Introduction
In today’s competitive business scenario, it has become critical for organisations to give priority to customer service and satisfaction. Such priority is more crucial for the service industry such as health care. Due to increasing competition, private sector companies engaged in health care are forced to prioritise customer service. On the other hand, public sector enterprises are bound to serve the people due to government’s obligation towards its citizens.
The task of evaluating customer (here, patient) satisfaction has emerged as a separate industry and that too, a major one. Several companies are engaged in conducting health care surveys that target patients as respondents. Such surveys bring forth the patients’ perspectives about their experiences while availing health care facilities. Asking the patients directly is probably the best way to know their feelings about the quality of health care and personal services provided to them during their treatment. This exercise can help health care organisations in assessing and improving their services so that patients can avail better care and feel happy (White 40).
During the past couple of years, customer satisfaction evaluation has witnessed great participation by various evaluating companies. However, the health care sector has not been able to keep up the pace of gauging their patients’ satisfaction. Reports suggest that patients’ opinion about the health care services is not encouraging. They feel that doctors, nurses and other health care professionals are more concerned about the technical features of the treatment rather than the individual requirements of patients. Current advancements in the medical scenario have necessitated health care professionals to consider patients as a crucial part of their success (Powell 1).
Earlier, the term ‘customer care’ was apt for the hospitality industry (hotels, restaurants, etc.). Due to intensive competition among health care facilities, the term has become inseparable from this sector as well. Organisers of such facilities are aware of the fact that patients are free to choose health care facilities for treatment. As such, they try to attract patients by providing better patient services (Slowiak, Huitema and Dickinson 112).
Project rationale
The purpose of this study is to investigate and understand patients’ perception after having availed health care services at public hospitals in Abu Dhabi. The author aims at assessing the level of satisfaction among patients of these hospitals. This study will help the public hospitals to understand their patients’ perceptions about services being provided during and after treatment. This will help them in identifying their drawbacks, which may be rectified for offering better services. After completing this project, the author is optimistic of attaining excessive knowledge about the importance of patient satisfaction in the health care industry.
History of customer services in health care facilities in the world
Over the years, the health care industry has experienced massive changes in its approach towards services being offered to patients. Such changes have been influenced by the growing awareness of patients regarding their rights and privileges. The situation is more related to public hospitals that are managed by governments. Private hospitals have different reasons for enhancing the quality of their services. As a result, patient satisfaction has become the most sought-after feature in health care industry. Patients’ level of satisfaction or displeasure suggests the quality of services being provided at health care facilities. Better services offered to patients guarantee dual benefits: patient satisfaction and better image/status.
The term “hospital” has been derived (as a combination) from Latin words that signify guest and hospitality. It means that hospitality was one of the major concerns during the times when the concept of hospitals was started. During those times, hospitals were meant to serve the pilgrims who came back after visiting the Holy Land. People working at hospitals served such pilgrims without any intention or motive.
Patients’ viewpoints pertaining to health care services portray hospitals as daunting and inhospitable areas (Torcson 1). Patient satisfaction is basically a reaction of experiences during treatment (Sharma and Kamra 130). It relates to the service aspect rather than the technical aspect (pertaining to the quality of treatment). Majority of the patients do not complain about the quality of treatment being provided; they are more concerned about the services being offered. People are of the opinion that hospitals ought to provide appropriate treatment otherwise they would land up in the court. As far as services are concerned, it is up to the hospitals to decide the quality (Torcson 1). The main aim of hospitals should be to complete appropriate treatment of patients within the minimum possible time frame. Patients want to get out of hospitals at the earliest. The sooner a patient gets treated the level of satisfaction would be higher (Sharma and Kamra 130).
Nursing profession is a critical part of service to patients. It comprises of assisting the patients in observing cleanliness, following a nutrition and exercise regime, maintaining ecological sanitation, assessment, keeping up body temperature, giving security and solace, assisting in breathing, giving wellbeing training, and so forth. Nursing profession is obliged to maintain good health of patients and ensure comfort of their patients.
The psychology or mindset of people (here, patients) plays an important role in making choices or preferences. It is a general perception that hospitals in developing and under-developed nations are not up to the required standards of health care. On the contrary, patients in Western countries are not worried about the quality of service and treatment provided at hospitals. The reason is that the standard of hospitals in Western countries is already so high that the level of patient satisfaction is more as compared to that in developing and under-developed nations. Considering health care facilities in Gulf countries, it would not be undermining to mention that the quality and infrastructure are in tandem with those in western countries. Gulf countries have enough resources to maintain a standard similar to that of the western countries but the appropriate use of these resources has to be justified as being optimum (Margolis et al. 242).
Once the British withdrew from Abu Dhabi, it became an independent state (emirate). After becoming the head of state of Abu Dhabi, late H. H. Sheikh Zayed Al Nahyan initiated attempts to improve the health care system of the emirate. Health care services started being managed by the government. Gradually, as the emirate’s economy improved, better infrastructure (in line with the economic enhancement) for the health care sector was introduced. The General Authority of Health Services (GAHS) was formed in 2001. In order to have better control over the overall health care system, the emirate was divided into four regions namely, “Abu Dhabi City, Al Ain, Middle Region and Western Region” (SKMC 1).
During his tenure as the ruler of Abu Dhabi, H. H. Sheikh Khalifa Bin Zayed Al Nahyan made health insurance compulsory for residents (both locals and foreigners) of the emirate. The new law made it obligatory for business organisation to “provide health insurance coverage for their expatriate employees and their families” (SKMC 1). The government shouldered the responsibility of providing health insurance coverage to its citizens. In pursuance of this endeavour, the government established The National Health Insurance Company (Daman). Daman was responsible to provide health insurance coverage to Abu Dhabi citizens and also formulate the “Abu Dhabi Plan” (for foreign workforce working in Abu Dhabi).
The year 2007 witnessed a bifurcation of GAHS into two separate entities namely, ‘Health Authority of Abu Dhabi’ (HAAD) and ‘Abu Dhabi Health Services Company’ (SEHA). While HAAD was given the authority of controlling health care, SEHA was responsible for the execution part. SEHA manages the operations in all government hospitals of Abu Dhabi; it allocates contracts to renowned and experienced global health care organisations to operate such hospitals (SKMC 1).
Literature review
Relation between staff and patient satisfaction
The role of staff in attaining patient satisfaction cannot be undermined. Health care sector is indisputably a multifaceted one. There are several factors related to this sector that keep on changing with time, such as: policies, laws, research, expertise, and paraphernalia. In addition, new diseases – and their treatments – and the diversity of people (various staffs) who deal with the patients have added to the complexity. There are scholars who believe that it is always advisable to try and prevent diseases in comparison to treating them. Such scholars feel that the quality and costs of treatment can be controlled only if such a policy is adopted (Mossberger 1). In spite of all such arguments, the fact remains that the employees of health care facilities are the ones who play a crucial role in achieving optimum patient satisfaction.
Research proves that in order to achieve better patient satisfaction ratings, it is crucial to ensure employee satisfaction (Larson 1). In today’s competitive scenario, health care facilities around the globe are adopting ways and means to make sure that their employees are satisfied. It is thus understood that better levels of employee satisfaction can be instrumental in attaining higher levels of patient satisfaction. It can thus be implied that if the employees are satisfied, the possibility of patients also being satisfied is higher. A work atmosphere conducive to employee satisfaction can help reduce death rates (within the health care facility) and unsuccessful rescue attempts. On the contrary, if employees are not satisfied with their jobs, they would not perform their duties whole-heartedly and might commit certain mistakes or errors that may prove harmful for the patients. The correlation between staff and patient satisfaction was established by Matthew McHugh in his study, which revealed that 10% of staff discontent resulted in a decline of 2% in patient satisfaction (Larson 1).
Patients are also human beings and as such, they have an understanding of human behaviour. Though they may not understand the technical details of their treatment, the displeasure among the staff (if any) is not hidden from them. Gradually, such displeasure overtakes the patients as well that results in lower ratings of patient satisfaction. It is thus very important to have employee engagement in health care facilities. Research shows that there are five main decisive factors that augment employee engagement (Halogen Software 3).
In cost-cutting measures being adopted by global businesses, health care sector was no exception. Policies pertaining to finance (mainly expenses) are changed frequently and in doing so the health care facilities sideline the cause of patients’ wellbeing. Due to less treatment resources, nurses feel detached and due to less vested powers, they are unable to offer the required care to their patients. In such cases, there are chances of nurses quitting their jobs because they sense the unrewarding nature of their job (Peltier and Dahl 7).
Role of technology in attaining patient satisfaction
Health care is among the sectors that lack sufficiency pertaining to adoption of technology and its utility. The turbulent health care market has been inundated by increased patient demands, declining margins, constant revisions of the current laws and restrictive laws. The health care sector is increasingly viewing IT as a basic asset in the provision of decision support and health related services, as well as managing the increasing costs of health care. Advancement in technology has influenced the manufacture, distribution, and even administration of health care equipments and medicine. The medical world is now full of machines and bioengineered equipments that require a certain degree of technological proficiency to operate. Moreover, technology has also empowered customers to seek and access their health care rights and information. Customers can now use current technology to assess the credentials of medical practitioners. Negligence and errors in medical treatment that were witnessed before the inception of modern technology have reduced.
Technology has enabled health care professionals to treat critical diseases but at the same time the cost of such treatments has increased, making it out of reach for most of the patients. The concerned departments do provide subsidy for the costly technology but that too is for a limited period and only for select technologies. Owing to the adoption of new technological methods of treatment, the cost of health care has also risen in the past few years. Medical technology is expensive and hence today the cost of medicine and medical services has risen. Modern technology has also been credited with the current increased level of accuracy in medical treatment. There are various ways in which technology has aided in the compliance of medication requirements for patients.
One drawback that new technology has is the cost factor. In some cases, cost limits the adoption of basic medical technologies. Considering this aspect and due to excessive developments in medical technology, the government has to do higher spending in the health sector (Bardhan and Thouin 443). The benefits of the spending should be weighed against the efficacy of the technology in attaining patient satisfaction. Information technology can have a great impact on the variety of jobs and their necessity. As is understood, new technology needs appropriate knowledge. The health care employees who can adapt to the change will continue and those who can’t will be eliminated. New technology has even changed the approach of the patients. Patients now prefer to contact the doctors via emails. This has reduced the regular visits by patients to health care centres. Obviously, this aspect has reduced the need of more health care employees. Modern technology and medical informatics are quickly taking over some of the traditional roles that were played by medical practitioners (Korzep 354).
There have been ongoing discussions on whether the investment done by health care centres on new technology is necessary and whether the new technology will be able to sustain itself. It is understood that initially, such new technologies might receive subsidies from charity organisations or the government. Sustenance in health care means that with time any particular machinery becomes self sufficient (doesn’t need any external aid or grant).
It may be argued that while adoption of new technology has improved medical treatment, it has also increased the cost. Another drawback of new technology is the reduction in the job opportunities. The new technology also needs adequate training that again involves cost and time. Specialised personnel are required to handle such technology. A small mistake in handling such technology might be disastrous. So there are both pros and cons of technology.
Need of urgent care centres
The current global health care system is struggling with the problem of over stretched hospital emergency department capacity, limited clinicians to provide primary care as well as constant increase in health care cost. As such, urgent care centres have come out as an option to the increasing health problems that need immediate attention. Patients are more concerned about getting better treatment at economic rates (Galewitz 1). Essentially, urgent care units have been perceived by the populace as critical in improving accessibility to immediate medical services at affordable costs (Landen 1). Besides, the growth in urgent care centres in the recent past indicates the patients’ increased demand for immediate medical services. In fact, urgent care centres offer medical services for minor illnesses and injuries that need pressing consideration. However, the centres are not fully equipped to handle complicated emergencies.
Studies indicate mixed data on the impact of urgent care centres on health care. However, the rising optimism among the health professionals and the public indicate positive effects in terms of costs and accessibility to medical services. In most cases, urgent care centres have contributed to reduced visits and long queues in hospital emergency departments. Other studies directly link urgent care centres to increased accessibility and reduced health care costs. Moreover, most studies indicate that the increase in the number of urgent care centres can be attributed to customers’ requirement to have easy approach to the required treatment. While the growth in urgent care centres is seen as disruptive to the health care coordination in some quarters, proponents argue that the concerns may be overstated given the fact that urgent care centres put much emphasis on intervallic and uncomplicated health conditions instead of chronic and multifaceted cases (Japsen 1). The future growth potential of urgent care centres is bright given the expansion of heath care coverage under the health care reforms. The expansion of health coverage would lead to increased pressure on both primary and emergency care living room for the growth and expansion of urgent care centres.
Urgent care centres have proliferated and grown considerably in the last two decades. The rapid growth and development of the urgent care centres has been attributed to the inefficiencies in the primary care deliveries, crowded emergency departments and the need to for increased accessibility to immediate medical attention. Essentially, urgent care centres provide medical services based on walk-ins. Besides offering the medical services during the regular business hours, urgent care units offer their services during weekend and evenings. In most cases, urgent care centres offer medical services usually provided by primary care units ranging from flu to minor ear or eye infections. Contrary to hospital emergency departments, urgent care units are not fully equipped to deal with complex medical services situations. In terms of staffing, physicians with professional backgrounds in emergency medicine or primary care manage urgent care centres (Galewitz 1).
Origin of urgent care centres can be traced back to the early eighties. Such centres could not garner popularity and acceptance because the promoters did not have a suitable plan. However, demands for urgent care units have been increasing consistently as the need for increased accessibility and efficiency in emergency medical services increases (Japsen 1). Current studies linking primary care physicians and health care services delivery indicate deteriorating provision of health services particularly during the extended hours. The void is filled by urgent care centres prompting their rapid growth in the recent past (Landen 1).
Before, urgent care centres were being managed and owned by independent private entities. However, increased growth and expansion of urgent care centres have led to large units being managed by big hospitals and chain of entities (Japsen 1). Moreover, hospital systems are expanding in urgent care systems to increase their services offerings. Besides, insurers have also embraced the low cost systems of urgent care centres thereby shifting some of the medical care from emergency departments to urgent care centres. Essentially, insurers believe that urgent care centres cost less compared with emergency care departments.
Importance of health care professionals being culturally congruent
Culture is a typical kind of characteristics of people having many things in common such as speech, communication style, creed, faith, beliefs, food habits, social traditions, music, arts, etc. These aspects keep on changing with the passage of time. Now what is culturally congruent care? It is basically the care that is provided by a compassionate, proficient, and culturally perceptive nurse or any other health care provider. Moreover, it is a human right rather than an obligation to receive equivalent treatment (Jeffreys 18). In other words, when the cultural aspects of patients are considered and there is no bias in the treatment, then it is a culturally congruent care.
Due to the rapid expansions of multinational companies, there has been an incessant increase in the quantum of migrating populations. The changes in the characteristics of such populations, the unstable fertility rates, and advancement in science and technology have resulted in an overall cultural revolution. Owing to such developments, there has been a need for change in the nursing practices worldwide. The current requirement pertaining to pain is that the nurses should be taught how to tackle the culturally diverse patients. It is the need of the hour that the concept of culture is included in nursing education and implementation of management skills.
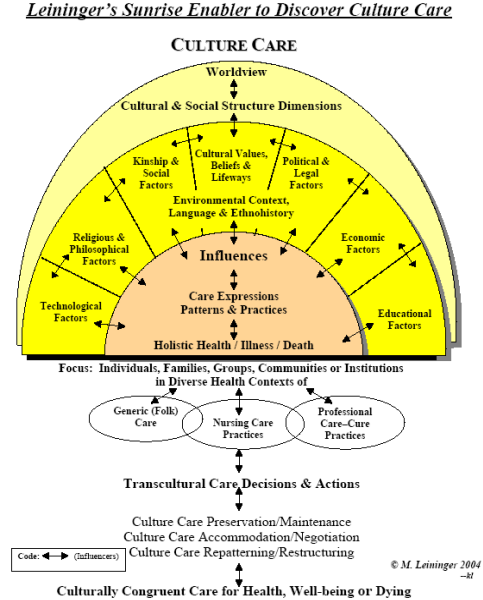
It is not as easy as it seems, to understand different cultures and offer treatment accordingly. It’s a huge task to get details from each and every patient about his/her culture. Moreover, there are many cultures around the world where the health and sickness of an individual is associated to God and Saints. Also, there are certain medicines that the nurses might not have heard of before. But it becomes improper to bluntly neglect all such things when such a patient comes for health care assistance. In such circumstances, it becomes very difficult to have the same health care approach for the patients. Appendix 1 depicts a model for optimum culture care.
Language is yet another problem that is very critical. In health care segment, it is very important for a patient to make the health care provider understand the problem being faced. Language plays a crucial role in explaining. Similarly, it is very important for health care professionals to understand their patient’s problems. Most of the times, nurses and other health care professionals are able to understand their patients’ problems but in circumstances where language poses a problem, the patient is not satisfied. Such incidents prove to be harmful for both the parties. On one hand, the patient is unable to receive medical attention (sometimes, such attention is required urgently) and on the other, the health care facility loses trust and credibility. This might result in bad publicity among that patient’s acquaintances and they might not want to utilise the services of that particular health care facility in future.
As such, each and every one of us is entitled to have health care that corresponds with culture. Observations from some studies indicate that the culturally motivated health care and the performance of health care are interrelated. This means that if a health care institution adheres to the culturally congruent health care for all its patients then the overall performance of that institution will be appreciable, and vice versa. The astounding number of legal cases claiming of improper health care suggests that the legal implications can be serious. The nurses are not only bound morally but legally as well to provide better health care, indifferent to culture.
If the moral values are considered by nurses and other health care providers, most of the problems relating to culturally congruent health care will automatically be resolved. If this may be the case, then they will “come simply to perceive the morally relevant aspects of situations and so to adopt a moral perspective on them without deliberation (unless the situation is unusually confusing or unclear)” (Huddle 2005). This is a very practical way of overcoming the problem of culture in nursing. If in any situation the nurses consider the moral values, there is no way that they will disregard the problems being faced by patients of different cultures.
Pain Management
In order to have a perfect understanding of their patients’ pain, nurses need to have optimal knowledge of the pain assessing skills and patient attitudes. At the same time, it is very crucial for the nurses to have a thorough knowledge of pain management. Such skills and management should be substantiated by suitable evidence on hand so that the patient doesn’t have to suffer much. Usually, patients are not ready to experience pain once they are under the care of any particular hospital. In fact, they are right in this approach because hospitals are meant to give optimum relief to their patients. Simultaneously, it is not acceptable on the part of nurses to have insufficient understanding of their patients’ pain. It is an ethical or moral responsibility of nurses to be accountable to their professional job profiles. The severity of pain assessment and management can be gauged from the fact that the Royal College of General Practitioners, UK, decided to make chronic pain as a priority.
Nursing programmes may as well add pain as a mandatory segment to educate future nurses about the skills and aptitudes required for handling patients who are experiencing acute pains. This will help them (the nurses) in assessing and managing pain with expertise from the very beginning of their professional careers. As a result, the patients will not have to bear severe pain and the potential risks of continuous pain might be decreased. Such care by nurses would definitely augment the patient satisfaction ratings.
Strategies to success to provide excellent health care services for all SEHA health care facilities
Making appropriate strategies that are conducive to growth, popularity and better image is crucial for any business. Likewise, all SEHA health care facilities need to adopt such strategies. In addition to the already available features, incorporating the following could prove to be beneficial for the facilities:
- Nurse-patient ratio: It is obvious that if there is less number of nurses, they would not be able to provide the required care to each patient because they will have to take care of all the patients. On the contrary, if there are a limited number of patients under each nurse, the care could be personalized (Silow-Carroll 2). It is advisable to have a ratio of 1:4 (one nurse for every four patients) for the medical or surgical departments. Considering the significance of Critical Care Units, the desired ratio should be 1:1 or maximum 1:2 (one nurse for every one or two patients).
- Nurse-patient relationship: The relationship between nurse and patients should be that of care and cooperation. In order to have optimum results of any treatment, the cooperation should be mutual. Such awareness should be spread among the nurses and patients and they should be educated on the importance of cooperation. Simply by paying the requisite fee, patients do not become free from their responsibilities. They have to cooperate with the nurses and other health care professionals by obeying the given instructions.
- Even though an evaluation of services is in place at all SEHA health care facilities, the frequency should be increased. While requesting the patients for a feedback, it is advisable to include the names of the health care professionals who attended them. This way, instead of a general feedback, a personalized feedback would be available and individuals will be able to identify their positive and negative points.
- Health care professionals who score low in patients’ feedbacks should be asked to undergo training and polish their skills.
- One issue that might not have been raised earlier is a bit complicated to understand; the ambulatory service of SEHA should have details of vacant beds in all the related/connected health care facilities and also the availability of specialized doctors and nurses. Ambulatory services are generally used for emergency situations. It is quite possible that when a patient is brought to a particular hospital, there might not be any vacant bed or the concerned doctor might be unavailable. In such circumstances, the patient has to be taken to another hospital. If the ambulatory service has such details, the patient can be taken directly to the hospital where the conditions are met. This way, precious time (and life) could be saved.
Recommendations to make standards for all SEHA hospitals for patient satisfaction
SEHA has a set of standards to be maintained in order to fulfil its commitment towards the staff, patients, shareholders, and the government. All the concerned people and bodies are responsible to abide by the standards that steer the organization towards achieving its vision and mission objectives. The present standards include those pertaining to leadership responsibilities, patient care, outsourcing of management, rights and duties of staff and patients, etc.
All other things seem to be proper except the fact that the management is outsourced. It is sensible to take heed from successful health care organizations but the policy of outsourcing management will lead SEHA nowhere. It is understood that at present the outsourcing is required in order to maintain high standards of care. Does it mean that SEHA will be managed by foreign companies in future as well? Why? Are there no competent locals who can manage such facility? If at all the locals require any training, SEHA can shortlist candidates and send them for training for six months or may be one year. Once they finish their training, they can take over the charge of management. In my opinion this is the one recommendation that SEHA should include in its code of standards. The organization should specify a date after which outsourcing of management would be stopped and all the hospitals would be managed by locals of Abu Dhabi (or even other emirates).
Applying experiences of global hospitals in SEHA health care facilities
For the purpose of this study, the services provided at Parkwest Medical Centre will be taken as guidance. The health care centre started its operations in 1973 at Tennessee. It has 462 beds and is presently managed by the Covenant Health group. Parkwest follows a reward policy for its employees. Appropriate training is provided to all managers and even the members of the board of directors. After witnessing the success and patient satisfaction ratings of Baptist Hospital, Parkwest adopted its (Baptist Hospital’s) strategies. Managers and other superiors are rated according to the ratings received by their subordinates (Edwards 2). Such a policy can also be incorporated in SEHA’s health care facilities. This will act as a motivating factor for the employees to perform better.
Case study
Al Mafraq Hospital
Al Mafraq Hospital is one of the leading hospitals in Abu Dhabi and has been operational since 1983. The operational contract for the hospital has been given to Bumrungrad International. It has a capacity of 466 beds with an ongoing expansion to add 750 beds (by the year 2016).
As mentioned earlier in the paper, the main concern of patients is to get best treatment in minimum possible time and at economic rates. Waiting time is of great significance because it can annoy or please, depending on the amount of waiting time, the patients. As such, it becomes imperative to investigate this aspect at Al Mafraq Hospital. In addition to the waiting time, there are other aspects within the in-patient and out-patient departments that contribute towards patient satisfaction. The hospital has an option where patients can fill a complaint form. Prompt action is taken on the complaints and the complainants are informed about the actions taken. Al Mafraq Hospital conducted a patient satisfaction survey, the results of which are discussed below.
A quantitative methodology was adopted to investigate the desired aspect. A questionnaire was formulated for patients who had availed the services of Al Mafraq Hospital in recent past (about a fortnight ago). Patient data was passed on to GRMC, who in turn contacted the patients. A method of face-to-face and telephonic conversation was adopted to ask questions to such patients. Since patients at Al Mafraq Hospital are from cultures with different languages, care was taken that the operators (those who were entrusted the job of asking the questions) were conversant with languages such as Arabic, English, Urdu, Farsi, and other prevalent languages (in UAE). Demographic details pertaining to name, age, gender, country of origin, etc. and other details such as contact number and hospital visiting date were included in the details provided to GRMC.
Further, the questionnaire was formulated under the guidance of HAAD officials. “Approximately 1,150 interviews were conducted of which 806 were completed and validated” (GRMC 4). Following are the results of the survey:
Inpatient department
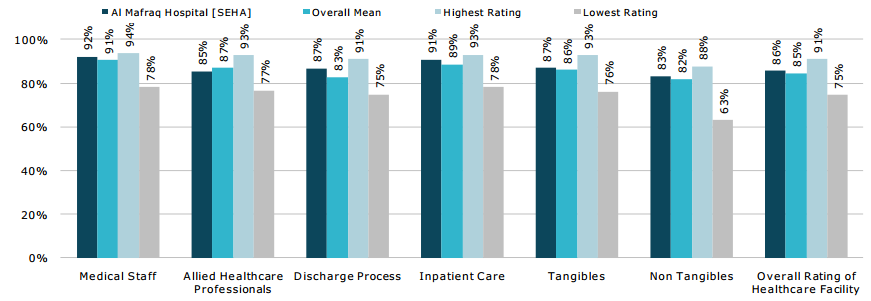
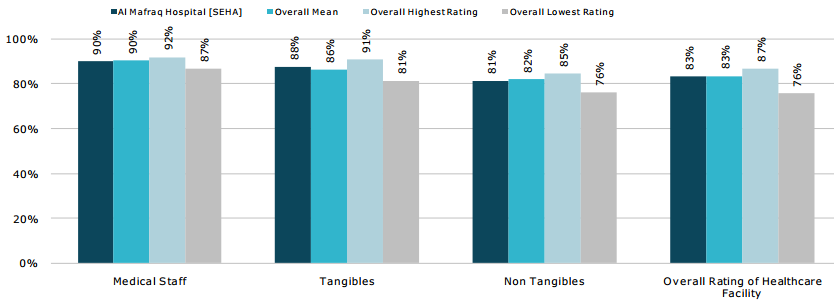
As is evident from figure 1, the in-patient department components that were included in the questionnaire were medical staff (92%), allied health care professionals (89%), discharge process (87%), inpatient care (91%), tangibles (87%), non-tangibles (83%), and overall rating of health care facility (86%). The results were quite encouraging because all the results showed patient satisfaction above 80%, with the highest level being 92% (pertaining to the medical staff). The overall ratings suggested patient satisfaction of 86% as compared to highest rating (in other hospitals) of 91% and lowest rating (in other hospitals) of 75%. Two points are of specific importance here: highest rating and lowest rating. Figure 1 depicts that in comparison to the highest rating, Al Mafraq Hospital’s patient satisfaction rating for all the components is less. This means that some of the other hospitals have better patient satisfaction rating than AL Mafraq Hospital. This implies that there is a scope of improvement in all these in-patient components. On the other hand, it can be seen that in comparison to the lowest rating, Al Mafraq Hospital’s patient satisfaction rating for all the components is high. Obviously, this means that Al Mafraq Hospitals services pertaining to the in-patient components are better than some of the other hospitals.
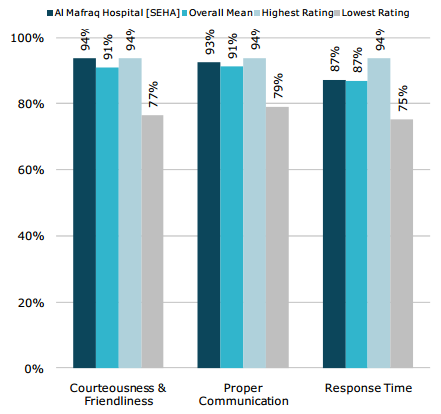
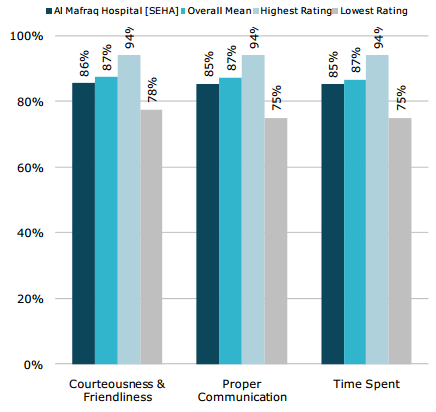
Health care professionals and the medical personnel are the ones who deal directly with the patients. Their way of dealing with the patients decides the level of patients’ satisfaction. The survey included aspects such as courteousness & friendliness, proper communication and response time in the questionnaire to get patients’ perceptions. It has already been discussed earlier that waiting time is an important aspect of patient satisfaction. In addition, proper communication (understanding the exact problems and requirements of the patients) and courtesy are also significant. The following figures (2 and 3) depict the results of such aspects pertaining to the medical staff and other allied health professionals. As is evident, Al Mafraq Hospital’s patient satisfaction rating for the three aspects is higher than the overall mean (of all hospitals considered). Here again, it is observed that Al Mafraq Hospital’s patient satisfaction rating for the three aspects is less than the highest rating (in comparison to some other hospitals). This implies that there is a scope of improving the related services. On the contrary, as compared to some other hospitals, the rating is high.
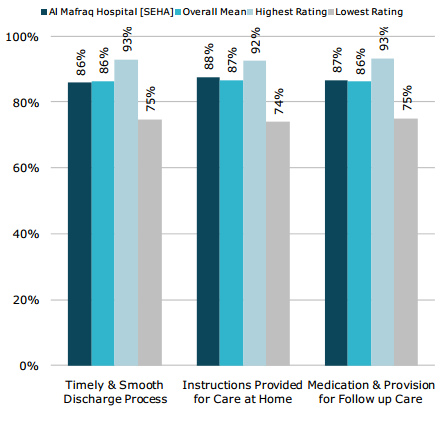
The questionnaire also contained questions pertaining to timely & smooth discharge process (86%), instructions provided for care at home (88%) and medication & provision for follow up care (87%). Figure 4 depicts the respective results. These three aspects, related to the discharge process can be considered to be the final touch in patient satisfaction. Likewise the earlier results, here also, Al Mafraq Hospital’s rating is either low or high in comparison to some other hospitals but considering the overall mean, Al Mafraq Hospital’s patient satisfaction rating is high.
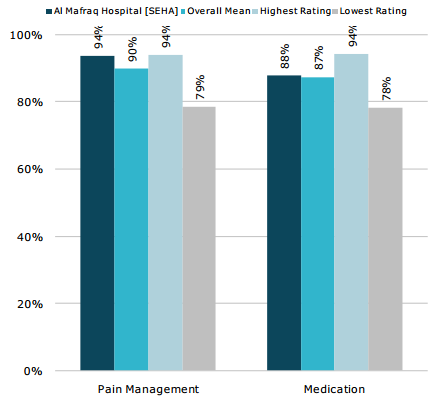
Patients visit hospitals to get treated for various diseases. Most of the diseases are accompanied by acute pain. Hospitals and the concerned health care professionals need to understand the severity of a patient’s condition who is suffering from such pain. Pain management is an altogether different subject that needs vast knowledge and experience. Similarly, proper medication is also important. Appropriate diagnosis and subsequent medication can heal the patient early. Al Mafraq Hospital’s patient satisfaction rating for these two aspects is encouraging it is higher than the overall mean. Figure 5 depicts the corresponding results. Since pain management is a crucial aspect of health care service and patient satisfaction, the topic has been briefly discussed later in the paper.
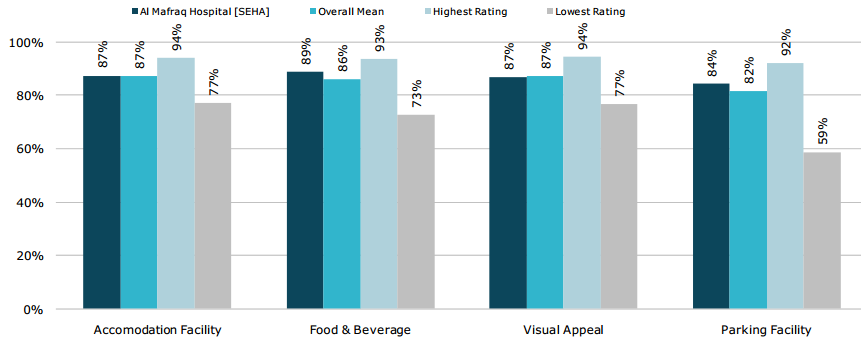
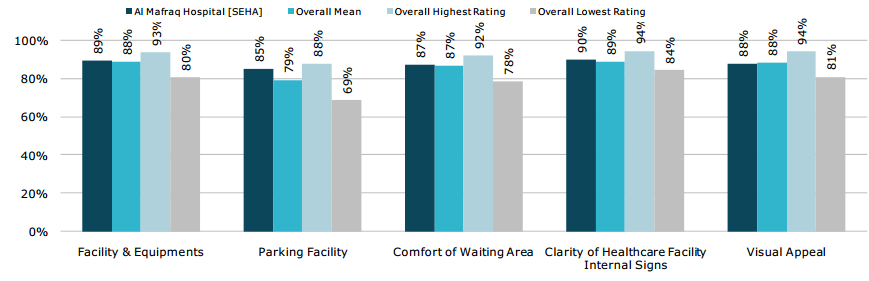
Tangible features such as accommodation facility, food & beverage, visual appeal, and parking facility were also considered in the questionnaire. Al Mafraq Hospital’s rating for patient satisfaction in these areas also exceeded the overall mean rating. Again, there is scope for improvement since there are certain hospitals that have a higher level of patient satisfaction in these areas. Figure 6 depicts the corresponding results.
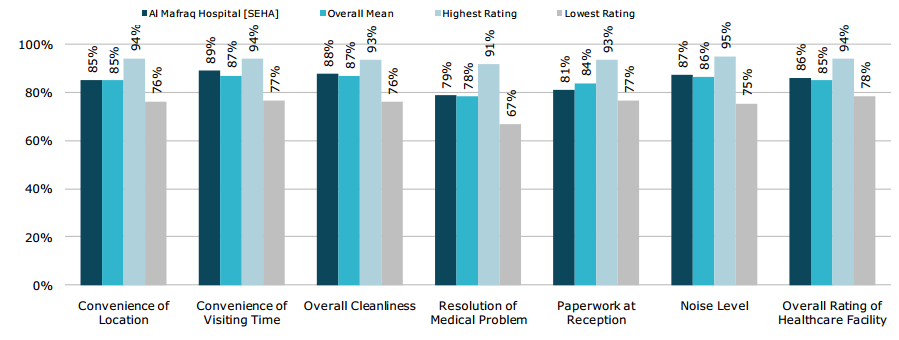
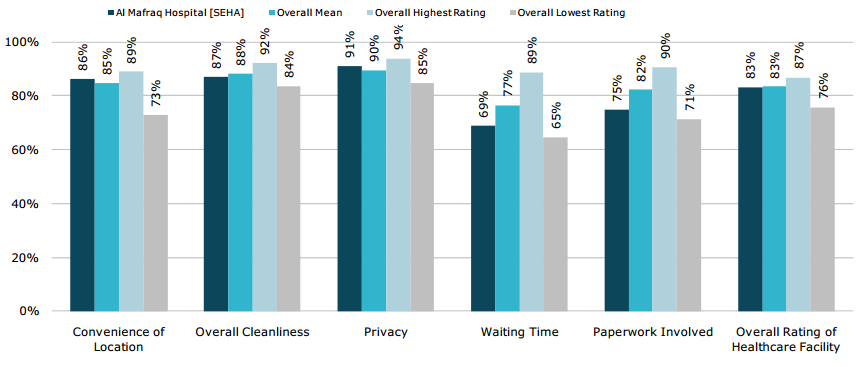
Similarly, non-tangible features such as convenience of location, convenience of visiting time, overall cleanliness, resolution of medical problem, paper work at reception, noise level, and overall rating of health care facility were are also considered. Except paperwork at reception, all other features received ratings that were higher than the overall mean ratings (of other hospitals).
Out-patient department
Following are the results of the survey questionnaire pertaining to out-patient department. The results depict that even though Al Mafraq Hospital’s various ratings for patient satisfaction in this department are higher than those of other hospitals, there are still certain hospitals where the respective ratings are higher. This implies that in the out-patient department also, there is scope for improvement. Figures 8, 9, 10, and 11 depict the corresponding results.

Analysis of “waiting time” at Al Mafraq Hospital Pharmacy
In addition to the aforementioned questionnaire survey, the author also consulted the quality department of Al Mafraq hospital to inquire about patient satisfaction in regard to the waiting time. The personnel at the quality department were very helpful and furnished the required details. The initial aim of investigating the waiting time at pharmacy of Mafraq Hospital in comparison to the service offered was attained; figure 12 depicts the waiting time. It is evident from the chart that during 2013, waiting time continued to decrease from one quarter to another; in Q1 it was 30 minutes, reduced to 15 minutes in Q2; this shows that the pharmacy service improved at Mafraq hospital in the first two quarters but deteriorated thereafter for reasons that will be discussed later.
Mafraq hospital is focusing on reducing waiting time, as it is considered to be the most essential need of customers that must be fulfilled to serve them in an excellent manner. This finding is supported by previous researches, where it was found that one of the major sources of customer dissatisfaction is the amount of time they wait when they visit health care centres. A survey was conducted to know the expectations of patients regarding the entire visit for medical care. It was found that 48% of the respondents felt that to get an appointment quickly was most important; 34% of the respondents said that time taken when a visit to a doctor is critical is the most concern for them, 44% of respondents claimed that short waiting time at the health care centre when visit to a doctor is one of the most essential requirements out of three previously mentioned requirements. Several researchers have conducted an investigation on identifying the relationship between customer satisfactions and waiting time for service to be rendered in health care organisations.
It is observed that in the first quarter of 2013, waiting time was 30 minutes; it reduced to 15 minutes in the second quarter, showing a positive improvement in the service. However, in the third quarter of 2013, waiting time increased by 22 minutes to 37 minutes but further reduced to 27 minutes in the fourth quarter of 2013.
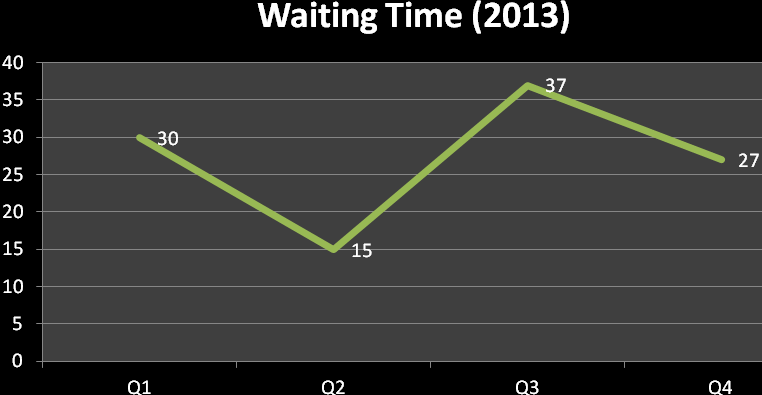
The sudden jump in the 3rd quarter indicates that there was an issue that needed to be solved since waiting time was dramatically increased. Even though the fourth quarter results showed improvement the service still couldn’t be considered as best practice and efforts to sustain the downward trend had to be made.
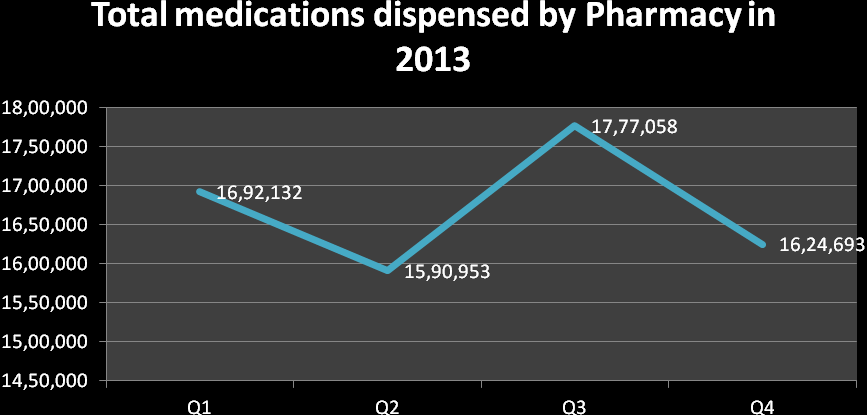
Investigation into what caused the second quarter improvement revealed only a slight decrease in volume of medications dispensed, thus no deliberate actions had been taken, which could be replicated. Further investigation and research had to be conducted to look for reasons of third quarter deterioration and try to eliminate these. Factors contributing to this spike in waiting time in the third quarter were analysed and found to be the following:
Medications dispensed by the pharmacy for inpatients, outpatients and to customers visiting the service from prescribers outside of the facility as per figure 13.
- Manpower challenges encountered, resulting in the closure of service counters in Q3:
- 2 pharmacists each went on 90-days maternity leave
- 1 pharmacy technician had unexpected long term sick leave
- 2 pharmacy technicians and 1 pharmacist resigned without replacements appointed in time
Al Mafraq hospital is familiar with these issues and is trying to cope with its unsatisfied customers. This finding is supported by previous research stating that in the health care industry, service quality is the level where health care service providers deliver services to individuals and the society to increase the probability of desired health outcomes and remains consistent with the current knowledge of professionals.
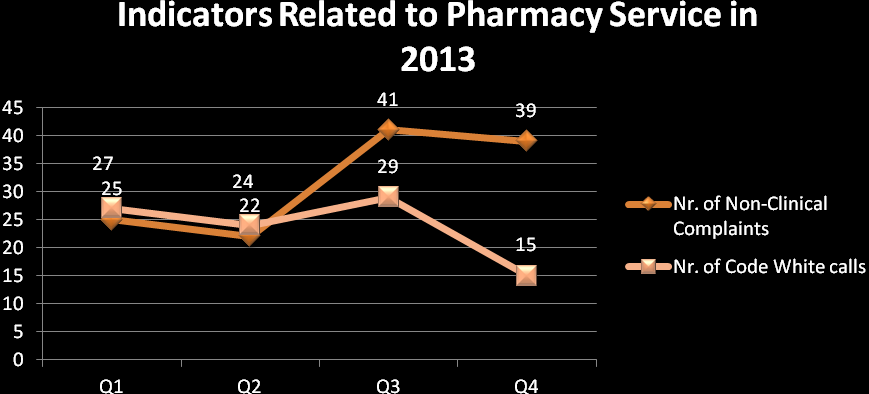
Two indicators of customer dissatisfaction that were analysed are “Code White” calls (angry patient) and non-clinical complaints. In 3rd quarter there were 29 Code white announcements, of which 24 related to impatience with waiting time; 5 related to staff attitude. In 4th quarter the total number decreased to 15; 13 thereof being the result of waiting time. Non-clinical complaints pattern almost followed the waiting time pattern, as per figure 14.
Analysis of service quality from an outpatient perspective
A representative sample of outpatients were asked to rate the customer service with respect to waiting time encountered; waiting time referred to as waiting to see the physician after registration. The trend from January 2013 to December 2013 was analysed and found to be unstable but generally upward sloping, yet since December 2013, the trend is negative, showing a challenge linked to increased waiting time. The perspective of outpatients was included because these patients are the main focus and the customers who receive the direct medical service and have stronger responses. It is known that the main objective of every organisation is to produce products and services for customers to earn profit. These products or services are liable to maintain certain standards of quality to meet the expectations of customers. If quality is not met by a product or service, several negative results can appear which organisations have to face, such as customer retention, reputation, lawsuit, safety and value; hence it is important for organisations to produce their services qualitatively and serve in a pattern that can satisfy customers and increase this satisfaction.
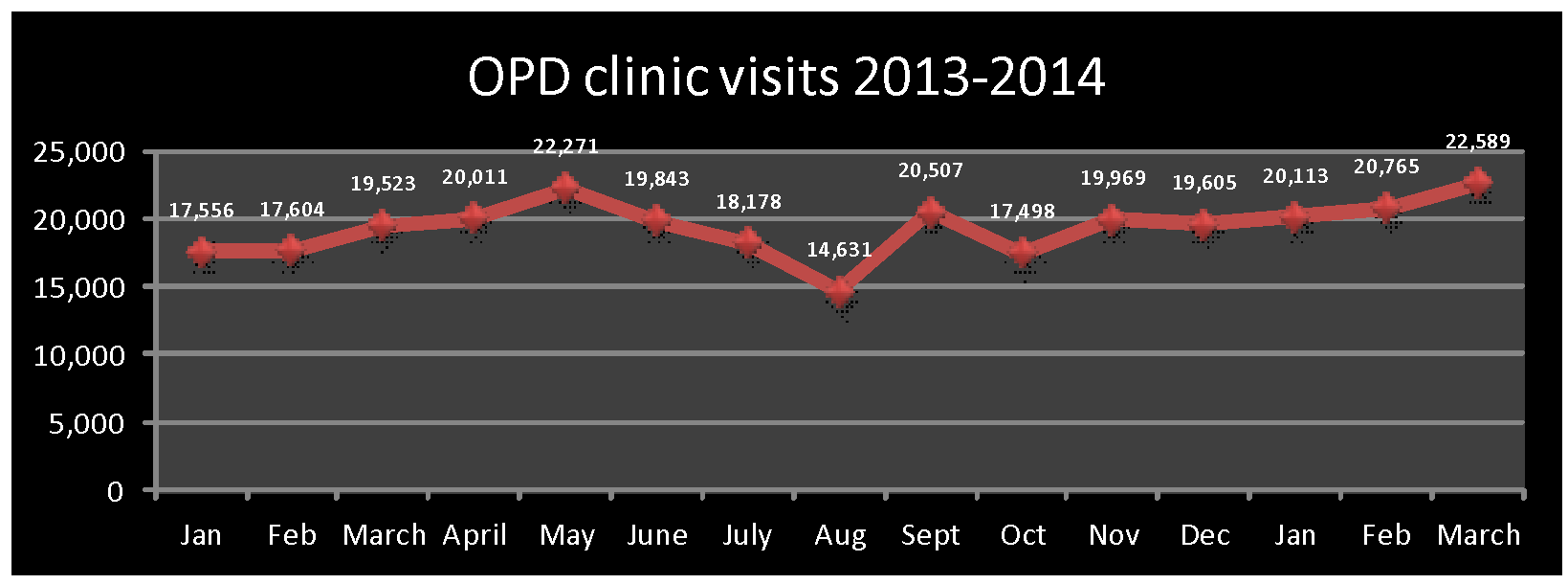
From the above chart, it is evident that the out-patient department witnessed an increase in patients January 2013 onwards. This trend continued until May 2013. June 2013 onwards, there was a decrease in the number of OPD patients till August 2013. After an increase in the month of September 2013, the number again decreased the next month. October 2013 onwards, the OPD department witnessed a steady but slow growth in the number of patient visits. The decline that was witnessed during the months of May 2013 to August 2013 might be due to some renovation work at the hospital.
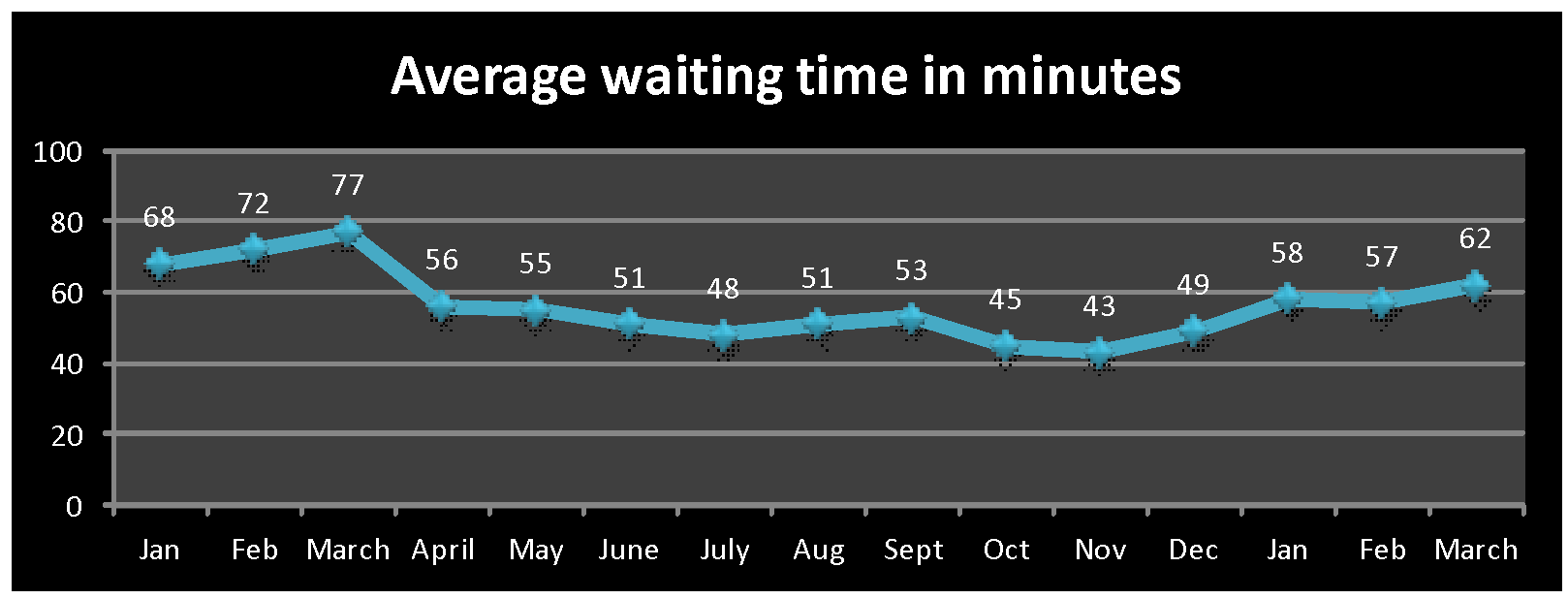
The above chart pertaining to the waiting time depicts that after a slight increase during the months of January 2013 to March 2013, the waiting time started decreasing. Except for a few instances of increase in the waiting time, it has decreased during most of the months. The hospital management is well aware of the importance of less waiting time for patient satisfaction. When, during January 2013 to March 2013, the management might have noticed the increase in waiting time, danger bells might have rung. It is quite possible that an urgent meeting might have been called for and this topic might have been discussed at length. A new strategy might have been adopted. Appropriate training to the staff might have been imparted. It is quite possible that as a result of these two actions, the waiting time started decreasing.
The above chart (of out-patient waiting time) depicts a reverse image of in-patient waiting time. This means that when the waiting time is more in the in-patient department, the employees are concentrating more on the out-patient department and vice-versa. This is not a good sign. This might have happened due to shortage of employees. The management needs to employ more staff to meet the patient demands.
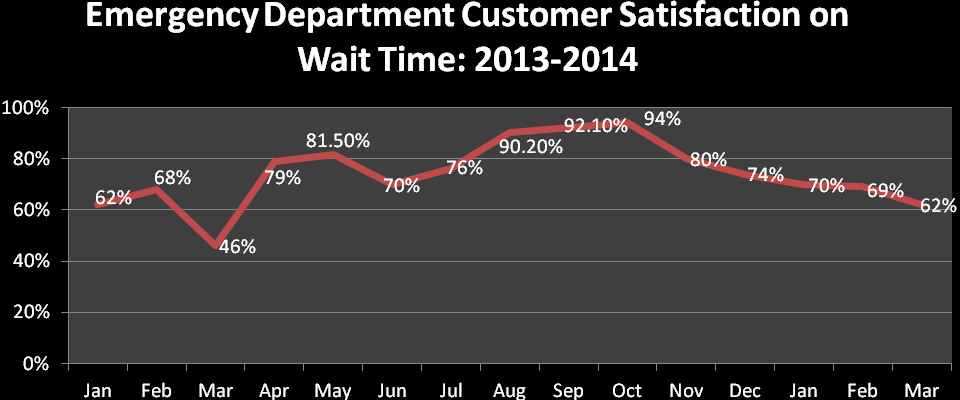
Analysis of service quality from the emergency patient perspective
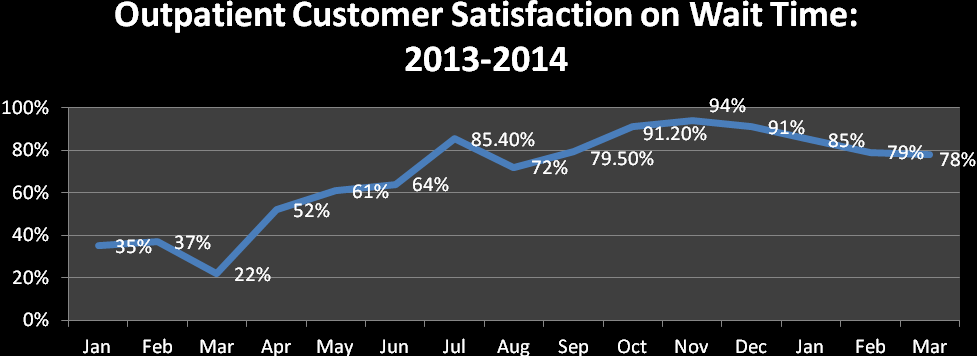
The lower acuity (Triage category T3-T5) patients in the emergency department (ED) were asked to rate the quality of customer service. In January 2013, satisfaction with wait time (from triage to seen by physician) was rated at 62% while in November 2013 it was rated at 94%, but it continued decreasing demonstrating an area for improvement in quality service. Ratings on quality were taken because quality maintains an important place in services. The perception of emergency patients regarding the quality of service judges the service equality as it is perceived by the patient and it may differ from the actual service delivered by the product. The actual service delivered by the organisation and actual service received by the customers may have a gap which needs to be filled with the help of service quality. However, service quality is defined as the degree of difference between the perceived service and expected service at the customer end. It is a social act that takes place in contact between representatives and customers of the service company.
It is found that customer service given by Al Mafraq hospital in the emergency department is decreasing as evidenced by unsatisfied customers.
During analysis in the ED, no correlation was found between actual waiting times and customer satisfaction. It was however found that customers do not understand that patients in triage categories T1-T2 require urgent attention and therefore “jump the queue”. Customers are facing several problems and have several options when they decide about a specific health care provider because of the hyper competitive market. Because of the availability of several options, quality and service are two important factors in the health care industry that influence the process of selection. From the above analysis, it is recommended that Mafraq hospital should enhance their quality of service provided by reducing wait time as waiting time is the main concern of customers and must be minimised to the maximum. Moreover, it is recommended that Mafraq hospital should focus on other aspects as well to meet quality standards.
Analyses of attempts by Mafraq hospital to improve wait times
Al Mafraq hospital appears to have focused all its energy on actually reducing wait times, which they perceived as the only factor to be prioritised. Some attempts in the pharmacy were piloted, but failed and hence abandoned. Other attempts in the Emergency department and Outpatient service were severely hampered by the restrictions of the physical space. Eventually there was agreement to invest in an expansion project, where a recently vacated building is currently being converted into an extended emergency service; i.e. for the less critical patients (T4-T5). The outpatient service is still exploring alternatives to its current patient flow and a high-level taskforce is addressing the matter. The challenge faced by the outpatient service, is that the volumes are constantly growing (Figure 4) and are expected to further rise, as the catchment area of the hospital is expanding rapidly, yet the new hospital that is being built as larger replacement facility will potentially only open in 2016. The company does not want to invest much in the current facility, as the future of the existing building is as yet undetermined. A different approach to managing wait time is thus required, i.e. managing customer perceptions of waiting time.
Examples
Mayo Clinic (United States)
Mayo clinic is a non-profit organisation engaged in health care services. It also imparts education to students from all over the world and has research facilities as well (Mayo Clinic 1). It has campuses at various locations throughout United States of America (in states such as Arizona, Minnesota and Florida). At Mayo Clinic, the requirements of patients are considered to be the first priority. Its mission is to motivate patients while providing excellent health care services. The organisation boasts of treat at least one million patients annually, from all over the world. It has almost 57, 700 employees and 3,450 students (Mayo Clinic 1). The missions and values of Mayo Clinic are based on respect, compassion, integrity, healing, teamwork, excellence, innovation, and stewardship.
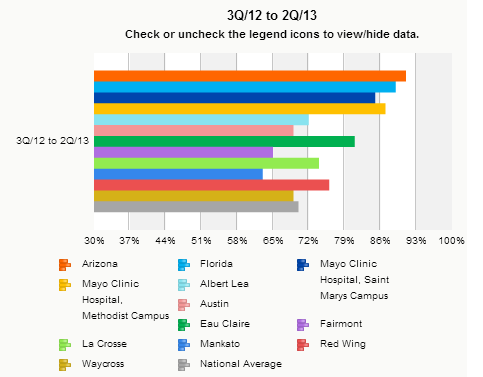
Mayo Clinic has a trend/practice of carrying out patient satisfaction surveys in order to measure its patient satisfaction level. This trend is being followed since the past couple of years. Such surveys assist the organisation in identifying the areas that lag behind in patient satisfaction and need special attention. In this manner, it can improve its health care and other related services. The following graph (19) depicts patient satisfaction rating of the inpatient department of Mayo Clinic at various locations during the period starting from third quarter of 2012 to second quarter of 2013. Various aspects were considered for the survey such as communication, diagnosis, ambience, noise level, post treatment guidance, etc.
As is evident from the graph, Arizona branch of Mayo Clinic has the highest patient satisfaction rating of 91 percent. Ratings for other branches are: Florida 89 percent, Saint Mary’s campus 85 percent, Methodist campus 87 percent, Albert Lee 72 percent, Austin 69 percent, Eau Claire 81 percent, Fairmont 65 percent, La Crosse 74 percent, Mankato 63 percent, Red Wing 76 percent, and Way Cross 69 percent. The national average rating of patient satisfaction for Mayo Clinic is 70 percent. The branches of Mayo Clinic that have a rating of less than 70% (Austin, Fairmont, Mankato, and Way Cross) need special attention. Arizona branch has a rating of 91 percent means that the organisation is capable of providing better services. The only thing required is better management at branches where the rating is low.
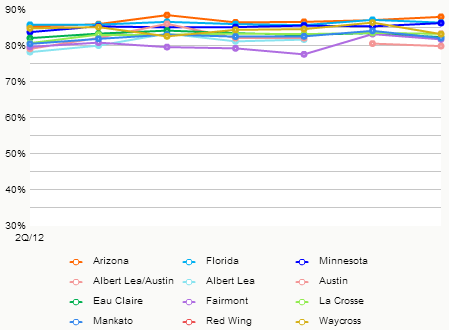
The following graph (20) represents patient satisfaction rating of out-patient department of Mayo Clinic at various locations for the fourth quarter of 2013. The ratings for different locations of Mayo Clinic were: Arizona 88.1 percent, Florida 86.5 percent, Minnesota 86.4 percent, Albert Lea / Austin 80 percent, Fairmont 81.9 percent, Mankato 82.2 percent, and Way Cross 83.3 percent. The percentage depicts the proportion of answers in “strongly agree”.
It is understood that adopting professionalism in any job gives better results. Similarly, in health care services also, professionalism is crucial to attain patient satisfaction. This rule is not only for the doctors and nurses, who come into direct contact with the patients, but also for those who work in the background (allied staff). At Mayo Clinic, importance is given to allied staff of health care. They are provided with the requisite training that enables them to understand customer behaviour and how to achieve customer satisfaction (Locke 1). Mayo Clinic has given training (“Please Care” training schedule) to almost 4,000 of its employees. After the training was completed successfully, the employees were advised to follow what they had learned. Almost 2,000 patients were requested to participate in a survey that was conducted twice (one before the employees took training and the other one after completion of training). It was noticed that while patient satisfaction rating was 71 percent before the employees took training, it increased to 77 percent after the employees took the requisite training (Locke 1). The survey questions included various aspects of health care services. In the survey conducted after the training, it was noticed that there was an improvement in most of the aspects. This proves that better professionalism can be helpful in achieving better ratings of patient satisfaction.
Bumrungrad International Hospital (Thailand)
Bumrungrad is a Thai word that means concern for the masses. There could not have been a better name other than this for Bumrungrad International Hospital that is one of the biggest health care centres in Southeast Asia. Almost one million patients (almost 40 percent are foreigners) are treated every year in this hospital. The popularity of the hospital is due to the fact that world-class treatment is offered at economic rates. Other plus-points of the hospital include less waiting time, outstanding services, and varied nature of treatments from normal check up to complex surgeries (Woodman 3).
According to Mack Banner, CEO of Bumrungrad International Hospital, the three main aims of the organisations are to please the patients, doctors & staff members and to continue its endeavour of adopting ways and means to provide better health care facilities and services (Woodman 4).
The hospital is engaged in meeting health care needs of foreign patients while arranging for those who accompany them. A special department named Medical Coordination Office (MCO) has been set up for the convenience of patients. Considering the importance of language in health care services, the hospital has a special arrangement for language translation. In addition, the hospital has branch offices in 13 nations to facilitate patients in taking appointments and arranging for the scheduled travel. Furthermore, in order to continue its endeavour of providing better services, the hospital has engaged Gallup (a renowned global research company) to conduct patient satisfaction surveys at frequent intervals of time. One of the recent surveys showed that almost 93% of foreign patients (who got treated at Bumrungrad International Hospital) were satisfied with the services being offered at the hospital (Woodman 32).
Joint Commission International (JCI) is a firm engaged in conducting surveys of hospitals for accreditation. Such a survey includes a varied set of aspects such as the hospital building, health care practices, staff behaviour, competence and experience, documentation, confidentiality, etc. A hospital having such accreditation can be considered to be the epitome in providing service to its patients. Bumrungrad International Hospital received this accreditation in the year 2002 (first in Asia) (Bumrungrad 4).
Bumrungrad International Hospital tries to be at par with global benchmarks of at least 60 health care indicators. The following table depicts some of the important indicators of the hospital in comparison to the corresponding global benchmarks.
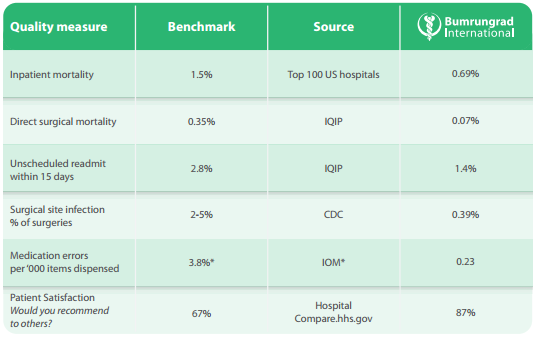
From the table at figure 21, it is evident that Bumrungrad International Hospital is within the limits of global benchmarks of various health care indicators. According to global benchmark, the in-patient mortality rate should be 1.5 percent, whereas it is 0.69 percent. This means that it is even less than the benchmark; it is far better than the global benchmark. Direct surgical mortality at the hospital is 0.07 percent as compared to the global benchmark of 0.35 percent; this again is far better. Similarly, indicators pertaining to unscheduled readmit within 15 days, surgical site infection % of surgeries, and medication errors per ‘000 items dispensed are less than their respective global benchmarks. Most encouraging is the fact that patient satisfaction at the hospital is 87 percent as compared to the global benchmark of 67 percent.
Cost is also a major deciding factor for patients while choosing a health care facility. Bumrungrad International Hospital has kept the rates of its services very economical. As compared to similar services in US and other countries, the prices at the hospital are very less. The difference in rates of such treatments is more than enough to take care of additional check-ups and treatments (Bumrungrad 6). The following table depicts a comparison of rates at Bumrungrad International Hospital and various hospitals in the US.
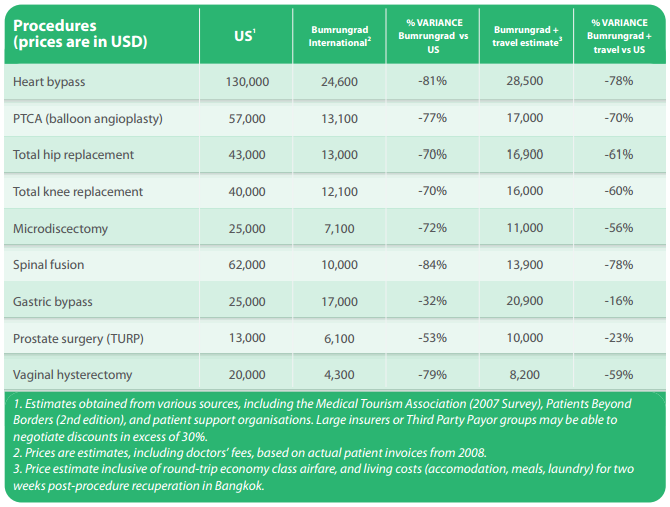
The above table depicts the difference in treatment rates of various surgeries. As is evident, in each case, even if the travel cost to Thailand is included, the total amount is still less than the treatment cost in the US. This is probably the reason why patients opt for Bumrungrad International Hospital. They are satisfied with the cost and the quality services (of global standards).
Features of health care service in Abu Dhabi
Demographics
Population: Likewise other emirates of United Arab Emirates, Abu Dhabi’s population also consists mainly of expatriates. Only 20 percent of the total population are locals. The local population is a young lot with almost 33% locals under 30 years of age. Among the expatriates, males dominate the numbers and are mostly between 20 to 40 years. Most of the expatriates are employed with construction companies and reside in camps erected at various sites. In the year 2006, health insurance was made mandatory for all the residents of the emirate. The expatriates are given health insurance cover by their employees, whereas the locals’ health insurance is taken care by HAAD.
Birth: It is unfortunate to note that during the past 30 years, Abu Dhabi’s fertility rate has declined considerably. Between 1990 and 2010 alone, this rate has decreased by 2.7 percent. “Declining birth rates are attributes to urbanisation, delayed marriage, changing attitudes about family size, and increased education and work opportunities for women” (HAAD 5).
Death: There has been a substantial decrease in the death rates as well. This is a good sign and a proof of better health care services in the emirate. In terms of infant death rate, Abu Dhabi is now at par with most of the developed countries. According to a report of World Health Organisation, the death rate of children (less than 5 years) has gone down by 15 percent (1990 – 2010).
Injuries: Since the roads in Abu Dhabi have been constructed using the latest technology and the best of material, driving has become a pleasure. But some people, mostly the youngsters, make wrong use of these beautiful roads. They engage in street and road races that end up in accidents and subsequent injuries to the driver and the passengers. Road accidents account for more than 10 percent of the total deaths in Abu Dhabi.
Non-contagious diseases: As a result of changed life style residents of Abu Dhabi have become prone to various chronic diseases. Heart-related diseases are also on the rise; in 2012, one-fourth of total deaths were due to some or the other heart related problem.
Cancer: In 2012, cancer was the reason for at least 13.9 percent of deaths in Abu Dhabi. The two kinds of cancer that are common among UAE residents are Lymphoid and Haematopoietic. Among females, breast cancer is more prevalent.
Contagious diseases: As a result of timely inoculation of children instances of contagious diseases are very rare. Since Abu Dhabi has a large population of expatriates, they are tested for any contagious disease before issuing them residence visa.
Respiratory infections: This is one of the most commonly found problems among residents of Abu Dhabi. It affects the productivity of work.
Private and public health care services in Abu Dhabi
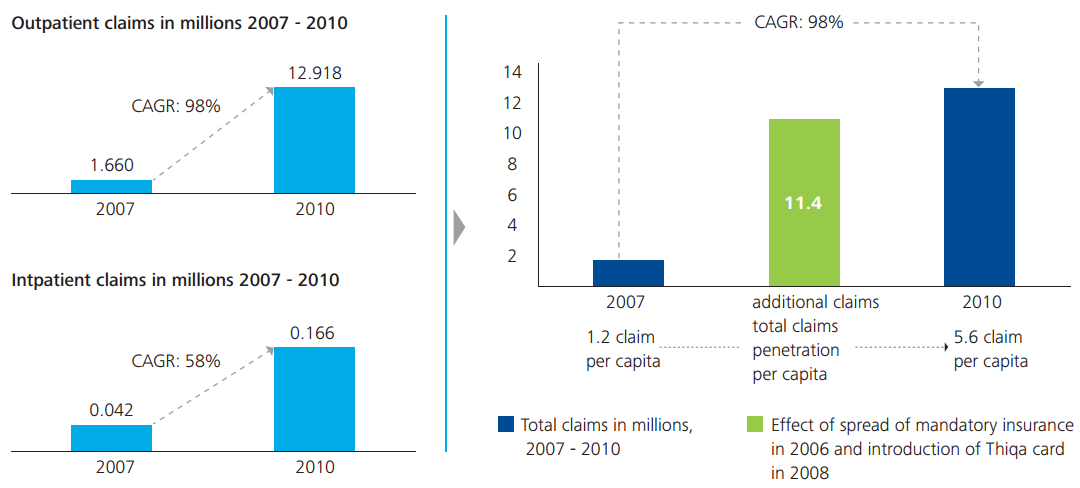
There was a time when most of the Gulf nations provided free health insurance coverage to the locals. Over the years, the declining economic conditions and growing costs of health care services have made health care a costly affair. Governments of most of these nations find it difficult to sustain such costs and as such, many Gulf nations have been compelled to shift to private health care services. Abu Dhabi is considered to be the pioneer (within the gulf region) in providing health care services. Even in Abu Dhabi, private health care providers are being promoted in order to maintain a balance in the growth of both the sectors (private and public). The growing cost of health care services can be gauged from the fact that from 2007 to 2010, health insurance claims increased at least 7.75 times. The following graph depicts the details.
Further, the following figures depicts the benchmark of health care spending by different Gulf nations (figure 24) and the per capita health care expenditure in the UAE (figure 25).
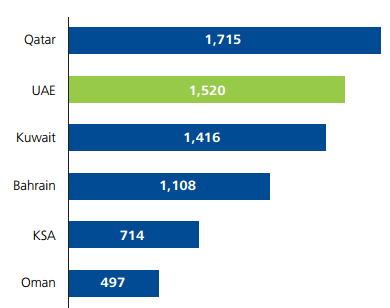
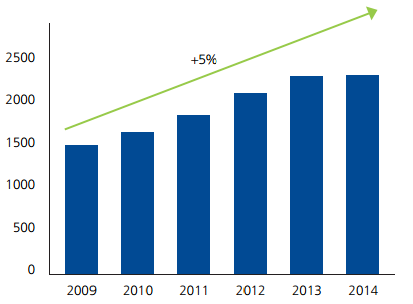
As is evident from figure 24, UAE stands at second position in per capita spending on health care services. Figure 25 shows that the per capita spending on health care is increasing at a steady pace of 5 percent (average). In terms of per capita spending on health care services, UAE ranks 20 among the global nations (Deloitte 7). The increase is largely due to the changed lifestyle (and the accompanying chronic diseases), increased income, low inflation, increasing population of aged people, and a fairly large budget allocation to health care.
The aim behind promoting private health care services is similar to that of Thailand; making Abu Dhabi a destination for medical tourism. Another reason for the promotion of private health care services is the fact that recent years have witnessed growing number of cases of heart-related ailments, diabetes and cancer. This has resulted in excess work load for nurses and other health care professionals.
SEHA Company
The Abu Dhabi Health Services Company, also known as SEHA, was formed in the year 2007 under decree number 10. It is a ‘joint stock company’ of Abu Dhabi government. It owns the health care facilities within the emirate. It acts as the executor of HAAD’s policies pertaining to health care in Abu Dhabi. The company also owns several ambulatory services. It has teamed up with renowned global health care companies such as Johns Hopkins Medical, Cleveland Clinic and Vienna Medical University.
Abu Dhabi’s health insurance law
Abu Dhabi has a new health insurance law, the objectives of which are as under:
- To promote a well-organised and economical health insurance service.
- To safeguard the interests of the people who opt for insurance.
- To warrant appropriate use of insurance premium amount.
- To foster the wellbeing of the people who opt for insurance.
- To ensure optimum health care for people who opt for insurance.
- To make available options for patients.
Provisions during emergency situations
As per the provisions of the new health insurance law, an approved health care service provider has to give suitable treatment to an injured person (emergency cases), irrespective of the injured person’s insurance coverage. The treatment charges can be recovered at a later stage from the insurance provider (if insured) or from the employer (if not insured). A special provision of the law omits injuries during work from insurance coverage. Such injuries come under the ‘Work Compensation Insurance’.
Bindings for employers
The new health insurance law makes it mandatory for all businesses to provide valid health insurance to their employees and their families (spouse plus three kids who should be less than 18 years of age). Such insurance coverage should include all the related charges. Renewals of expatriate visas and work permits will not be done unless the applications are accompanied with valid insurance policies.
Employers are forbidden to recover the insurance cost from their employees. If any employer violates this provision, suitable action will be taken against the business.
Insurance policy features
All insurance policies have a validity of a single year and are required to be renewed on a yearly basis. It is possible to opt for another insurance provider even if the previous policy has not expired. In such cases, the insurer has to bear the extra amount (difference in premium).
HAAD
The health care scenario in Abu Dhabi is controlled by the Health Authority of Abu Dhabi (HAAD). HAAD shoulders the responsibility of providing best possible medical facilities to the residents of Abu Dhabi. It formulates the strategy and policy pertaining to health care system; evaluation of the system is carried out at regular intervals. It also promotes the use of latest technology in health care field.
HAAD’s vision
“The system is driven towards excellence through continuous improvement and monitored for achievement of targets” (HAAD 1).
HAAD’s mission
“Ensure reliable excellence in health care for the community” (HAAD 1).
HAAD’s values comprise of commitment to the community, pursuit of excellence and continuous improvement, respect and compassion, integrity, accountability, and collective wisdom of teamwork & collaboration. HAAD recognises its accountability to the society and is devoted to cultivate a habit of maintaining good health, avert poor health and encourage the growth of programs and services suitable for the society. It is also committed to make available the best possible health care facilities for the patients. The main motto followed by HAAD is that everyone has his/her own dignity and they need to be treated with respect. Appropriate attention and preference is given to people and the society. HAAD observes a regular reporting system so that the stakeholders are aware of the happenings in the health care system. Team work and proper communication are given utmost importance because without these two, appropriate services cannot be rendered to patients.
Conclusion
Considering the increasing demand for health care services and the growing number of international companies entering into this field, it has become important for such facilities to adopt better patient services. Patient satisfaction has become of great importance in the popularity of health care centres. Various factors contribute towards better patient satisfaction. These include, and are not limited to, better and innovative technologies, courteous and knowledgeable staff, and better services (less waiting time, cleanliness, less noise pollution, etc.). Word of mouth publicity plays a crucial part in augmenting the image of health care centres. With government of Abu Dhabi having started to promote private sector participation in the health care sector, patient satisfaction becomes all the more crucial. The future of health care sector is quite encouraging. This is supported by various surveys that show an increase in spending on health care sector. Increased incomes and mandatory insurance coverage have made the locals of Abu Dhabi to use health care facilities more frequently.
The government of Abu Dhabi is committed to provide the best possible health care facilities to its residents (locals as well as expatriates). In pursuance of its endeavour, the government has formulated new health policy that makes it mandatory for all businesses to provide health insurance to their employees and their families 9with certain conditions). Insurance coverage of locals is taken care of by the government itself. According to the provisions of the new law, no health care centre can deny treatment to emergency patients, irrespective of their insurance coverage. The expenses of treatment can be recovered from the concerned parties once the treatment is over or at least started.
Appendix 1
Works Cited
Bardhan, Indranil and Mark Thouin. “Health information technology and its impact on the quality and cost of healthcare delivery.” Decision Support Systems 55.2 (2013): 438-449. Print.
Bumrungrad 2008, Choosing an International Hospital. Web.
Deloitte 2011, 2011 Survey of the UAE Healthcare Sector: Opportunities and Challenges for Private Providers. PDF file. Web.
Edwards, Jennifer 2009, Parkwest Medical Centre: Focusing on Patient and Staff Satisfaction. Web.
Galewitz, Phil 2012, Urgent Care Centers Are Booming, Which Worries Some Doctors. Web.
GRMC 2011, Patient Satisfaction Survey – Al Mafraq Hospital. Web.
HAAD 2014, Vision. Web.
Halogen Software 2008, The Influence of Employee Satisfaction on Patient Satisfaction and Safety. Web.
Japsen, Bruce 2013, A Boom In Urgent Care Centers As Entitlement Cuts Loom. Web.
Jeffreys, Marianne. Teaching Cultural Competence in Nursing and Health Care: 2nd Edition, New York: Springer Publishing Company, 2010. Print.
Korzep, Karen. “The future of technology and the effect it may have on replacing human jobs.” Technology & Health Care 18.4 (2010): 353-358. Print.
Landen, Rachel 2013, Study says urgent-care centres filling void. Web.
Larson, Jennifer 2012, The Connection Between Employee Satisfaction and Patient Satisfaction. Web.
Locke, Richard 2007, Professionalism among Allied Health Staff. Web.
Margolis, Stephen, Sumayya Al-Marzouqi, Tony Revel and Richard Reed. “Patient Satisfaction with Primary Health Care Services in the United Arab Emirates.” International Journal for Quality in Health Care 15.3 (2003): 241-249. Print.
Mayo Clinic 2014, About Mayo Clinic. Web.
Mossberger, Marcus 2014, The Relationship Between Employee Satisfaction and Hospital Patient Experience. Web.
Peltier, Jimmy and Andy Dahl 2009, The Relation Between Employee Satisfaction and Hospital Patient Experiences. PDF file. Web.
Powell, Linda 2001, Patient Satisfaction Surveys for Critical Access Hospitals. PDF file. Web.
Sharma, Suresh and Pawan Kamra. “Patient Satisfaction with Nursing Care in Public and Private Hospitals.” Nursing and Midwifery Research Journal 9.3 (2013): 130-141. Print.
Silow-Carroll, Sharon 2008, Munson Medical Centre: Constant Focus on Patient Satisfaction. Web.
SKMC 2014, Healthcare in Abu Dhabi. Web.
Slowiak, Julie, Bradley Huitema and Alyce Dickinson. “Reducing Wait Time in a Hospital Pharmacy to Promote Customer Service.” Q Manage Health Care 17.2 (2008): 112–127. Print.
Torcson, Patrick 2005, Patient Satisfaction: The Hospitalist’s Role. PDF file. Web.
White, Brandi. “Measuring Patient Satisfaction: How to Do It and Why to Bother.” Family Practice Management 6.1 (1999): 40-44. Print.
Woodman, Josef 2012, Bumrungrad International Hospital. PDF file. Web.