Introduction and theoretical framework
The knee joint is composed of ligaments, cartilage, bone, and fluid (Gandhi & Viscusi, 2009). These structures work together with the tendons and muscles to enable the knee joint to move. Injuries caused to any of the structures can result in a variety of knee problems that may necessitate knee replacement to restore normal function. There are a significant number of people who suffer from severe cases of discomfort in their knees, mainly due to osteoarthritis and meniscus tears. Older patients who show up for Knee replacement procedures are most commonly afflicted with complications resulting from conditions such as osteoarthritis, fractures and meniscus tear (Gandhi & Viscusi, 2009).
Osteoarthritis (OA) is regarded as the most common disease in individuals aged 65 years and above that compromises the quality of life due to pain, reduced joint movement and walking ability (Adams, White, & Beckett, 2010). Knee replacement surgical procedures have been proven to be effective in the elimination of pain and improvement in the patient’s ability to walk.
Older patients who have had a knee replacement surgery normally experience pain resulting from the swelling and stiffness around the surgical area or a result of stress buildup. Effective postoperative pain management is of great importance in the prevention of postoperative (OP) pulmonary and neurovascular complications (Gandhi & Viscusi, 2009). Several approaches are advanced in the management of postoperative pain in older patients who have had knee replacement surgery.
These approaches are broadly categorized into conventional approaches, complementary and alternative approaches. Conventional approaches include the use of opioid pain relievers such as morphine, oxycodone, and fentanyl, and NSAIDs such as aspirin and Cataflam (Hirvonen, 2006). Complementary approaches are often achieved through the combination of conventional approaches and alternative approaches. The use of true lavender via massage and inhalation is one of the most commonly used alternative approaches to post-operative knee pain management.
This study seeks to utilize the PICOT framework to compare the effectiveness of true lavender and conventional medical treatment to relieve pain within 48 hours of knee surgical procedure in adults.
The study will be based on the premise that the use of true lavender causes patients to relax and therefore relieves the pain caused by stress. The PICOT research proposal developed for this paper states: (P) Among admitted adult post-op patients who have undergone a knee replacement (due to osteoarthritis, fracture, or meniscus injuries) (I) How does the use of True Lavender (C) Compare to a patient only receiving conventional medical treatment and pain medications (O) In the management of pain to decrease the patient(s) pain response based upon the premise that the use of lavender on post-op patients causes them to relax and therefore relieves the pain caused by stress (T) Within 48 hours of surgical procedure. This comparative PICOT study will utilize the Numeric Rating Scale to assess pain alleviation by the use of true lavender, and conventional methods.
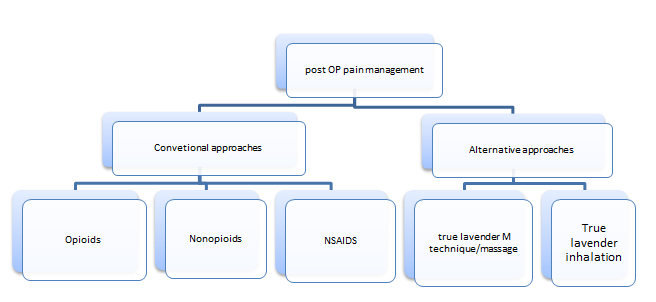
The figure above indicates the theoretical framework that will be the focus of this study.
The research will be a quantitative study in which the effectiveness of the conventional medications i.e., NSAIDs, opioids, and nonopioids will be compared with the use of true lavender in the management of post OP pain in patients who have undergone knee replacement surgery. This PICOT study seeks to confirm the prevailing impression that the use of True lavender should be more effective due to its ability to relieve pain related to stress. (Buckingham, 2000)
Statement of the Problem
Older patients who have undergone knee replacement surgery are often faced with post OP pain that should be managed effectively to prevent further complications such as neurovascular complications (Coppa, 2008). Several methods are currently being used to alleviate post OP pain. The conventional approaches include the use of NSAIDs, Opioids, nonopioids among others. There are various alternative methods to post OP pain management following a Knee replacement, this study is interested in the use of true lavender due to its ability to cause the patients to relax and therefore relieve pain caused by stress.
This is benchmarked on the demonstration that high levels of stress and anxiety result in an increased perception of pain (Moyer, 2009). Within the acute care settings, there is a lack of consensus as to which approach should be favored in the management of post-operative pain following knee replacement (Mitchinson, Kim, Rosenberg, Geisser, & Kirsh, 2007). This study will therefore seek to indicate that the use of true lavender is more effective in the management of post OP pain (within 48 hours) following knee replacement in older patients (due to osteoarthritis, fracture, or meniscus injuries), as compared to conventional medical treatment and pain medications.
Purpose of the Study
The purpose of this study is to draw a comparison between the use of true lavender and NSAIDs and Opioids in the alleviation of post-OP pain within 48 hours in adult patients who have undergone a knee replacement surgery (due to osteoarthritis, fracture, or meniscus injuries). The study intends to confirm that the use of true lavender is more effective due to its ability to relieve pain related to stress. Pain measurements will be conducted using the Numeric Rating Scale (NRS) (Aourell, Skoog, & Carleson, 2005). The results of this study will effectively enhance post-operative pain management in adult patients who have undergone knee replacement surgery.
Review of the Literature
Research data indicates that most patients who seek knee replacement procedures are adults, mainly suffering from osteoarthritis complications (Linsell, Dawson, Zondervan, Car, & Randall, 2006). Quite a number of these patients show up with fractures and meniscus injuries. Postoperative pain control is a well-known clinical challenge that occurs shortly after a knee replacement surgery (Linsell, Dawson, Zondervan, Car, & Randall, 2006). Several therapeutic techniques are currently applied in the control of postoperative pain following knee replacement (Hirvonen, 2006). These techniques are mainly categorized into conventional approaches and alternative approaches.
True lavender is often administered through inhalation or massage/M- technique massage therapy. It’s important to note M technique and massage are distinct procedures but for this study, the terms will be used interchangeably to refer to the manipulation of muscles, soft tissues, and connective tissues together with the stimulation of the skin, nerves, blood, and lymph systems (Linsell, Dawson, Zondervan, Car, & Randall, 2006).
Evidence-based research has revealed the importance of touch in contemporary healthcare practices (Wilkinson, 2004). Massage has long been used to help elderly patients lead active lives by reducing pain and maintaining mobility. Research shows that the application of diluted essential oils through massage assists in the fulfillment of the need of touch, eliminates toxins from the body, enhances mobility, restores posture, decreases all levels of stress, and helps individuals recover faster from injuries. The M technique is illustrated as a simple technique of gentle, structured touch or stroking (Roberts & Campbell, 2011). Each movement in the course of the M technique is conducted in a set pattern at a predetermined speed and pressure that remains constant. The M technique is a widely used method in aromatherapy.
Previous studies have shown that aromatherapy improves parasympathetic response as a result of the effects of both touch and smell and encourages a deep feeling of relaxation that alters the perception of pain. Analgesic effects have been documented in human studies. In a study reported by Woolfson, it was shown that a 50% pain reduction was achieved through lavender massage in 100 patients who were being nursed in a critical care unit (Alexander, 2001). Studies conducted in an animal in vitro model have shown that lavender and its main constituents, linalyl acetate and linalool have local anesthetic effects (Adams, White, & Beckett, 2010).
Generally, the analgesic properties of aromatherapy can be connected to several factors: A complex mix of unstable chemicals manipulating the pleasure site of the brain; specific analgesic factors that are found in the essential oil resulting in the stimulation of neurotransmitters such as dopamine and noradrenaline; and the interaction of touch with sensory fibers in the skin resulting in altered transmission of pain (Mitchinson, Kim, Rosenberg, Geisser, & Kirsh, 2007).
Postoperative pain following a knee replacement is conventionally controlled using medications delivered through the intravenous route. Intravenous patient-controlled Analgesia (IV-PCA) is the most common form of post-operative analgesia that is given to patients after knee replacement surgery (Ozawa & Shimizu, 2007). PCA relies on infusion pumps to deliver small doses of activated opioids. The opioids that are most commonly used with PCA include morphine ad fentanyl.
Patients are often required to give consent and be ready to give themselves a bolus when they feel pain. Opioid-related side effects are commonly observed, especially in the elderly who might get confused following PCA use (Gandhi & Viscusi, 2009). Morphine is an opioid derived from the opium poppy and usually functions by depressing the cerebral cortex, resulting in impaired concentration and reduced pain perception (Rose & Kam, 2002). Recent studies have shown that opioids such as morphine result in the depression of cough and respiratory centers. Patients using opioids for pain control run the risk of getting addicted to them. Another commonly known contraindication with opioid use is constipation (Reuben & Connelly, 2000).
Nonopioid drugs are also used in pain management following knee replacement surgery. The most commonly used drugs in this category are aspirin and acetaminophen. Aspirin (acetylsalicylic acid) is a well-known know analgesic that causes anti-inflammatory effects ad works by blocking prostaglandin synthesis in the CNS and peripheral nervous system (Hirvonen, 2006). Acetaminophen does not cause anti-inflammatory effects since it doesn’t block the synthesis of prostaglandin in the peripheral nervous system.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are also used in postoperative pain management. These drugs are most commonly indicated for patients who have undergone knee replacement due to arthritis. Aspirin belongs to this group of drugs due to its ability to inhibit factors that are necessary for the synthesis of prostaglandin synthetase enzymes (Gandhi & Viscusi, 2009). A lot of other NSAIDs exert the same effect but through different mechanisms. Previous research indicates that all NSAIDs cause increased gastric bleeding in patients suffering from gastric ulcers by inhibiting prostaglandin PGE2 which controls the secretion of gastric acid. Additionally, NSAIDs can result in prolonged bleeding by inhibiting renal blood flow, cause bronchospasm and nasal polyposis in susceptible individuals (Reuben & Connelly, 2000).
Several issues are surrounding the use of conventional medications in post-operative knee replacement pain control. Besides the obvious side effects, studies show that patients often fear getting addicted and therefore become reluctant to report pain. Opioids/Narcotics are also controlled so tightly that they are not freely available to patients at the time when they need them most (Gandhi & Viscusi, 2009). Such issues do not arise with the use of true lavender or other essential oils for post-operative pain control. Several studies have been conducted to draw a comparison between the efficacies of different classes of drugs utilized in pain management. However, no study has been conducted to compare the efficacy of these drugs with the use of lavender or other essential oils. In fact, there are only a few empirical studies that have been done to demonstrate the efficacy and safety of essential oils with humans (Roberts & Campbell, 2011).
Research questions
- To what extent (measured using the NRS) does the use of true lavender reduce pain within 48 hours of post OP knee replacement in adult patients?
- To what extent (measured using the NRS) does the use of opioids/ nonopioids/NSAIDs reduce pain within 48 hours of post OP knee replacement in adult patients?
- How does the efficacy of true lavender compare with that of conventional medications (opioids/nonopioids/NSAIDs) in the relief of post-operative pain within 48 hours in adults who have undergone knee replacement due to osteoarthritis, fracture, or meniscus tear?
Methods and Procedures
Sampling
The study will utilize a multi-site non-randomized sample to attain the required number of participants for validation. In order to be included in the study, participants will be required to be of 35 years of age and above and will have undergone a knee replacement procedure due to osteoarthritis, fracture, or meniscus tear, and will be required to have utilized true lavender (massage/ M technique or inhalation) only or conventional medication only for postoperative pain management. The study will pay close attention to the following demographic factors: gender, ethnicity, and age as they are likely to influence the outcomes. Laid-down procedures will be utilized in seeking informed consent from the participants and their confidentiality will be highly upheld.
The exclusion criteria will be as follows: Patients who are less than 35 years of age or have undergone knee replacement surgery for reasons other than osteoarthritis, fracture, and meniscus tear will be excluded from the study. Those who will have utilized a multimodal approach in post-operative pain management will be excluded from the study (Ozawa & Shimizu, 2007). Those who cannot complete the Numeric Rating Scale (NRS) for one reason, or another will also be excluded from the study.
Instrumentation
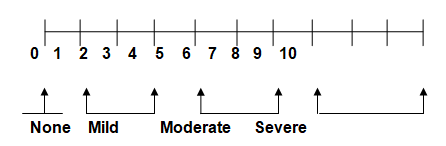
None Mild Moderate Severe
The Numeric Rating Scale (NRS) will be used to measure the perception of pain by patients who will be under opioids/Nonopioid/NSAID medication or lavender (inhalation/massage/ M-technique) following knee replacement. The measurements will be taken at the start of pain control for a maximum of 48 hours. Patients will be required to state how they perceive the pain they are feeling ad how they can rate it on a scale of 1 to 10. The NRS has potential advantages as a screening test. It is short, easy to administer, and has been validated as a measure of pain intensity in populations with known pain (Gandhi & Viscusi, 2009).
Data Collection
Pain assessments will be conducted between 13.00 and 17.00 hours. For those receiving conventional pain management therapies, the assessment will be conducted immediately before and some period after, depending on the route of drug administration. For participants in the lavender M technique/ massage/inhalation group assessments will be conducted immediately prior to the first and final lavender massage/M technique/ inhalation sessions. Onsite nurses will be required to assist the patients in the completion of the Numeric Rating Scale (NRS). The collected data will be assembled and tabulated according to the variables.
Data Analysis
Data will be analyzed using the statistical software SPSS for windows (Mitchinson, Kim, Rosenberg, Geisser, & Kirsh, 2007). T-tests and will be used to draw a comparison of the baseline variables between the different groups. The effect of lavender will be compared with the effect of the conventional medications used via repeated measures ANCOVA with hours of hospitalization (as an indication of pain duration) and the number of hours between assessments as covariates (Coppa, 2008). The study will make use of paired sample t-tests to draw a comparison between the differences in pre and post-therapy pain assessment variables. Pearson’s correlation will be used to establish the relationship between the different variables (Coppa, 2008). The significance of the tests will be set at 0.05.
Limitations and Delimitations
Pain is said to be unique to a person who is feeling it. The perception of pain varies from a person to person. The study will utilize patient-self reporting of pain and therefore there might be cases of overrating or underrating which may pose a threat to internal validity. The effects of this limitation will be reduced by assessing the pain before and after the therapy to assist the patient in drawing a reasonable comparison. The study will not include patients who have developed pulmonary or respiratory complications due to their limited ability to communicate effectively. Patients with mental conditions that are likely to influence their judgment will also be excluded from the study. The study will be focused on older patients because they are more likely to undergo knee replacement and are also able to communicate effectively.
Significance of the Study
Empirical data on comparative efficacy between conventional pain control medications and alternative approaches is conspicuously lacking. Previous studies have revealed high patient satisfaction rates with alternative therapies such as massage and M technique. If this study ascertains that the use of true lavender is reasonably effective in post-operative pain control, as compared to conventional medications, then this will positively impact healthcare (Buckingham, 2000). Further studies can be conducted to evaluate the same in other healthcare specialties to examine how alternative approaches can be utilized fully to prevent the effects associated with conventional medicine.
References
Adams, R., White, B., & Beckett, C. (2010). The Effects of Massage therapy on pain management in the acute care setting. International journal of therapetic massage and bodywork , 3(1):4-11.
Alexander, M. (2001). How Aromatherapy Works: Principle Mechanisms in Olfaction. Odessa, FL: Whole Spectrum Books.
Aourell, M., Skoog, M., & Carleson, J. (2005). Effects of Sweddish massage on Blood pressure. Compliment Ther Clin Pract , 11(14):242-246.
Buckingham, C. (2000). Effects of Aromatherapy o PMS. New York: Buckle Associates.
Coppa, D. (2008). The internal process of therapeutic touch. J Horlist Nurs , 26(1):17-24.
Gandhi, K., & Viscusi, E. (2009). Multimodal pain management techniques in hip and knee arthroplasty. The Journal of New York School of Regional Anesthesia , (13): 1-10.
Hirvonen, J. (2006). Health-related quality of life in patients waiting for major joint replacement. A comparison between patients and population controls. Health and quality of life outcomes , 4 (10):1186- 9.
Linsell, L., Dawson, J., Zondervan, K., Car, A., & Randall, T. (2006). Pain and overall health status in older people with hip and knee replacement: a population perspective. Journal of public health , (28):267-273.
Mitchinson, A., Kim, H., Rosenberg, M., Geisser, M., & Kirsh, M. (2007). Acute postoperative pain management using massage as adjuvant therapy: a randomized trial. Arch Surg , 142(12):1158-1167.
Moyer, C. A. (2009). Affective massage therapy. Int J Ther Massage , 1(2):4.
Ozawa, T., & Shimizu, K. (2007). Evaluation of patients’ satisfaction after total hip arthroplasty. Journal of Physical Therapy Science , (19):139-143.
Reuben, S., & Connelly, N. (2000). Postoperative Analgesic Effects of Celecoxib or Rofecoxib After Spinal Fusion Surgery. Anasthesia and Analgesia , 91: 1221-5.
Roberts, K., & Campbell, H. (2011). Using the M technique as therapy for patiets at the end of life: two case studies. International journal of palliative nursing , 17(3):114-118.
Rose, M. S., & Kam, P. (2002). Gabapentin: Pharmacology and it’s use in pharmacology. Aesthesia , (57): 451-462.
Wilkinson, J. (2004). Aromatherapy practice in nursing: Literature review. Wagga Wagga: Blackwell.