Unlike what we may believe sedation does not make the patients totally unconscious but it soothes the nerves and makes them relaxed. Sedation dentistry is helpful for adults as well as children as it restricts their movements and responses considerably. The sedative reduces anxiety and places the patients in a half awaken state. They may not remember how they are treated and do not feel any pain during the whole dental operation. Towards this, the dentists usually administer sedative drugs or nitrous oxide to their patients to make them relaxed and overcome their fear. 2
In sedation dentistry the local anesthetic when administered to the patient will relieve the pain during the treatment as all the responses to pain are blocked due to the sedative. This happens only after the oral sedation has taken place. The patient will feel relaxed and very comfortable following it. The medications have to be administered with local anesthetics so that the patient gets sedated properly for the dental work. These agents are effective in inducing conscious sedation. Though the patients are at ease and in a relaxed condition they are aware of sound and can feel while the treatment is done. 1, 62-64
In the conscious sedation methods, dentists administer the sedatives to the patients during or after dental procedures. It is done by allowing the medication through inhalation, injection or oral application. There are more complex treatments that are used in conscious sedation methods than these. Such sedation methods sometimes use drugs that can induce deep sedation in the patient. These drugs cause a sense of numbness and the patient’s consciousness level goes down considerably. The merit of these sedation techniques are that the patient is relieved of pain and anxiety while the dentist performs the dental procedure at ease and expertise without any alarm. 1, 62-64
Degrees of Sedation in Dentistry
According to the General Dental Council, there should be provision for adequate anxiety control and it must remain an integral part in dentistry. Several types of dental sedation techniques are used now in accordance with the existing directives. A patient has several choices in dental sedation. The dentist normally recommends the sedation dentistry technique and it depends on the treatment that will be performed on the patient. It also takes into account the level or degree of the patient’s dental anxiety. After the check up, the dentist adopts the right sedation method required for the patient. It is decided whether the patient needs moderate sedation with oral sedatives or nitrous oxide. If these two are found not feasible the dentist may opt for a deeper sedation method like intravenous drugs and other medications. 3, 65
Who are the Sedation Dentistry Candidates?
Every patient needs appropriate anxiety control and the sedation method must be chosen carefully according to the type of treatment. Patients who go in for dental procedure have high levels of anxiety and area afraid of the treatment. Moreover, they may also need more complex treatment and want it to be performed without any pain or discomfort.3
Is there any way in which Dental Anxiety can be treated?
The same sedation method is not advisable for all patients. It varies according to the physical condition and age of the patients. People usually avoid going to a dentist for years together as they are gripped with fear of the treatment procedures. This may be due to some past traumatic dental experience that they still need to overcome. Due to this they become reluctant to consult a dentist even if their dental problem is very acute. However, the moment they are convinced about the conscious sedation methods and how it makes the entire procedure free from pain, they will agree to the treatment procedure. 3
Different methods of Dental Sedation
In sedation dentistry effective and precise management of pain and anxiety have to be observed scrupulously. Conscious Sedation is an inseparable part of sedation dentistry. The different medications used in sedation dentistry help a patient immensely. They help the patient who is undergoing the treatment to be more comfortable during the dental visits. The sedation drugs are very helpful and effective in controlling the pain of the patient who is undergoing the treatment. It also helps them to relax. Other medications are administered to the patients so that they do not have any consciousness during the dental procedure. The dentist is able to do his work better. 4
The dentist before implementing the sedation methods must take the patient in confidence and inform the details of drugs to be given for the treatment. He should be satisfied with the overall health condition of the patient. If not, the treatment may not become smooth and result oriented. The patient will have to inform the dentist about his medical history and other details such as allergies to certain medications or his anxiety levels that can thwart the treatment. The dentist can become selective in determining the best treatment for his patient. It has to be a joint effort on the part of the patient and the dentist to sit together and decide upon the most appropriate steps for the treatment and to make the whole experience as pain free as possible. 4
Costs of Sedation Dentistry
The health insurance is still keeping distance in giving proper health cover to sedation dentistry, and this stance is creating problems to the patients in getting reimbursement of the medical expenses that are incurred towards the treatment. Patients are left with no other choice but to bear the heavy medical expenses. Most of them are unaware of the sedation dentistry costs and it creates uncertainty in pre-assessment of the expenses. The sedatives are very expensive and are not static and vary according to the type of treatment. The cost of the dental work that the patient has to pay is additional. These adversities make sedation dentistry unaffordable like ‘moon and six pence’ for a layman. 1
The cost of oral sedation is very high in UK and it changes according to the popularity of the dentist and geographical location. The other forms of sedation are just as expensive and even more as intravenous and general sedatives are charged hourly and differ in cost. The reason for its becoming costlier than oral sedation is due to the fact that the dental doctor needs to be assisted by a dental anesthesiologist for administering sedation methods during the dental work. As such it would only be proper to consult with the insurance company to know whether these companies give cover to sedation dentistry, at least before availing the treatment. This will avoid unwanted expenses and worries related to sedation dentistry. 1
The risks involved in Sedation Dentistry
Sedation dentistry is cost effective and economical to every patient. It is of the view that sedation dentistry is akin to any other type of general anesthesia and that the notions otherwise are really baseless. The sedatives used in conscious sedation methods should be administered to the patient by a skilled dentist and his staff so that the chances of complications are significantly reduced. 1
Considering all these problematic situations it deems necessary that the patient shall seek the help of the dentist to have a general awareness about the drug use. He must reveal to the dentist the side effects if any he had had, prior to availing the benefits of the sedation dentistry. This can make the things much easier and feasible and will enable both the patient and the dentist to tackle the problems. Additionally, it will also help the doctor to determine what type of medication has to be given to the patient during the treatment if the past history of the person is known. The failure on the part of the patient to disclose information to the doctor may bring in unfortunate incidents during the treatment for which the dentist cannot be held responsible. 1
The lack of ethics in male dentists and female patients during the past several years has brought concern in the sedation dentistry. Female patients had been sexually assaulted at dental offices earlier and these precedents may cause worry among women patients. In such a case a female patient may insist that a caregiver should be present during the dental work. Otherwise, one can go for a female dentist which would be a safer side. Nevertheless, these types of incidents are very rare and one must not consider this to be a bad reflection on this field of medical science. Sedation dentistry is a blessing for so many people as it provides a solution to painful dental treatment. The patient should not delay in going to a dentist as it will make matters worse. The tooth pain or an abscess may gradually become acute and will lead to complicated issues in the future life of the patient.1, 2, 25,
Sedation Dentists
The organisations and statutory bodies in dentistry have issued directives to the effect that the dental professionals are moderately trained in handling sedative equipment, drug administration and techniques for sedation dentistry. For this purpose the Association has conceived certain crash training programmes of 25 hour duration similar to advanced CPR course. The dentist even though is trained in sedation dentistry is not considered as an expert because he will still have to learn how to evaluate a patient’s medical history carefully. With proper training apart from his physician-status, the dentist can very well determine the exact sedation method required for the patient. 1, 4, 39
Benefits of Conscious Sedation Methods
There are several sedation dentistry methods that help patients to overcome fear and anxiety during a treatment. 5 The conscious sedation methods in dentistry are a solution for those who:
- have difficulty in getting sedated
- have extremely sensitive teeth.
- need several dental procedures.
- underwent traumatic dental problems.
- have aversion to injections.
- Loathe aroma and taste connected with the treatment
- hate their own disfigured teeth
- do not have the right medical, physical and mental conditions for sedation dentistry.
- look forward to a relaxing, problem free and a comfortable experience. 5
Different types of Sedation methods
Sedations are of different types. The conscious sedation methods help the patient a lot while undergoing the treatment. Doctors let the patient choose the level of sedation in such cases. The patient may need to relax a little or may lie to sleep during the dental procedure. It is up to the patient to choose the sedation method. Doctors will administer the sedation method accordingly.5, 66, 72
Comparison between important conscious sedation methods
Inhalation sedation as compared to Intravenous sedation
Inhalation sedation
The report of Standing Dental Advisory Committee, Department of Health4 says: “The only currently recommended technique for inhalation sedation is the use of a titrated dose of nitrous oxide with oxygen”.
Nitrous oxide is allowed to inhale during the treatment in order to place the patient in a relaxed condition. The patient experiences mild sedation due to it. For almost all patients Nitrous oxide induces a higher level of sedation and the application of local anesthetic will relieve the pain that follows the treatment. This type of sedation has long been in use in dentistry and is one of the conventional methods. There are few side effects to inhalation sedation. Therefore, doctors do not recommend it generally. 4
How is Intravenous sedation applied?
Standing Dental Advisory Committee report stipulates that “The standard technique for intravenous sedation is the use of titrated dose of single drug: for example the current use of a benzodiazepine”. 4
But in the Intravenous method the doctor gives an injection to the patient and the drug is injected for sedation. Instant sedation is brought to the patients by injecting the drug right into the blood stream. The patient does remain conscious and at the same time is deeply relaxed to allow the treatment by the dentist. The patient’s response to the injected drug is monitored by the anesthesiologist very carefully throughout each treatment session. This ensures that during the entire process the patient is in a comfortable condition and receives just the right amount of sedation required for the dental work to complete. Extra dosage may prove harmful and so it needs to be administered by a skilled dentist only. 4
Intravenous sedation as compared to intravenous sedation using different drugs
Intravenous sedation
Doctors use a blend of sedative drugs during the treatment. I.V. as the name suggests stands for intravenous, and it means that the sedation medication is administered directly into the person’s blood stream through an injection. The patient is given only one shot and he experiences light to deep sedation depending on the type of treatment that is required. The sedation effect is almost instantaneous. Overcoming the fears is a big hurdle before the dentists and that comes in the way of the patients getting optimal oral health for themselves. 4, 60
Intravenous sedation using different drugs
Intravenous sedation using drugs may be appropriate in certain cases and they are extremely effective. This sedation method with multiple drugs may be necessary for some patients as a single drug may not work for them. These types of sedation with a combination of oral or inhalation sedation may be beneficial in some cases and is recommended by the dentists to their patients. Doctors also go in for infusion of short acting agents during the treatment. Therefore, intravenous sedation needs to be administered carefully by trained dentists along with a team of professionals in an appropriate medical environment, and only then it is considered as safe by the patients.4
Oral Sedation vs. Intravenous Sedation
Oral Sedation
With the application of oral sedation the patient may sleep or doze off instantly. It is painless and is readily available as pills or in liquid forms. Those who fear the needle or are scared of injections may choose this type of sedation. This medication affects people in different ways and varies in its effectiveness depending on the factors such as genetics, age and weight. Previous system of medication they had will also determine the effectiveness of the sedatives. Normally sedation will happen in the patient after some minutes of taking the pills. However, when compared to the other forms of sedation, most people respond favorably to oral sedation. 5
Intravenous Sedation
Another effective sedation method is the intravenous sedation method. In this method, the sedative is injected into the blood stream of the patient. It is found very useful in dentistry and as such it is considered as the best sedation method where the patient requires instant sedation. This will enable the dentist to proceed with the treatment without losing any time. The intravenous sedation is administered through the patient’s veins and that is the reason why the medication acts so fast and effectively. The drug is injected directly in to the person’s blood stream causing sedation quickly. 5
A single drug or multiple drugs are injected according to the type of treatment given to the patient. The person remains in the conscious state and when the medication starts to wear off more medication can be given to the patient. I.V. sedation is the best type of conscious sedation method in sedation dentistry. It is due to the fact that the patient is sedated within moments of taking the injection. 5, 60 According to dentists, 5 this sedation technique induces the most powerful amnesic effect of the three popular sedation methods namely, inhalation, intravenous and oral. Intravenous is commonly used in Oral Surgery Cases as it is very effective. In oral surgery, oral surgeons have to perform reconstructive and cosmetic surgery, implants and other dental work along with diagnostic and emergency surgery. Dentists who are trained along with proper certification are only allowed to administer intravenous sedation to the patients. This is preferred by most of the dentists and patients because intravenous sedation gives the option to the dentist to administer more drugs or medication if the patient is not adequately sedated in the first time. This is the reason for its popularity.5 Oral Sedation is found to be effective when:
- the patient wants the benefits of sedation but at the same time does not want to pay the fees associated with intravenous sedation because it is too high.
- the oral sedation is greatly easier to administer to the patient when compared to intravenous sedation.
- the patient is scared of injections 5
Intravenous Sedation is effective when:
-the patient has to drive himself to his dentist. In oral sedation the medication needs to be taken by the patient just an hour or more before the appointment with his dentist. In such a condition, it is not advisable to drive.
- the person is not averse to a shot or injection. This type of sedation allows the doctor to have a much better control of the patient’s sedation level.
- the medication wears off faster compared to oral sedation and the dosage can be monitored more precisely by the medical practitioner. 5 .
Transmucosal sedation versus pre medication
Transmucosal sedation
This is an effective technique in sedation and is recommended by many dentists. Drugs are administered to the patients through the nose. It is also known as intranasal sedation and the medications given are midazolam or other benzodiazepine. Transmucosal sedation is different from other premedication where the main aim is to make the anxiety management technique less troublesome. 3
Patients do suffer from a great deal of anxiety and the dentists have to try to make them more comfortable during the treatment. This is why different sedation techniques are adopted by the dentists. It is important that in the case of oral or transmucosal sedation in dentistry, medication must strictly be administered under the able guidance of a qualified seditionist. It is compulsory, because sometimes it can happen that the patients are given more medication than they actually require by the negligence of a dentist. In such cases the patient can be harmed. The necessity of the presence of a qualified sedationist will avoid such problems as the medication can be given according to the dosage needed by the patient. 3
In the transmucosal sedation the accurate titration of midazolam or benzodiazepine can be administered to the patient against his response. Thus, proper sedation is not achieved in this technique. Oral and transmucosal sedation have their undesirable and potential effects. Dentists have to rely on a sedationist during the dental work. In these sedation techniques, fixed doses are recommended and it often leads to under- sedation or over-sedation in patients. The monitoring, discharge and supervision requirements in transmucosal sedation are similar to that in intravenous sedation. 3
Pre medication
In premedication the patient can take the medicine the night before and in that no supervision is required. The application is very simple. Oral premedication is advised with an effective low dosage of a sedative agent to help the patient in going to sleep the night before. The prime function of any oral pre-medication is to assist the patients in getting rid of their fear. It helps them to soothe their nerves before the actual treatment. Many dentists feel that it is far from being the perfect sedation technique for patients. It has been observed that oral pre-medication when administered to the patient along with a small dosage of benzodiazepine can help in reducing the anxiety level. Normally, patients who are given oral pre-medication should have suitable pre- and post-operative directions so that they know the dental treatment process better. 3
Over the past years, people have expressed their concerns over the safety of the sedation techniques used for healthcare procedures where the presence of an anesthetist is not at all required. The concerns have persisted because it has been found that many of the sedative drugs are randomly being administered quite unnecessarily and inappropriately to the patients at large. Dentists are doing this without adhering to some of the key components of published recommendations. This has created situations in some cases where the patients have been harmed. Thus, while giving any sedative medication to the patient, sufficient care should be taken so that it does not invite any harm. 3
Inhalation sedation method with
Nitrous oxide
Among the several sedation methods, the inhalation method is the most versatile one and is preferred by many patients the world over. This is due to the fact that in this form of sedation dentistry there is no requirement for injections, actions or medications that the patient may have to undergo prior to the treatment. Dentists make use of inhalation dentistry as they are able to manage the sudden anxiety attacks of their patients. Most of the times, the patients complain that the regular dental check ups are very difficult and unpleasant. Knowing that the dentist easily administers nitrous oxide to distract and help the patient relax. In normal practice, the dentist gives a pill to the patient to take a day before the check up. They even consider an intravenous sedation if the patient is driven back home by a friend. 3, 66-68
Patients can become selective and opt for inhalation sedation. It is better than oral sedation as one does not have to wait for the effects of the oral sedation for long. It is easy to administer the inhalation sedation and it can be given to the patient at any time. The side effects of inhalation sedation are short lived. Therefore, the patient does not feel groggy throughout the day. The dentist administers the inhalation sedation to the patient at his chamber. 3
Once the patient reaches the place of the dentist, a mask or nasal cannula will be fixed on the nose. With the help of the mask, the oxygen and nitrous oxide (laughing gas) will flow inside and the sedation starts to take place gradually. The patient’s condition is closely monitored and at the slight indication of any pain or discomfort, the dentist can adjust the mixture in such a way that it changes the level of sedation in the patient instantly. The nitrous oxide gas relaxes and relieves the patient from any anxiety. The patient is taken care of and made comfortable as the dental treatment may take hours at a stretch. 3, 68
The other factors that help a patient to get relaxed and distracted from the procedure are the radio, television and white noise machines. Since the effects of inhalation sedation are short, the patient should be reasonably alert. This form of sedation is liked by patients as it is an important method of relieving fear. It is easy and pain free and as such people going in for dental treatment prefer to have this sedation. 3
Sevoflurane
Several studies have been conducted to find out whether inhalation sedation is effective with sevoflurane in outpatient third molar surgery. In one such study conducted by the College of Dentistry, Ohio University twenty four patients who were to have their third molar surgery were administered nasal hood inhalation sevoflurane or an intravenous deep sedation using midazolam and fentanyl followed by propofol infusion. Patients responded well to the sedation methods and the doctors were very satisfied with the overall result of the procedures. 6, 41
In the study several points were observed such as measuring patient, surgeon, and dentist -anesthesiologist subjective satisfaction with the technique, pschychomotor recovery, amnesia and physiological parameters. Doctors came to a conclusion that there was no major difference in the results of sevoflurane, midazolam, fentanyl and propofol sedative groups. A marked trend showed that the patients recovered fast in the sevoflurane group. From this it was found that sevoflurane can be an excellent sedative to be given to healthy patients as a deep sedative rather than a general anesthetic to remove the third molar surgeries in dentistry. 6
The use of the conscious inhalation sedative nitrous oxide has a long history of success and safety in the dental office, provided that supplemental oxygen is administered. Nitrous-oxide oxygen inhalation sedation has rapid onset and recovery, with varying degrees of analgesia, and has minimal respiratory and cardio-vascular and other adverse effects. This sedation method is very common and is used by the dentists. However, it has been found that nitrous oxide and oxygen do not provide adequate sedation to the dental patients. Thus, alternative techniques were thought about in dentistry and that is how intravenous sedation came into practice. 1
Over the years, inhalation sedations with other well known drugs apart from nitrous oxide have been unpopular with the dental patients. This is so because most of the drugs have a pungent smell and are not accepted by the conscious patients during and after the treatment. Moreover, these anesthetics provide low onset and recovery in patients. Volatile anesthetics are considered complete if they produce amnesia, muscle relaxation, hypnosis, and analgesia when given in appropriate doses. Patients should not feel the pain during the dental procedure and an anesthetic that fails to sedate the patient during the treatment will not be considered effective. 1
Sevoflurane and Desflurane are now the two most popular and new inhaled anesthetics that have a rapid onset and recovery in patients. Unlike sevoflurane, Desflurane has a pungent and unpleasant smell that is unbearable to a sensitive patient. Sevoflurane on the other hand, has a pleasant smell and as such it is well tolerated for mask induction of general anesthesia in patients. Doctors use sevoflurane due to the fact that the patients including adults and children respond well to it. Presently, doctors are exploring the potential of sevoflurane as a deep sedative on volunteers only and not on patients undergoing surgical procedure. 1
Oral sedation with various drugs
Lorazepam
Patients are given Lorazepam as oral sedation in dentistry. This particular medicine was earlier known as Ativan and Temesta in the market. It is well known high potency benzodiazepine and dentists recommend it as a drug to be taken orally by the patients prior to the treatment. Lorazepam is suggested as the best medicine because it has got the five important intrinsic benzodiapine qualities and effects. 7
The medicine is highly effective as hypnotic, muscle relaxant, axiolytic and as an amnesic sedative. The dentists have confirmed that Lorazepam has been very useful in sedating aggressive patients as well as hospitalized patients due to its sedative qualities. It is very good for the treatment of patients suffering from acute anxiety, acute seizures and insomnia. This particular drug is a short acting one and thus starts acting on the patient pretty fast. It has to be given to the dental patient in doses so that it does not affect adversely. 7
The therapeutic effects of this medicine are innumerous and due to it dentists used to tell lies to administer the drug orally to their patients to sedate them properly. In this connection it must be mentioned that Lorazepam can become addictive. Mostly people misuse it and take advantage of it for various reasons. Some do it for recreational purposes. Others simply take it continuously against proper medical advice. This unwarranted usage makes this useful drug a harmful one. 7
Lorazepam creates dependence on the drug to a large extent. In addition it results in tolerance, cognitive impairments and benzodiazepine withdrawal syndrome. These can become very acute in patients if unchecked. One has to be extremely careful with this sort of medicine because the cognitive impairments in patients may not completely reverse even when the treatment is ceased. High level of anxiety, sleeplessness, forgetfulness and psychosis are identified as the main withdrawal symptoms of this medicine. By stating this one can very well imagine the harmful effects of this medicine if they are given for a long period of time. 7
Dentists recommend Lorazepam for a short term use from 2-4 weeks only, which is long enough for the dental treatment to take place. The continuous usage of the benzodiazepines may create adverse effects in children and aged patients. The elderly patients have complained of poor body balance. Due to this they have problem standing steadily and fall often causing injuries and hip fractures. The adverse effects are depression, insomnia etc. From this fact it could be clearly seen that the drug is very popular due to its properties. It is up to the dentists to administer the medication in the proper dosage so that it helps in sedation of the patient. 7
Lorazepam is used as a pre medication by the dentists. It has good axiolytic effect and is known to be the best in short term management of severe anxiety problems in dental patients. The FDA has repeatedly warned against the use of Lorazepam and other benzodiapines for more than 2-4 weeks. More and more dental patients are given Lorazepam as a pre medication and it helps them to soothe their nerves. While this happens the dentists can perform their work with ease. This medicine is given before a general anesthetic. This reduces the amount of anesthetic agent required during the treatment. The drug ensures that the patient wakes up with a pleasant feeling and does not feel any discomfort associated with the dental treatment. 7
Any dental treatment of a serious nature does cause a lot of pain. The conscious sedation methods are used so that the patient does not feel the pain or anxiety before or after the treatment. Oral medication becomes a boon in such situations and therefore, Lorazepam is given to the patients one and a half to two hours before the dental work, whereas in the intravenous sedation method Lorazepam is injected on to the patients around ten minutes prior to the treatment. This is given in palliative sedation as an alternative to midzolam and is very effective in intensive care units for its properties such as hypnosis, amnesia etc. The efficacy and safety of the use of the different sedatives have long been established. It has successfully managed the anxiety in patients in all kinds of dental treatments. 7
Midazolam
Midazolam is another effective sedative used in oral sedation. The drug is absorbed quickly and is ideal if given orally. It can be mixed in liquids and given to the patient. The drug is known to produce the desired sedation in the patient before the treatment. Midazolam has an oral bioavailability of 35 to 44% which is considered to be allowable in a sedative. It begins to act fast and the effects show just after 15–30 minutes from administering the medicine. It has been observed that the peak plasma levels are achieved within 20–50 minutes of administering it. 8
Midazolam is very effective in treating children who undergo dental procedures. In adults the drug is less effective. Dentists are using the intravenous preparation of midazolam orally for short dental procedures on adults. Specific dose of 0.25 mg/kg with a cumulative maximum of 20 mg are usually proposed by the dentists for the dental treatment. Despite the advancements in the local anesthetic agents, most patients are still scared of dental procedures. Some patients have a low level of fear, while the moderate patients have high levels of fear. It is the last group of patients who present the greatest challenge to the doctors as they succumb to fears and anxiety. The oral sedatives are preferred by most of the patients. 8, 25
According to dentists, most adults have very little objection to oral medications. This is because the oral route is less costly, widely accepted and convenient. Oral sedation is effective unlike what most people may choose to believe. If it had not been so these medicines might not have been in the market at all, and the dentists would not have recommended them as sedatives. 8
The double-blind randomised study conducted by M.R.C. Rodrigo and L.K. Cheunga computed the value of midazolam given orally. The patients selected were having minor oral surgery. Thirty young and healthy patients who had bilateral impaction of lower third molars were put to the study. During the patient’s first and second visits they were given midazolam tablets. After 45 minutes the teeth were subjected to surgical removal. Most of the patients were found to be relaxed during the surgery and that Midazolam sedation exhibited was stable with enough verbal response.41
Transmucosal
Transmucosal sedation
This is an effective technique in sedation and is recommended by almost all dentists. Drugs are administered to the patients through the nose. It is also known as intranasal sedation and the medications given are midazolam or benzodiazepine. Transmucosal sedation is different from other pre-medications where the main aim is to make the anxiety management technique less troublesome. 3
Patients are used to suffer from a great deal of anxiety and it is the duty of the dentists to make them more comfortable during the treatment. The necessity to apply different kinds of sedation techniques by them to help their patients depends on this factor. 3
Transmucosal comparative studies with midazolam
Oral versus rectal
Jensen B and Matsson L has conducted a comparative study on f oral versus rectal administration of midazolam in the form of a pre anaesthetic sedative agent in young children who are dental patients. The dental treatment in them is supported by sedation. Earlier it was administered rectally, but now the same has been changed to oral sedation. So the study was focused on to compare the sedative performance level of the oral and midazolam in the young patients who were subjected to dental treatment with general anaesthesia and also to know the acceptance level of sedation, application of facemask, amnesia etc. 50 children between 2-7 years were randomly selected to give oral or rectal sedation. In each group there were 25 children. The study revealed that the sedative effect due to rectal administration was a bit higher than oral administration (p = 0.07). It was concluded that both the techniques are positive. However, more sedation effect can be achieved by rectal administration of the drug in pre cooperative children. 47
Nasal v sublingual
As a premedication nasal transmucosal midazolam is found to be very effective in pediatric patients. Nevertheless, 61-74% of them will cry if drug is administered nasally. Sublingual benzodiazepines bring better results in adults. This blinded randomized study was aimed at comparing the reception of transmucosal midazolam and the behavioural response when the drug is administered through intranasal and sublingual routes. 93 patients aged 0.5-10 yr were randomly taken. Out of them 30 were infants. 39 were preschoolers, and 24 were of school age. They were given 0.2 mg/kg of midazolam nasally or underneath the tongue without adding any flavours. For another group flavoured midazolam was given sublingually. The findings such as the period of crying and compliance to the sublingual administration of the drug were recorded. The saturation level of Hemoglobin oxygen, sedation values etc. were also noted. It was concluded that in the children who were not crying prior to the drug administration through sublingual route have accepted the drug better than those who were given it intranasal. 48, 58, 59
Nasal v rectal v sublingual
Midazolam was transmucosally administered in forty seven randomly selected children and they were formed into three groups namely N, R and S. The group N was nasally given 0.2 mg.kg-1and group R was rectally administered 0.5 mg.kg-1. The third group viz., S received 0.2 mg.kg-1 drug sublingually. They were treated after 60 minutes of planned IV puncture and EMLA. Corresponding pyschological parameters were recorded following the premedication. It was done before and after i.v. puncture, until induction. The blood sample was taken at an interval of 10, 30 and 60 minutes immediately after premedication. The levels of midazolam, ACTH, cortisol, glucose etc. were noted. It was found that there were no commendable differences in the psychological parameters among the N, R and S groups and that the sublingual premedication has acquired a few advantages. Therefore it was concluded that the sublingual premedication was the first choice. The three forms of transmucosal applications are very safe.49
Nasal v rectal v Sublingual v Oral
Koran A, Katz J, Efra R, and Edelman LA 50 have undertaken a study to compare the efficacy of the 4 drug administering routes for premedication with midazolam in children. The study method was as follows: 119 non-medicated young children of 1.5-5 years were selected and divided into four groups as part of the randomized double-blind study. The first 3 groups consisted of 30 patients and the 4th one consisted of 29 children, and all of them were scheduled for elective surgery with sedation by using midazolam. It was given randomly to one of four groups. Group A was intranasal administered midazolam of 0.3 mg.kg-1; while group B took oral midazolam measured 0.5 mg x kg (-1). Group C was administered with midazolam of 0.5 mg x kg (-1) rectally, while group D was served midazolam about 0.3 mg x kg (-1) sublingually. A blinded observer checked them for symptoms of sedation and anxiolysis at an interval of 5 minutes before the surgery. Quality of induction, behaviour in response to postanaesthesia care and satisfaction of the parents were assessed. It was found that there were no identifiable variations in the sedation and anxiety levels among these children. The sedation and anxiolysis went up with time to get the highest at 20 minutes in Group A and at 30 minutes in groups B and C. 77% of the children cried due to nasal irritation after administering the drug. The parents were found to be very satisfied with the premedication. Therefore, it was concluded that all the 4 forms of sedation methods produced commendable levels of sedation and anxiolysis. Mask acceptance is expressively more viable for inhalation induction in children. 50
It is important that in the case of oral or Transmucosal sedation in dentistry, medication must strictly be administered under the able guidance of a qualified sedationist. The accurate titration of midazolam or benzodiazepine can be administered to the patient against his response. Thus, proper sedation is not achieved in this technique. Oral and transmucosal sedation have their undesirable and potential effects. Dentists have to rely on a sedationist during the dental work. Fixed doses are recommended and that often leads to under- sedation or over-sedation in patients. The monitoring, discharge and supervision requirements in transmucosal sedation are similar to intravenous sedation.3
Intravenous sedation
Midazolam
Midazolam is given as an intravenous sedation to the dental patients. Intravenous midazolam is recommended for procedural sedation, and the dentists administer it with drugs such as Opoid and Fentanyl as it is helpful in preoperative sedation. Upon injecting, this drug will function enough to create general anesthesia in the patients. Therefore, it is used to sedate ventilate patients in intensive care units as well. This drug is far superior to Diazepam and today it is among the most popular benzodiapines. It is a water soluble drug and dentists can infuse the medicine continuously if required. 8, 66
Midazolam is more effective in impairing memory. As compared to Midazolam, Propofol has better onset and recovery time. This drug is even good for memory impairing effect. Sufficient studies have established that in buccal and intranasal cases Midazolam is very effective. It cures anxiety and severe restlessness in patients. Intravenous midazolam when combined with nitrous oxide will become the tool for a successful treatment. However, intravenous sedation with Midazolam has its own limitations. In spite of the limitations it helps a large sect of patients who are suffering from varied levels of anxiety. 8
It is seen that in the intravenous sedation using Midazolam, its application depends on the different levels of sedation required by the patients such as deep sedation or general anesthesia. The dentist has to become very decisive in selecting the sedation method in order to make dental care successful. 8
Diazepam
Diazepam is also very effective in sedation methods. It is one of the prototypical benzodiazepine. Pharmacists refer to it as grandfather of all drugs. This particular medicine has been in the dental treatment field for over 42 years now and is widely used in sedation dentistry due to its high lipophilic molecule content. It maintains fast onset of action in dental patients which is normally within 20–40 minutes of taking the medicine. It has peak plasma levels between 1–2 hours after administering it orally. Diazepam doses range from 2 to 10 mg for adults while it maintains about 100% oral bioavailability. The effect lasts 20 to 80 hours. Due to this, patients complain frequently of daytime drowsiness and lethargy. 7
Diazepam has its own shortcomings. It undergoes hepatic metabolism by oxidative reduction. What happens is that both the parent molecule and active metabolites are affected by aging elements and hepatic dysfunction. This is due to the drug to drug interactions. Therefore, dentists have reduced the use of diazepam for oral sedation and have largely supplanted it by the better benzodiazepine alternatives. 7
Propofol
Propofol is another good drug for intravenous sedation. A study was conducted at random to compare the effectiveness and quality elements of these two methods by administering Propofol to obtain conscious sedation. The drug was administered to 11 dental patients who had not been taken this drug previously but currently are suffering from severe anxiety. Two dental procedures were conducted simultaneously. It was carried out on each patient. One of the methods was target-controlled infusion method that was monitored by the anesthesiologist. The other method was patient-controlled sedation method. The target controlled infusion method provided an initial concentration having a dose of 2.5 microg/mL. This was closely monitored in both the directions and thus the requisite clinical result was successfully met. 9
Considering the effectiveness of the patient controlled sedation mode, action was initiated to administer a dose of 4-mg bolus of propofol 10 mg/mL to the patients during each activation process. The drug was administered over 7s without a break in order to achieve the desired conscious sedation in the patients with PCS settings. The study revealed that the blood propofol concentrations were not different in both the modes. Thus, it was proved that in these two sedation methods, the level of patient satisfaction has remained the same. Moreover, the sedation quality and treatment susceptibility were very identical. It was also found that there was a link between the level of amnesia and the blood concentrations in the patients. 9
In the ACS mode, one patient was unresponsive to the sedation. In both the dental procedures, either mode of propofol sedation did not produce adverse cardio respiratory effects. In the group, five patients have expressed a strong liking for patient controlled sedation method, whereas three patients have admitted that they have a more liking to the administering of anesthetist controlled sedation in their future treatments. The dentists were very satisfied with the outcome of the study and they have come to a conclusion that the PCS settings achieved a satisfactory level of conscious sedation. The patients expressed relief and appreciation in the treatments too. Thus, it was confirmed from the randomized, cross-over study that the results of the treatment were analogous. The study has also affirmed that the blood propofol concentrations for attaining the required conscious sedation in anxious dental patients who have been subjected to the treatment method of patient–controlled sedation against the target-controlled infusion resorted to by the anesthesiologists are proved to be identical. 9
The tests showed that with the PCS, a good level of conscious sedation was achieved. There was also a high level of patient satisfaction. The patients responded well to propofol. When any drug is given through the veins it starts to act almost instantly and propofol was very active in this case. The sedation gravity provided by the drug was very satisfactory and it eased the task of the dentist during the treatment. The patients who have a high level of anxiety can be treated with intravenous infusion of propofol, for it achieves positive results in sedation. If all the major drugs in intravenous sedation are considered, propofol is found to be the best among them, because patients are relieved of anxiety and feel relaxed during the dental procedure. 9
Comparative Studies
A study was conducted to assess the quality of sedation and postoperative recovery in patients. This was for intra-operative sedation provided by two distinct methods. One was patient-controlled sedation with propofol. And the other was a standard method that used divided doses of midazolam and fentanyl. The drugs were given to forty number of ASA patients of one-day surgery who were having treatment for extraction of their third molar teeth done under local analgesia. It was seen that in patient-controlled sedation with propofol the drug produced mild sedation. Their eyelids were fully closed and they responded very well to the verbal commands of the dentists. On the other hand, three patients experienced deeper levels of sedation and they belonged to the midazolam and fentanyl group respectively. 10
Apart from what was stated above it was also observed that patient’s satisfaction was relatively higher in the patient-controlled sedation propofol group. Both the subjective intra-operative feelings (p less than 0.01) and the consent of the patients to the sedation procedure repeated (p less than 0.05) were taken into account.10 The drug was administered to the patients because the duration was long and the risk was high in surgery in the group of patient-controlled sedation with propofol. In the postoperative testing there was a new computerised test conducted. 10
In addition to the above a FAST index was prepared and it exhibited a reduction in the dose-dependent cognitive function in the midazolam and fentanyl group of patients. This condition has lasted till the patient was discharged. The changes in the cognitive functions of the patients after the medication have recorded a low rate and they did not relate to the dose of propofol at all. 10
Another comparative study was done to observe Intra-operative patient controlled sedation with propofol. The patients were given a bolus propofol of 18 mg over 5.4 s with a break period of sixty seconds against the propofol infusion of a quantity of 3.6 mg.kg-1.h-1. This study was done at random that included 38 ASA one-day to two-day surgery patients. These patients were having a dental procedure of two-stage bilateral extraction of third molar teeth with local anesthesia. Here the mean SD propofol of (mg.kg-1) was less in the patient-controlled sedation (2.39 (1.28) against the infusion (2.58 (0.84). No significant difference was noticed in them. However, there were a few minor differences between the methods in postoperative recovery of cognitive function.11
The patients have extended their full support and cooperation and the surgeon’s satisfaction was the same in both the sedation methods. The records showed that nineteen patients liked the patient-controlled sedation while ten patients liked the continuous infusion of Propofol. The rest of the patients were indifferent to the procedure. From this, it was found that the preferences such as mild, moderate or strong expressed by the patients were very strong in the case of patient-controlled sedation that was (p < 0.05). 11
The seventy six dental procedures have confirmed that the sedation experienced was limited to eyelid closure only, and that the patients have readily responded to commands during the entire dental procedure. The same level of sedation was observed in all of the 8 infusion cases. But in the 26 patient-controlled sedation cases, 12 patients had only less sedation (p < 0.01). This study showed that sedation in patient-controlled sedation with propofol was very safe. It was preferred by a majority of patients as compared to the infusion method of sedation. Two sedatives were administered to patients by an infusion pump as part of the study. After administering the anesthetic agents, they were compared against each other. This was done during the third molar surgery to find out the more effective drug. 11
About forty volunteers were chosen for the study. The patients were then given supplemental oxygen via nasal hood along with midazolam and fentanyl. Methohexital and propofol were also given through the infusion pump to the patients. After giving the bolus a constant infusion of 0.05 mg/kg/min methohexital or 0.066 mg/kg/min propofol to the patients, the psychomotor performance and the Hemo-dynamic cum respiratory parameters were recorded. But no differences were noticed and the two groups showed a steady level of sedation which was maintained throughout the treatment. Along with that the propofol provided smoother sedation than the other drugs. The patients preferred propofol as a sedative than the other sedative anesthetic agents. 12
In another clinical trial study by Leitch JA, Anderson K, Gambhir S et al 51 to find out whether Propofol sedation will offer higher level of anxiolysis, speedy recovery, mild amnesia and depression of psycho-motar function. Towards this, they adopted the partially blinded randomised regulated trial among 110 patients of 28 years old. They were then sedated for removing their third molars. The technique used was intravenous conscious sedation. Patients were put under operator-regulated sedation with drug agent midazolam and/or patient controlled sedation using propofol. The result showed that the anxiety level was significantly low in the propofol group. The average difference was 10 (SD 4)mm; p=0.010). Propofol patients recorded a better recovery time.51
In recent years, Methohexital and propofol have proved to be very effective sedative agents. They are popular sedatives during oral surgical procedures and are much sought after by dentists and patients. This particular study was specially conducted to make a comparison between these techniques. Several factors were compared and observations were recorded during the process. 13
Seventy patients between 18 and 40 years were put under this study. They were to have a surgery on the impacted third molars as they needed extraction. The group A relating to Methohexital and group B of Propofol had 35 patients each. They were then given an intravenous sedation with a quantity of 1.5 μg/kg of fentanyl and 0.05 mg/kg of midazolam as a premedication. This was followed by the continuous infusion of methohexital or propofol to the patients. The drugs were administered at a rate of 50 μg/kg/min and observations were recorded at every stage. 13
The patients were given an infusion of100 μg/kg/min to accomplish a level of sedation. Due to the sedation they closed their eyes and responded to verbal commands. These factors were noted immediately. Along with it several other aspects such as cooperation, recovery time based on cognitive, perceptual, nausea, vomiting and psychomotor tests were also studied in the two drugs. There was no difference between the two medication groups. Only the heart rate differed a bit. The heart rate was increased to the level of11 beats/min for group A. In the group B, the heart rate was increased only by an average three beats/min. This study showed that a continuous infusion technique with either methohexital or propofol (50 to 100 μg/kg/min) was completely safe for the patients and it was effective too. 13
It was found that significant clinical differences in cooperation, amnesia, cardiopulmonary stability, recovery time, comfort or incidents of vomiting or nausea were absent and out of the two drugs, methohexital recorded superiority over propofol in cost effectiveness. Hence, it is preferred by the dentists all over. These two drugs are very much in use and are found to be the most effective sedative anesthetist agents. Patients have reported that they are very comfortable with these two drugs during the sedation process. 13
Common Sedation Agents
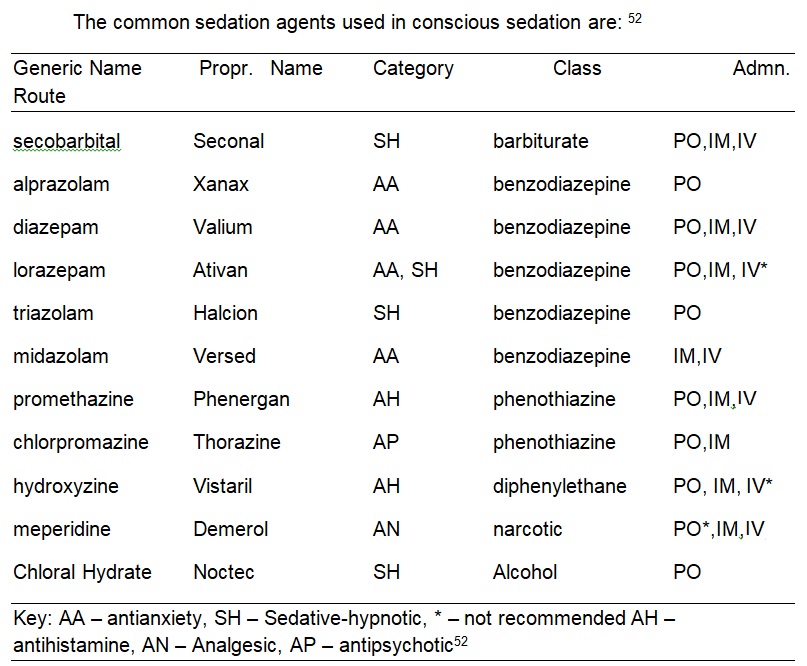
Sedative Hypnotics
Sedative hypnotics are the agents that are capable to produce sedation according to the dosage given. They are classified into two namely, barbiturates and non-barbiturates and can generate CNS depression including death. The disadvantage seen in these drugs comprises of respiratory and cardiovascular depression, GI disturbances, and addiction. Non-barbiturate sedative-hypnotics are called benzodiazepines and carbamates. The carbamates have low capacity than the barbiturate and have many disadvantages. The benzodiazepines are well known for their sedation qualities and do not carry any potential hazards. They are used in dentistry as sedative hypnotics such as triazolam and Lorazepam. 52
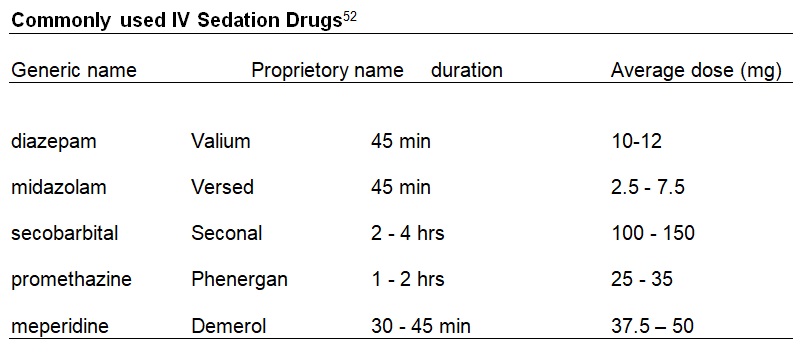
The dental assistance to those patients who have developmental disabilities needs some sort of behaviour management like reinforcement and verbal communication. Quite often some such patients become alarmingly anxious that they may create problems in dental offices which warrant added management techniques to overcome the frightful situation. Conscious sedation is the best option in these circumstances. 52
Dental implants
The provision of dental implants changed the dental practice in UK. It revolutionized the replacing of lost teeth. There is dependability and also has predictability about the success of the dental procedures. However, the resources of National Health Services are very limited and the number of patients referred for NHS-funded and NHS oriented implants in much higher than the available resources. Therefore, to combat the situation, the Royal College of Surgeons of England issued the Guidelines for the selection of deserving patients for dental implants by NHS.42-46
In implant therapy the ‘tooth’ is permanently attached to the jaw. The dentists evaluate the problem of the patients and refer them for dental plate or implants. Implants have the advantage of a natural look and they more or less look as if they are natural teeth. Implant dentistry is conducted in two stages – surgery and restoration. Normally, a prosthodontist does the restoration work but sometimes some dentists do both. A dental implant is basically a process whereby a screw is laid into the jaw and to this a cap is fastened. Sometimes implant failures arise if the dentist does not notice insufficient bone support while fixing the screw.42-47
More and more patients are now seeking a long term solution to replace the lost teeth and dental implant is the nearest procedure that one can find. The time taken for a dental implant surgery depends on the work that has to be done. All procedures are performed under local anaesthesia. This ensures that the patients undergo a relatively pain free process. The dental implant process is done in stages lasting from 3 to 6 months in many cases. It is not an overnight procedure. Average cost of an implant is about £2000, which is a huge amount for a layman. But the long term benefits outweigh the costs. However it depends on the type of dental implants that are required. 42-46
Dental implants are created with the help of commercially and medically unadulterated Titanium. Advantages of such implants are:
- Changed capacity to chew and speak correctly
- Regaining of facial aesthetics
- Conservation of continuing jaw bone structure
- Lessening of likely gum troubles and infections
References
Shameenpreeda, Sedation Dentistry Basics. 2009. Web.
Implementing and Ensuring Safe Sedation Practice for Healthcare Procedures in Adults. Report of an Intercollegiate Working Party Chaired By the Royal College of Anaesthesists. Web.
Conscious Sedation in Dentistry. Dental Clinical Guidance. Scottish Dental Clinical Effectiveness Programme (2006). Web.
Conscious Sedation in the Provision of Dental Care. Report of an Expert Group on Sedation for Dentistry. Standing Dental Advisory Committee, Department of Health (2003). Web.
Sedation Dentists Jackson Missisippi (2006). Web.
Ganzberg S, Weaver J, Beck FM, and McCaffrey G. Use of sevoflurane inhalation sedation for outpatient third molar surgery . 1999 46(1): 21–29. Web.
Donaldson M, Gizzarelli G, Chanpong B. Oral Sedation: A Primer on Anxiolysis for the Adult Patient. 2007; 54(3): 118– 129. Web.
Averley PA, Girdler NM, Bond S, Steen N, Steele J. A randomised controlled trial of paediatric conscious sedation for dental treatment using intravenous midazolam combined with inhaled nitrous oxide or nitrous oxide/sevoflurane. Anaesthesia (2004) 59: 844-852.
Oei-Lim VL, Kalkman CJ, Makkes PC, Ooms WG. Patient-controlled versus anaesthesiologist controlled conscious sedation with propofol for dental treatment in anxious patients. Anesthesia & Analgesia (1998) 86: 967-972.
Osborne GA, Rudkin GE, Curtis NJ, Vickers D, Craker AJ. Intra-operative patient-controlled sedation. Comparison of patient-controlled propofol with anaesthetist-administered midazolam and fentanyl. Anaesthesia (1991) 46: 553-556.
Osborne GA, Rudkin GE, Jarvis DA, Young IG, Barlow J, Leppard PI. Intra- operative patient-controlled sedation and patient attitude to control. A crossover comparison of patient preference for patient-controlled propofol and propofol by continuous infusion. Anaesthesia (1994) 49: 287-292.
Cohen M, Eisig S, Kraut RA. Comparison of recovery of propofol and methohexital sedation using an infusion pump. Anesthesia Progress (1996) 43: 9-13.
Johns FR, Sandler NA, Buckley MJ, Herlich A. Comparison of propofol and methohexital continuous infusion techniques for conscious sedation. Journal of Oral and Maxillofacial Surgery (1998) 56: 1124-1127.
Heasman PA, Restorative dentistry, paediatric dentistry and orthodontics Peter A. Heasman, Churchhill Livingstone, 2003, ISBN 0443061939, Web.
Anesthesia and Sedation in the Dental Office. NIH Consens Statement 1985 22-24; 5(10):1-18., Web.
Standards in Conscious Sedation for Dentistry, Published: October, 2000, Dental Sedation Teachers Group, Department of Sedation and Special Care Dentistry, Web.
Hallonsten A-L. Nitrous oxide-oxygen sedation in dentistry. Swed Dent J 1982;Suppl. 14.
Hallonsten A-L, Koch G, Schröder U. Nitrous oxide-oxygen sedation in dental care. Community Dent Oral Epidemiol 1983; 11:347-355.
Rowland AS, Baird DD, Weinberg CR, Shore DL, Shy CM, Willcox AJ. Reduced f ertility among women employed as dental assistents exposed to high levels of nitrous oxide. N Eng J Med 1992; 327(14):993-997.
Valtonen M, Salonen M, Forssell H, Scheinin M, Viinamaki O. Propofol infusion for sedation in outpatient oral surgery. A comparison with diazepam. Anaesthesia (1989) 44: 730-734.
Rowland AS, Baird DD, Shore DL, Weinberg CR, Savitz DA, Willcox AJ. Nitrous oxide and spontaneous abortion in female dental assistants. Am J Epidemiol 1995; 141:531-538.
Burns R, McCrae AF, Tiplady B. A comparison of target-controlled therapy with patient-controlled administration of propofol combined with midazolam for sedation during dental surgery. Anaesthesia (2003) 58: 170-176.
Roberts GJ, Gibson A, Porter J, de Zoysa S. Physiological changes during relative analgesia – a clinical study. J Dent 1982; 10:55-64.
Roberts GJ, Gibson A, Porter J. Relative analgesia. An evaluation of the efficacy and safety. Br Dent J 1979; 146:177-182.
Roberts GJ, Wignall KK. Efficacy of laryngeal reflex during nitrous oxide sedation (relative analgesia). Br J Anaesth 1982; 54:1277-1288.
Shipton EA, Roelofse JA, Blignaut RJ. An evaluation of analgesic efficacy and clinical acceptability of intravenous tramadol as an adjunct to propofol sedation for third molar surgery. Anesthesia Progress (2003) 50: 121-128. Web.
Kucukyavuz Z, Cambazoglu M. Effects of low-dose midazolam with propofol in patient-controlled sedation (PCS) for apicectomy. British Journal of Oral and Maxillofacial Surgery (2004) 42: 215-220.
Geldner G, Hubmann M, Knoll R, Jacobi K,1997. Comparison between three transmucosal routes of administration of midazolam in children. Paediatr Anaesth 1997; 7:103-9. Web.
Luyk NH, Zacharias M, Wanwimolaruk S. Bolus dose with continuous infusion of midazolam as sedation for outpatient surgery. International Journal of Oral and Maxillofacial Surgery (1992) 21: 172-175.
Leitch JA, Anderson K, Gambhir S, et al. A partially blinded randomised controlled trial of patient-maintained propofol sedation and operator controlled midazolam sedation in third molar extractions. Anaesthesia (2004) 59: 853-860.
Stephens AJ, Sapsford DJ, Curzon ME. Intravenous sedation for handicapped dental patients: a clinical trial of midazolam and propofol. British Dental Journal (1993) 175: 20-25.
Fukuta O, Braham RL, Yanase H, Kurosu K. The sedative effects of intranasal midazolam administration in the dental treatment of patients with mental disabilities. Part 2: optimal concentration of intranasal midazolam. Journal of Clinical Pediatric Dentistry (1994) 18: 259-265.
Rodrigo MR, Irwin MG, Tong CK, Yan SY. A randomised crossover comparison of patient-controlled sedation and patient-maintained sedation using propofol. Anaesthesia (2003) 58: 333-338.
Rodrigo MR, Tong CK. A comparison of patient and anaesthetist controlled midazolam sedation for dental surgery. Anaesthesia (1994) 49: 241-244.
Zacharias M, Hunter KM, Luyk NH. Patient-controlled sedation using midazolam. British Journal of Oral and Maxillofacial Surgery (1994) 32: 168-173.
Rowland AS, Baird DD, Weinberg CR, Shore DL, Shy CM, Willcox AJ. Reduced fertility among women employed as dental assistents exposed to high levels of nitrous oxide. N Eng J Med 1992; 327(14):993-997.
Rowland AS, Baird DD, Shore DL, Weinberg CR, Savitz DA, Willcox AJ. Nitrous oxide and spontaneous abortion in female dental assistants. Am J Epidemiol 1995; 141:531-538.
Implementing and ensuring safe sedation practice for healthcare procedures I adults. Academy of Medical Royal Colleges. November 2001
Guidelines for physiological monitoring of patients during dental anaesthesia or sedation. Society for the Advancement of Anaesthesia in Dentistry. London. March 1990.
Rodrigo MR, Cheung LK. Oral midazolam sedation in third molar surgery. International Journal of Oral and Maxillofacial Surgery (1987) 16: 333-337.
Sonia R Vartoukian and Hatem Algraffee, Does the Referral and Selection for NHS-Funded Dental Implant Treatment in the UK Follow National Guidelines? Department of Periodontology, Guy’s, King’s and St Thomas’ Schools of Medicine and Dentistry, King’s College, London, UK, 2007; 89(3): 247–251. Web.
Adell R, Eriksson B, Lekholm U, Branemark PI, Jemt T. Long-term follow-up study of osseo-integrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants. 1990;5:347–59. Web.
Lindh T, Gunne J, Tillberg A, Molin M. A meta-analysis of implants in partial edentulism. Clin Oral Implants Res. 1998;9:80–90. Web.
Palmer RM, Smith BJ, Palmer PJ, Floyd PD. A prospective study of Astra single tooth implants. Clin Oral Implants 1997;8:173–9. Web.
Johns RB, et al. A 5-year prospective multicentre follow-up report on overdentures supported by osseointegrated implants. Int J Oral Maxillofac Implants. 1996;11(3):291–8. Web.
Jensen B and Matsson L. Oral versus rectal midazolam as a pre-anaesthetic sedative in children receiving dental treatment under general anaesthesia. Acta Paediatr. 2002;91:920-925.
Karl, Helen W. M.D.; Rosenberger, James L. Ph.D.; Larach, Marilyn G. M.D.; Ruffle, Joan M. M.D, Transmucosal Administration of Midazolam for Premedication of Pediatric Patients: Comparison of the Nasal and Sublingual Routes, American Society of Anesthesiologists, May 1993 – Volume 78 – Issue 5.
Geldner G, Hubmann M, Knoll R, Jacobi K, Comparison between three transmucosal routes of administration of midazolam in children. Paediatr Anaesth 1997; 7:103-9. Web.
Kogan A, Katz J, Efrat R, Eidelman LA. Premedication with midazolam in young children: a comparison of four routes of administration. Paediatr Anaesth 2002; 12: 685-9.
Allen EM, Girdler NM. Attitudes to conscious sedation in patients attending an emergency dental clinic. Prim Dent Care. 2005;12(1):27-32.
MANAGING MALADAPTIVE BEHAVIORS: THE USE OF DENTAL SEDATION FOR PERSONS WITH DISABILITIES, SOUTHERN ASSOCIATION OF INSTITUTIONAL DENTISTS — Self-Study Course Module 5. Web.
Grant SMB, Davidson LE, Livesey S. Trends in exodontia under general anaesthesia at a dental teaching hospital. British Dental Journal 1998; 185: 347- 352.
Conscious sedation in dentistry. Practice inspection check list. Basic sedation techniques. Society for the Advancement of Anaesthesia (SAAD) 2004. Web.
Conscious sedation in dentistry. PCT Practice inspection check list. Notes for users. SAAD. 2004. Web.
Training in Conscious Sedation for Dentistry. Dental Sedation Teachers’ Group. 2005. Web.
Conscious sedation. A referral guide for dental practitioners. Society for the Advancement of Anaesthesia in Dentistry and Dental Sedation Teachers Group. 2001.
Abrams R, Morrison JE, Villasenor A, Hencmann D, Da Fonseca M, Mueller W. Safety and effectiveness of intranasal administration of sedative medications (ketamine, midazolam, or sufentanil) for urgent brief pediatric dental procedures. Anesthesia Progress (1993) 40: 63-66.
59 Fukuta O, Braham RL, Yanase H, Kurosu K. Intranasal administration of midazolam: pharmacokinetic and pharmacodynamic properties and sedative potential. Journal of Dentistry for Children (1997) 64: 89-98.
60 O’Boyle CA, Harris D, Barry H, McCreary C, Bewley A, Fox E. Comparison of midazolam by mouth and diazepam i.v. in outpatient oral surgery. British Journal of Anaesthesia (1987) 59: 746-754.
Implementing and ensuring safe sedation practice for healthcare procedures In adults. Academy of Medical Royal Colleges. 2001.
Guidelines for physiological monitoring of patients during dental anaesthesia or sedation. Society for the Advancement of Anaesthesia in Dentistry. London. March 1990.
Monitoring of patients during dental anaesthesia or sedation. Association of Dental Anaesthetists.1990.
Guidelines for sedation by non-anaesthetists. Report of a Commission on the Provision of Surgical Services working party. The Royal College of Surgeons of England, London. June 1993.
American Society of Anaesthesiologists; New classification of physical status. Anaesthesiology 1963; 24:111.
Murphy PJ, Erskine R, Langton JA. The effect of intravenously administered diazepam, midazolam and flumazenil on the sensitivity of upper airway reflexes. Anaesthesia 1994; 49: 105-110.
Nordt SP, Clark R. Midazolam: a review of therapeutic uses and toxicity. J Emerg Med 1997; 15:357-365.
Peretz B, Katz J, Zilburg I, Shemer J. Response to nitrous-oxide and oxygen among dental phobic patients. Int Dent J 1998; 48:17-23.
Royal College of Anaesthetists and Royal College of Radiologists. Sedation and Anaesthesia in Radiology 1992.
Rosenberg MB, Campbell RL. Guidelines for intraoperative monitoring of dental patients undergoing conscious sedation, deep sedation, and general anesthesia. Oral Surg, Oral Med, Oral Path 1991;71:1:2-8.
SAID — Guidelines for Dental Programs in Facilities for the Mentally Retarded/Mentally Ill. 1990.
Jastak JT, Praravecchio R. An analysis of 1,331 sedations using inhalation, intravenous or other techniques. J Am Dent Assoc 1975; 91:1242-1249.
A Conscious Decision: A Review of the Use of General Anaesthesia and Conscious Sedation in Primary Dental Care. Report of a Group Chaired by the Chief Medical and Chief Dental Officer. Department of Health (2000). Web.
Standards in Conscious Sedation for Dentistry. Report of an Independent Expert Working Group. Society for the Advancement of Anaesthesia in Dentistry (2000). Web.
Conscious Sedation in the Provision of Dental Care. Report of an Expert Group on Sedation for Dentistry. Standing Dental Advisory Committee, Department of Health (2003). Web.
Emergency Dental Drugs – National Dental Advisory Committee. Scottish Office Department of Health (1999).
Training in Conscious Sedation for Dentistry. Dental Sedation Teachers Group (2005). Web.
The Wylie Report. Report of the Working Party on Training in Dental Anaesthesia. British Dental Journal (1981) 151: 385-388.
Heasman PA, Restorative dentistry, paediatric dentistry and orthodontics. Peter A. Heasman, Churchhill Livingstone, UK, 2003, ISBN 0443061939, Web.
Anesthesia and Sedation in the Dental Office. NIH Consens Statement 1985 Apr 22-24; 5(10):1-18., Web.
Standards in Conscious Sedation for Dentistry, Published: October, 2000, Dental Sedation Teachers Group, Department of Sedation and Special Care Dentistry,
Luhmann JD, Kennedy RM, Porter FL, Miller JP, Jaffe DM. A randomized clinical trial of continuous flow nitrous oxide and midazolam for sedation of young children during laceration repair. Annals of Emergency Medicine 2001; 37: 20-27.
Martin JP, Sexton BF, Saunders BP, Atkin WS. Inhaled patient-administered nitrous oxide/oxygen mixture does not impair driving ability when used as analgesia during screening flexible sigmoidoscopy. Gastrointestinal Endoscopy 2000; 51: 701-3.
Averley PA, Girdler NM, Bond S, Steen N, Steele J. A randomised controlled trial of paediatric conscious sedation for dental treatment using intravenous midazolam combined with inhaled nitrous oxide or nitrous oxide/sevoflurane. Anaesthesia (2004) 59: 844-852.
Dionne RA, Yagiela JA, Moore PA, Gonty A, Zuniga J, Beirne OR. Comparing efficacy and safety of four intravenous sedation regimens in dental outpatients. Journal of the American Dental Association (2001) 132: 740-751.
Dolan EA, Murray WJ, Immediata AR, Gleason N. Comparison of nalbuphine and fentanyl in combination with diazepam for outpatient oral surgery. Journal of Oral and Maxillofacial Surgery(1988) 46: 471-473.
Dolan EA, Murray WJ, Ruddy MP. Double-blind comparison of nalbuphine and meperidine in combination with diazepam for intravenous conscious sedation in oral surgery outpatients. Oral Surgery, Oral Medicine, Oral Pathology (1988) 66: 536-569.
Ganzberg S, Pape RA, Beck FM. Remifentanil for use during conscious sedation in outpatient oral surgery. Journal of Oral and Maxillofacial Surgery (2002) 60: 244-250.
Gelfman SS, Gracely RH, Driscoll EJ, Wirdzek PR, Butler DP, Sweet JB. Comparison of recovery tests after intravenous sedation with diazepam- methohexital and diazepam-methohexital and fentanyl. Journal of Oral Surgery (1979) 37: 391-397.
Hook PC, Lavery KM. New intravenous sedative combinations in oral surgery: a comparative study of nalbuphine or pentazocine with midazolam. British Journal of Oral and Maxillofacial Surgery(1988) 26: 95-106.
Kaufman E, Davidson E, Sheinkman Z, Magora F. Comparison between intranasal and intravenous midazolam sedation (with or without patient control) in a dental phobia clinic. Journal of Oral and Maxillofacial Surgery (1994) 52: 840- 843.
Lipp M, Dick W, Daubländer M, Prior S, Jakobs W. Effects of an intravenous sedation technique with simultaneous administration of nitrous oxide in dental surgical operations. Anesthesia Progress (1989) 36:164-168.
Luyk NH, Whitley BD. Efficacy of oral midazolam prior to intravenous sedation for the removal of third molars. International Journal of Oral and Maxillofacial Surgery (1991) 20: 264-267 y.
Parworth LP, Frost DE, Zuniga JR, Bennett T. Propofol and fentanyl compared with midazolam and fentanyl during third molar surgery. Journal of Oral and Maxillofacial Surgery (1998) 56: 447-453.
Sandler NA, Hodges J, Sabino M. Assessment of recovery in patients undergoing intravenous conscious sedation using bispectral analysis. Journal of Oral and Maxillofacial Surgery (2001) 59: 603-611.
Scott RF. A double-blind comparison of nalbuphine and meperidine hydrochloride as intravenous analgesics in combination with diazepam for oral surgery outpatients. Journal of Oral and Maxillofacial Surgery (1987) 45: 473-476.
Stopperich PS, Moore PA, Finder RL, McGirl BE, Weyant RJ. Oral triazolam pretreatment for intravenous sedation. Anesthesia Progress (1993) 40: 117-121.
Zallen RD, Cobetto GA, Bohmfalk C, Steffen K. Butorphanol/diazepam compared to meperidine/diazepam for sedation in oral maxillofacial surgery: a double-blind evaluation. Oral Surgery, Oral Medicine, Oral Pathology (1987) 64: 395-401.
Conscious Sedation in the Provision of Dental Care. Report of an Expert Group on Sedation for Dentistry. Standing Dental Advisory Committee, Department of Health (2003). Web.
Rang HP, Dale MM. Pharmacology. Churchill Livingstone (2003).
Meechan JG, Robb ND, Seymour RA. Pain and Anxiety Control for the Conscious Dental Patient. Oxford University Press (1998).
Abrams R, Morrison JE, Villasenor A, Hencmann D, Da Fonseca M, Mueller W. Safety and effectiveness of intranasal administration of sedative medications (ketamine, midazolam, or sufentanil) for urgent brief pediatric dental procedures. Anesthesia Progress (1993) 40: 63-66.
Al-Rakaf H, Bello LL, Turkustani A, Adenubi JO. Intra-nasal midazolam in conscious sedation of young paediatric dental patients. International Journal of Paediatric Dentistry (2001) 11: 33-40.
Dallman JA, Ignelzi MA, Jr, Briskie DM. Comparing the safety, efficacy and recovery of intranasal midazolam vs. oral chloral hydrate and promethazine. Pediatric Dentistry (2001) 23: 424-430.
Kaufman E, Davidson E, Sheinkman Z, Magora F. Comparison between intranasal and intravenous midazolam sedation (with or without patient control) in a dental phobia clinic. Journal of Oral and Maxillofacial Surgery (1994) 52: 840- 843.
Sonia R Vartoukian and Hatem Algraffee, Does the Referral and Selection for NHS-Funded Dental Implant Treatment in the UK Follow National Guidelines? Department of Periodontology, Guy’s, King’s and St Thomas’ Schools of Medicine and Dentistry, King’s College, London, UK, 2007; 89(3): 247–251. Web.
Adell R, Eriksson B, Lekholm U, Branemark PI, Jemt T. Long-term follow-up study of osseo-integrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants. 1990;5:347–59. Web.
Lindh T, Gunne J, Tillberg A, Molin M. A meta-analysis of implants in partial edentulism. Clin Oral Implants Res. 1998;9:80–90. Web.
Palmer RM, Smith BJ, Palmer PJ, Floyd PD. A prospective study of Astra single tooth implants. Clin Oral Implants 1997;8:173–9.
Jemt T, Chai J, Harnett J, Heath MR, Hutton JE, Web.
Johns RB, et al. A 5-year prospective multicentre follow-up report on overdentures supported by osseointegrated implants. Int J Oral Maxillofac Implants. 1996;11(3):291–8. Web.
Fukuta O, Braham RL, Yanase H, Kurosu K. The sedative effects of intranasal midazolam administration in the dental treatment of patients with mental disabilities. Part 2: optimal concentration of intranasal midazolam. Journal of Clinical Pediatric Dentistry (1994) 18: 259-265.
Young ER, Therapeutics and Sedation in Dentistry, CAN. FAM. PHYSICIAN Vol. 34: 1988. Web.
Cronje, J., March 29, Research Methods Online, 2005, Web.
Trochim, W.M.K., Research Methods Tutorials, 1996-2004, Web.
ESRC, Research Methods, Economic and Social Research Council (ESRC) 2007a, Web.
Yin, R., Case study research: Design and methods (2nd ed.) Beverly Hills, CA: Sage Publishing (1994).
Davison, R.M. and Vogel, D.R., Group Support Systems in Hong Kong: An Action Research Project, in Galliers, R.D., Markus, M.J. and Newell, S. Exploring Information Systems Research Approaches: Readings and Reflections, Routledge2006: 33-46. Web.
ESRC, Qualitative Methods, Economic and Social Research Council (ESRC) 2007b, Web.
ESRC, June 8, Quantitative Methods, Economic and Social Research Council (ESRC) 2007c, Web.
Pathways, Action Research. Learning Point Associates. North Central Regional Educational Laboratory (NCREL) 2004. Web.
Coulthard P. Conscious sedation guidance,, Unit of Oral and Maxillofacial Surgery, School of Dentistry, University of Manchester, UK Evid Based Dent. 2006;7(4):90-1. Web.
Kroboth PD, Bertz RJ, Smith RB. Acute tolerance to triazolam during continuous and step infusions: estimation of the effect of offset rate constant. J Pharmacol Exp Ther 1993; 264:1047–55.